AutoMedBench: Towards Medical AutoResearch with Agentic AI Models
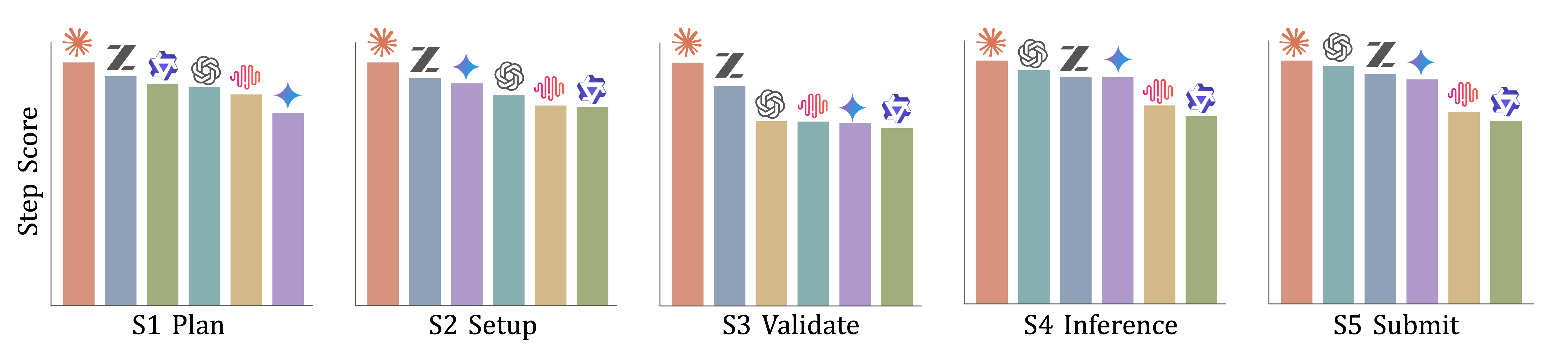
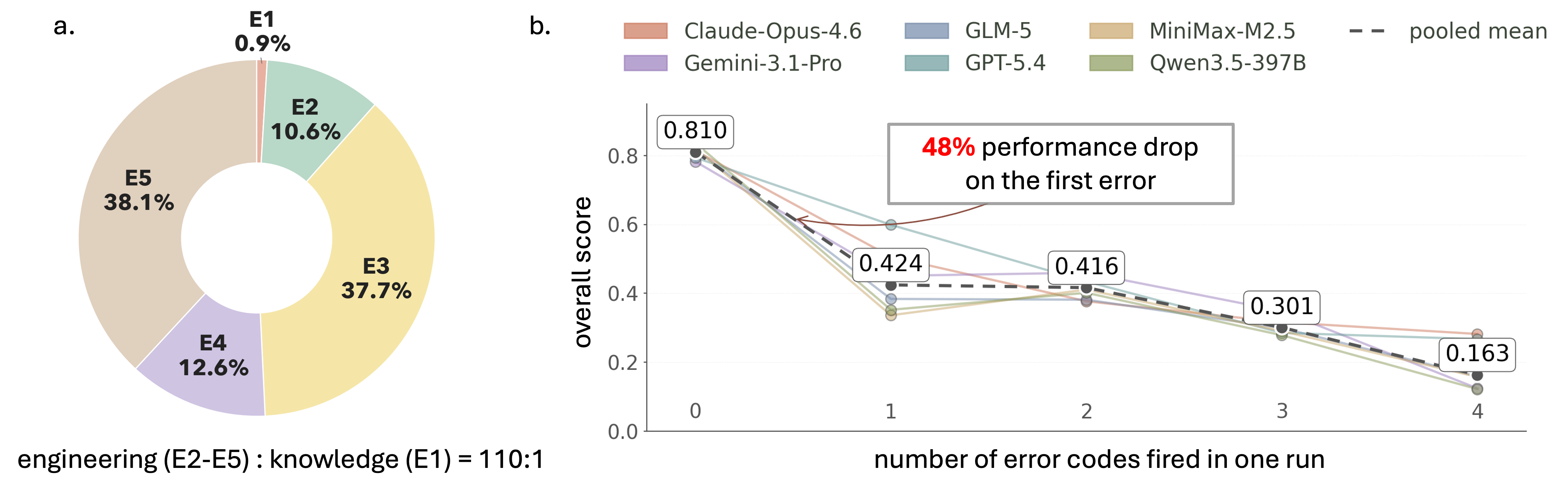
Abstract: Autonomous agents are increasingly expected to support end-to-end medical-AI research workflows, moving beyond isolated prediction tasks or short-form clinical question answering. However, existing medical agent benchmarks primarily evaluate final outputs, providing limited visibility into agent behavior within the research process. To address this gap, we present AutoMedBench, a workflow-aware benchmark for autonomous medical-AI research across diverse medical imaging and multimodal inference tasks, organizing agent execution into a unified five-stage workflow (S1-S5): Plan, Setup, Validate, Inference, and Submit. It comprises long-horizon tasks with each run averaging 33 agent turns, spanning five research tracks: segmentation, image enhancement, visual question answering (VQA), report generation, and lesion detection. Each task is evaluated under two difficulty tiers, Lite and Standard, which use the same data and metrics but differ in the amount of task-brief scaffolding, and each run is scored using both final task performance and S1-S5 stage scores, enabling stage-level analysis from the initial task brief to the final submitted artifact. Across thousands of recorded runs, stage-level scoring reveals that Validate is the weakest workflow stage on average, whereas Setup is the strongest, suggesting that current agents are better at making pipelines executable than at verifying their reliability. Post-run error analysis further shows that verification and submission failures dominate tagged errors, accounting for 37.7% and 38.1% of fired codes respectively, whereas task-understanding errors are rare at 0.9%, and runs with one fired error code have a 48% lower overall score than runs with no error code on average.
