- The paper introduces a composite loss and factorial perturbation strategy to calibrate verbalized uncertainty in Medical VQA.
- The methodology significantly reduces calibration error—up to 60% reduction in ECE—and maintains answer accuracy across diverse benchmarks.
- This approach enhances clinical safety by enabling model abstention under uncertainty and better error detection in high-stakes scenarios.
Improving Verbalized Uncertainty Calibration in Medical VQA: A Detailed Analysis
Introduction and Motivation
The transition from opaque, black-box medical AI models to interpretable multimodal LLMs (MLLMs) has increased interest in models capable of explaining both their reasoning and the confidence underlying their predictions. In Medical Visual Question Answering (VQA), this capacity is crucial: MLLMs frequently exhibit overconfident outputs, unaffected by the correctness of their answer, undermining their clinical reliability and safety. Current approaches to verbalized confidence calibration are optimized for unimodal (text-only) LLMs, neglecting the complexities introduced by multimodal data, particularly in high-stakes medical applications.
This paper presents a comprehensive training-based calibration framework for verbalized uncertainty in Medical VQA, addressing the aforementioned limitations. The approach introduces a (i) 2×2 factorial perturbation scheme to probe modality reliance, (ii) a composite loss function incorporating Brier-style calibration, a conservative anchor term, a contrastive alignment component, and a top-k KL divergence regularizer, and (iii) an extensive evaluation across accuracy regimes and model architectures—specifically MedGemma-4B-IT and Qwen2-VL-7B-Instruct. The method achieves substantial improvements in calibration error, discrimination, and practical clinical utility across three benchmarks.
Methodological Contributions
Factorial Perturbation for Multimodal Reliance
Properly calibrated confidence should reflect the evidence sources actually utilized in each prediction. To achieve this, the paper leverages a factorial design (Figure 1), orthogonally perturbing both image and text inputs: images can be original or entirely replaced (black image for evidence removal), while answer options can be original or textually perturbed (randomized/shuffled distractors). This results in four distinct input configurations per question and enables direct measurement of how model confidence and accuracy change when either modality's evidential value is ablated.
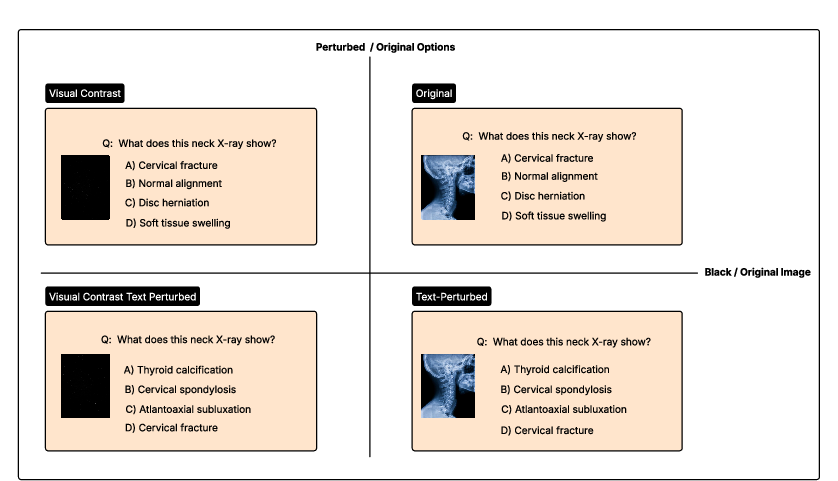
Figure 1: The 2×2 factorial perturbation design illustrated on a cervical X-ray example from OmniMedVQA.
Composite Loss for Calibration and Robustness
The training objective is formed as a weighted sum of four terms:
- Tokenwise Brier loss: Ensures per-sample predicted confidence matches empirical correctness, using fractional accuracy targets estimated by repeated sampling.
- Anchor loss: Penalizes deviations from maximal epistemic uncertainty (scale midpoint), preventing collapse to artificially high or low confidence.
- Contrastive alignment loss: Aligns inter-condition confidence differentials to match empirically measured performance differentials across the factorial perturbation axes, enforcing sensitivity to available evidence.
- Top-k KL divergence regularizer: Anchors answer token distributions to those of a frozen base model, constraining catastrophic forgetting and preserving answer accuracy and response format.
This loss is optimized via LoRA fine-tuning, with all components necessary for optimal calibration, as confirmed by ablation.
Experimental Evaluation
Benchmarking and Quantitative Results
The framework is evaluated on three Medical VQA datasets representing distinct accuracy regimes:
- OmniMedVQA: High accuracy (in-distribution).
- PMC-VQA: Intermediate accuracy (out-of-distribution).
- MedXpertQA: Low accuracy, high difficulty (out-of-distribution).
Two model architectures are used: MedGemma-4B-IT and Qwen2-VL-7B-Instruct. The method is benchmarked against the base model, prompt/sampling aggregations (Top-K Sampling, SteerConf), and the text-only fine-tuning strategy ConfTuner.
Strong quantitative findings are reported: reductions in Expected Calibration Error (ECE) by at least 60%, consistent Brier Score improvement (26–43% reductions on MedGemma per-benchmark, 3–18% on Qwen2-VL), and superior AUROC in multiple settings. Importantly, answer accuracy is not sacrificed, and calibration/discrimination improvements persist under distribution shift (cross-benchmark evaluation).
Calibration–Discrimination Tradeoff
While prior baselines achieve superficially low ECE by collapsing predictions near the dataset mean (thus failing to discriminate between correct/incorrect samples), the proposed approach achieves a larger separation of confidence distributions (Figure 2), reflected in higher AUROC and a lower overlap coefficient between correct and incorrect predictions.
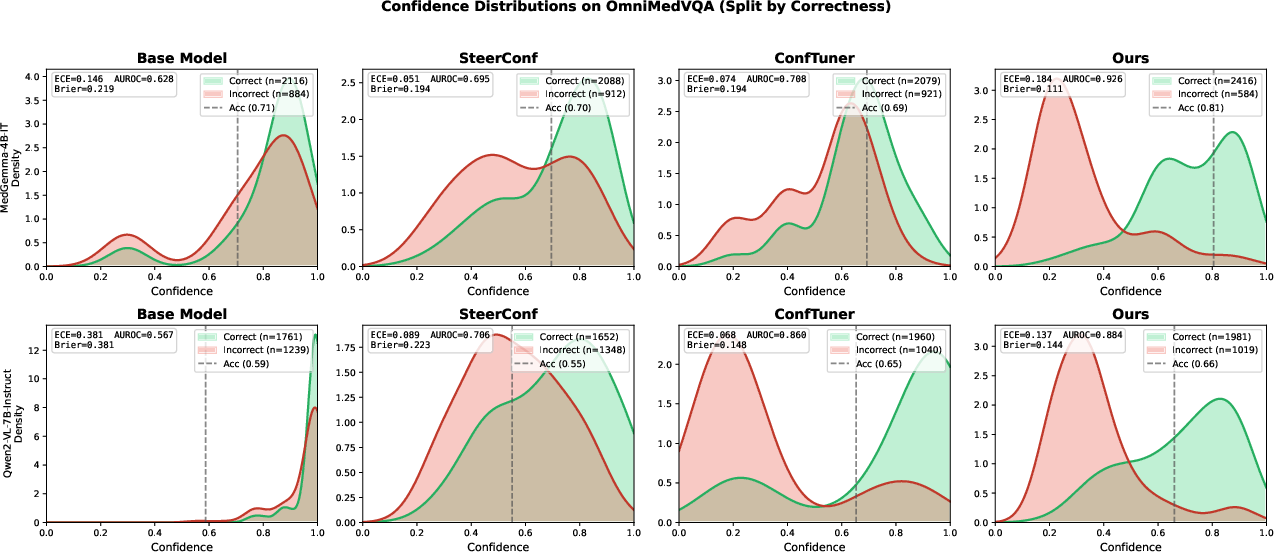
Figure 2: Confidence distributions on OmniMedVQA, split by correctness (top: MedGemma, bottom: Qwen2-VL). Baselines cluster around dataset accuracy (dashed line), overlapping correct and incorrect samples. The proposed method separates correct from incorrect, yielding higher AUROC.