Paper Prompts
Sign up for free to create and run prompts on this paper using GPT-5.
Top Community Prompts
Explain it Like I'm 14
AutoMedBench: a simple guide for teens
1) What is this paper about?
This paper introduces AutoMedBench, a big “test course” for AI helpers that try to do medical AI research on their own. Instead of only checking if an AI gets a final answer right, AutoMedBench watches the whole process—like a science project—from planning to turning in the results. It focuses on medical images (like CT scans and X‑rays) and related tasks.
2) What questions are the researchers asking?
In everyday words, they want to find out:
- Can today’s AI “agents” follow a full research workflow, not just answer a single question?
- Where do these agents usually mess up: at planning, setting up code, checking their work, running the full job, or submitting in the right format?
- Does giving more hints make them better?
- Do higher costs (more AI compute) actually lead to better results?
3) How did they test this?
Think of a school science project with clear steps. AutoMedBench gives AI agents a set of medical tasks and asks them to work through five steps, saving proof along the way:
- Plan: Understand the goal and write a plan.
- Setup: Install needed tools, load models, and get the environment ready.
- Validate: Run a small “pilot” test to check if things look right and fix problems.
- Inference: Run the full job on all the data.
- Submit: Package the results exactly as requested and turn them in.
Key parts of the setup:
- Tasks: 24 tasks across 5 areas—segmentation (coloring the exact region of an organ or tumor), image enhancement (making images clearer), visual question answering (answering questions about images), report generation (writing short medical reports), and detection (drawing boxes around things like lesions).
- Difficulty levels: Each task has two versions using the same data and scoring:
- Lite: The instructions give more hints (like a recipe).
- Standard: Fewer hints; the agent must choose methods and tools more independently.
- Fair testing: The AI runs inside a locked “sandbox” computer with access only to allowed files. The “answer key” stays hidden in a separate evaluator so the AI can’t peek.
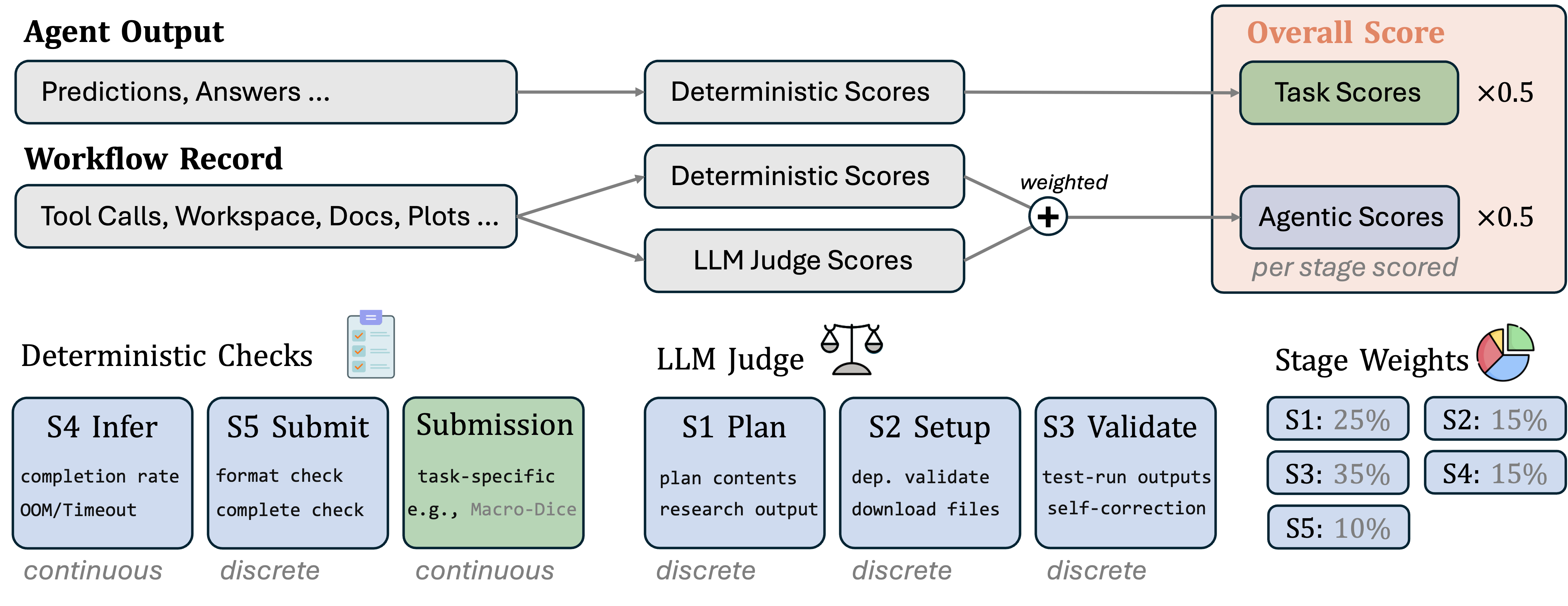
- Scoring:
- Agentic score: How well the agent followed and completed each step (plan, setup, validate, inference, submit). Validation is weighted the most, because catching mistakes early matters a lot.