This adaptivity holds across datasets: while baselines provide indiscriminately high confidence even as accuracy degrades (Figures 6–8), the new method's confidence adapts, tracking empirical performance across varying difficulty (Figure 3).
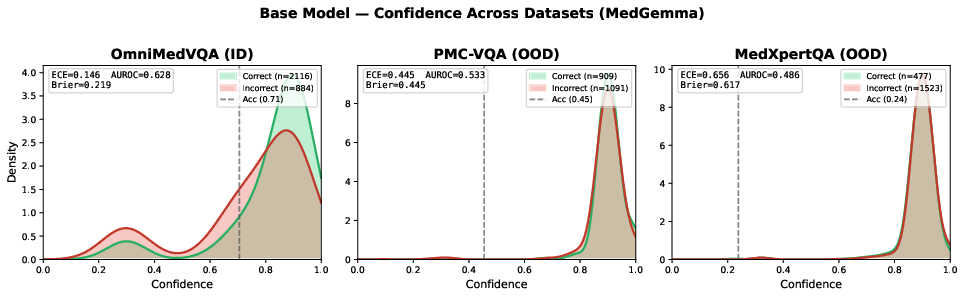
Figure 4: Base Model confidence distributions across datasets (MedGemma). The distribution remains concentrated at high confidence regardless of dataset accuracy.
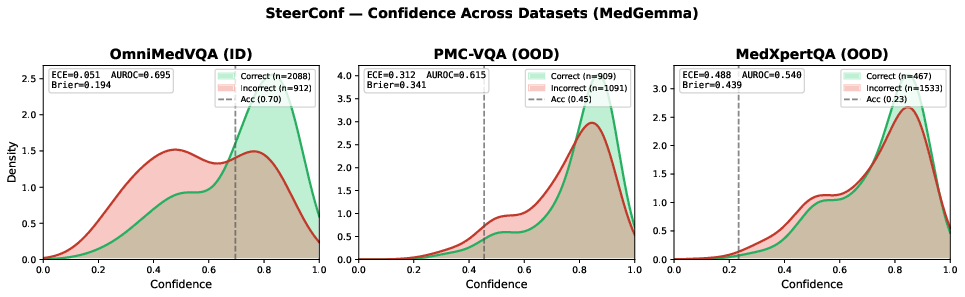
Figure 5: SteerConf confidence distributions across datasets (MedGemma). The distribution shape remains unchanged despite significant accuracy drop.
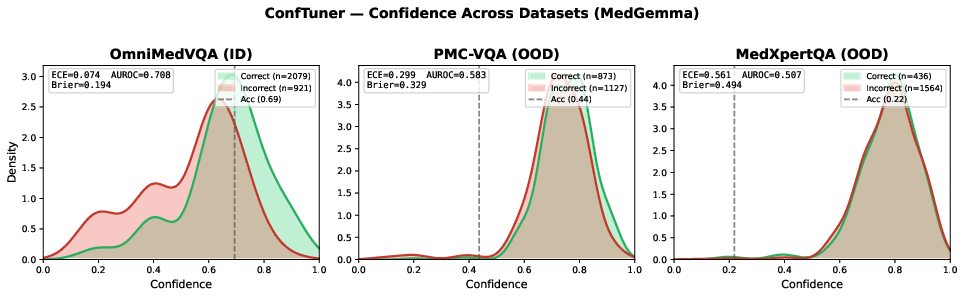
Figure 6: ConfTuner confidence distributions across datasets (MedGemma). Confidence remains high even on challenging datasets.
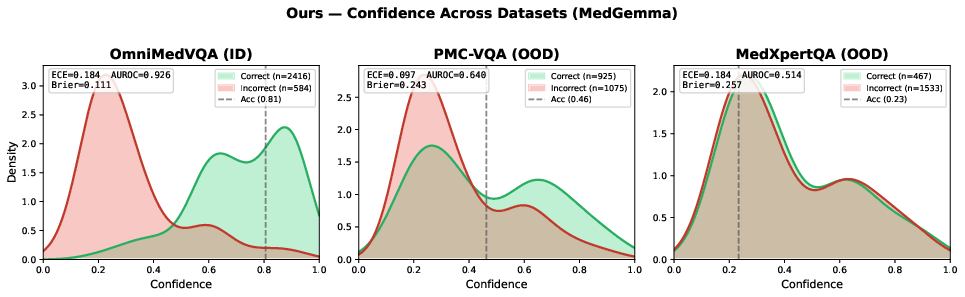
Figure 3: Proposed method's confidence distributions (MedGemma). Confidence tracks dataset difficulty: high on OmniMedVQA, moderate on PMC-VQA, low on MedXpertQA. Correct and incorrect predictions are well-separated except at the discrimination limit (MedXpertQA).
Practical and Clinical Utility
In clinical simulation experiments, the calibrated model abstains from recommendations when uncertain, reducing the number of wrong recommendations per 100 patients, especially in challenging out-of-distribution scenarios (Figure 7). Baseline models issue recommendations even when performance is at random chance, exposing clinicians to excessive incorrect suggestions.
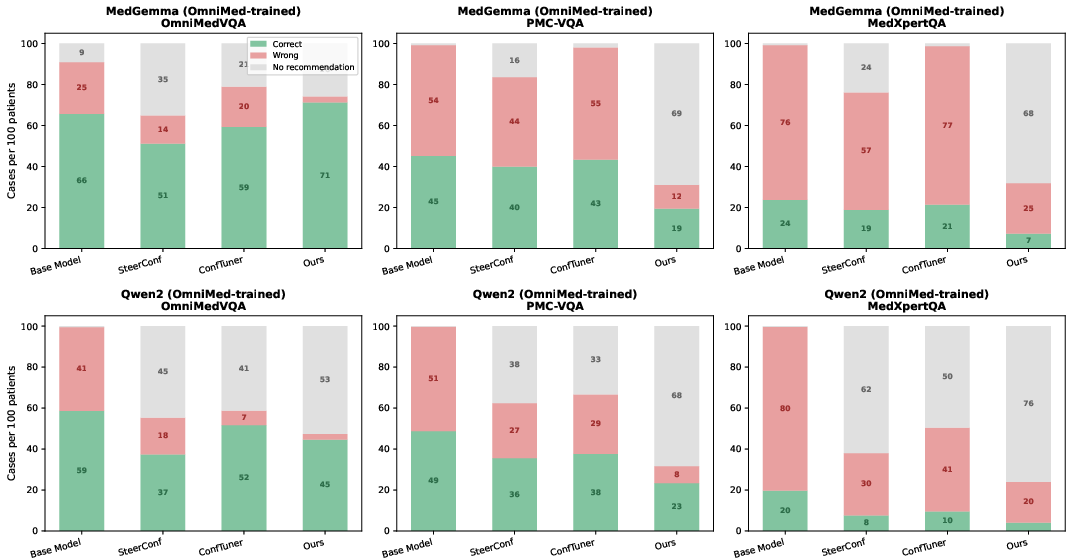
Figure 7: Recommendation outcomes per 100 patients at confidence threshold 6. The proposed method abstains when uncertain, reducing wrong recommendations compared to baselines.
Further, the error catch rate as a function of confidence threshold demonstrates that the proposed framework flags a higher proportion of true errors for review across a wide threshold range, enhancing the potential for human-in-the-loop clinical safety (Figure 8).
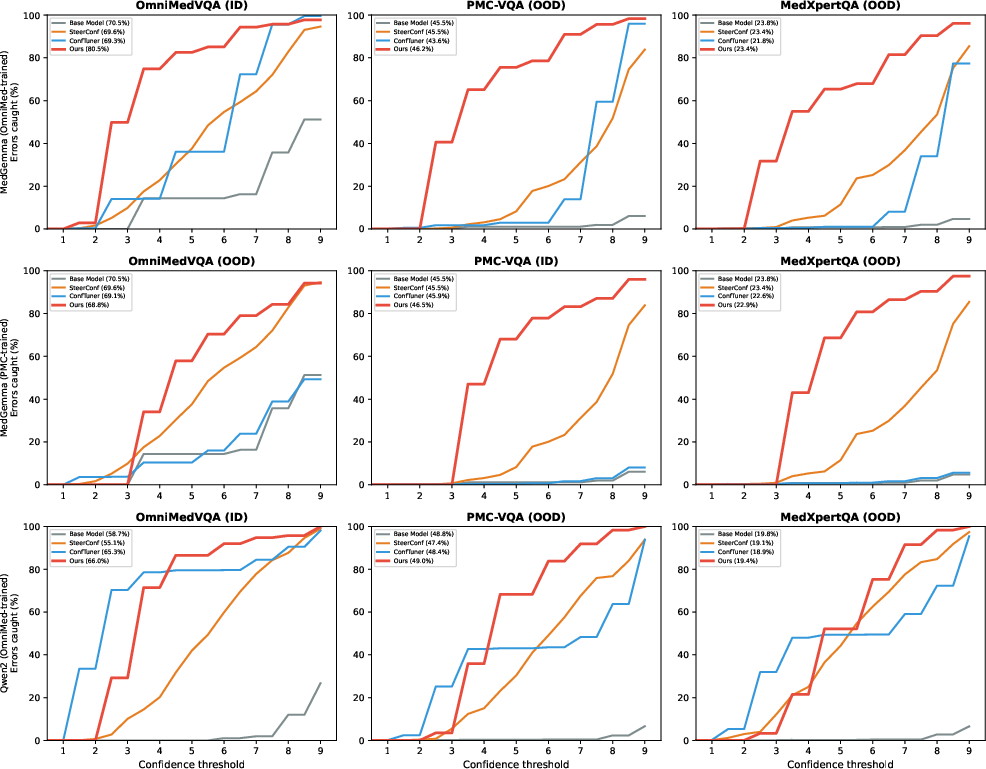
Figure 8: Error catch rate versus confidence threshold. The calibrated model captures a greater fraction of errors across thresholds in both in- and out-of-distribution evaluation.
Implications and Directions for Future Research
This work demonstrates that calibration of verbalized confidence in multimodal VQA can be robustly achieved by incorporating explicit perturbation-driven alignment signals, a conservative anchor prior, and strict answer preservation via top-k KL regularization. Practical implications include enabling threshold-based abstention/triage, improving downstream decision support efficiency, and increasing deployment readiness for MLLMs in safety-critical clinical workflows.
A notable finding is the failure of all methods, including the proposed one, to achieve meaningful discrimination at the most challenging regime (MedXpertQA), suggesting that as base accuracy approaches chance, reliable confidence estimation is inherently limited. This brings into focus open questions around scaling: whether larger architectures or open-ended answer spaces will preserve calibration gains, and whether future loss designs might integrate alignment and anchoring properties as intrinsic, not auxiliary, aspects of the calibration objective.
Conclusion
By combining factorial input perturbations with a novel composite loss, this paper establishes that MLLMs can be trained to express well-calibrated verbalized uncertainty in Medical VQA. Robustness to distribution shift and practical deployment benefits are verified across datasets and architectures, and each loss component's necessity is empirically validated. The framework currently operates in a multiple-choice regime and moderately sized models, and the generalization of these findings to large-scale open-ended medical reasoning remains a critical direction for further study. Properly calibrated uncertainty is required for safe AI clinical deployment; this work provides a rigorous, effective method for achieving it in the current generation of MLLMs.
References
Senoglu, E., Toschi, F., Brunello, N., Sassella, A., & Carman, M. J. "Just how sure are you? Improving Verbalized Uncertainty Calibration in Medical VQA" (2606.27023).