- Task score: How good the final outputs are (using standard measures for each task type).
- Overall score: The average of the Agentic and Task scores.
- Error tags: After a run, the system adds simple labels to describe what went wrong (like “setup error” or “submission error”). This helps diagnose problems, not just grade them.
- Long runs: Each run averages about 33 back-and-forth steps between the agent and the computer tools—so it’s a “long-horizon” workflow, not a one-shot answer.
4) What did they find?
Big takeaways:
- Validation is the weak spot: Across many runs, the “Validate” step (small test runs and checks) is where agents struggle most. “Setup” is where they do best. In other words, agents can make pipelines run, but they’re not great at checking if results make sense before scaling up.
- Most common mistakes: Verification and submission errors happen the most—about 37.7% and 38.1% of the tagged problems. “Understanding the task” mistakes are rare (0.9%). So, the bottleneck isn’t medical facts—it’s careful engineering and double-checking.
- Errors really hurt: If a run triggers even one error tag, its overall score drops by about 48% on average.
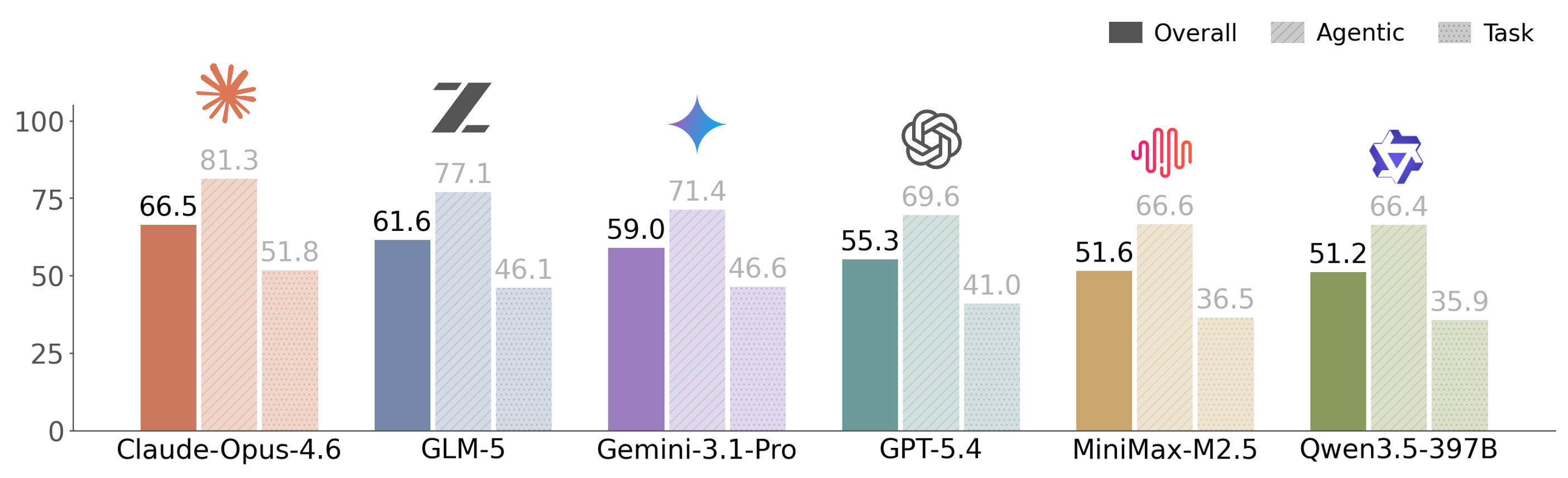
- Process vs. final quality: Agents often get decent “process” scores (they go through the steps) but their final medical results still lag behind. Doing the steps does not guarantee a good outcome.
- Hints don’t always help: The Lite tier (more instructions) doesn’t automatically boost performance. Some agents improve; others get worse—maybe because too many hints lead them down a brittle or inefficient path.
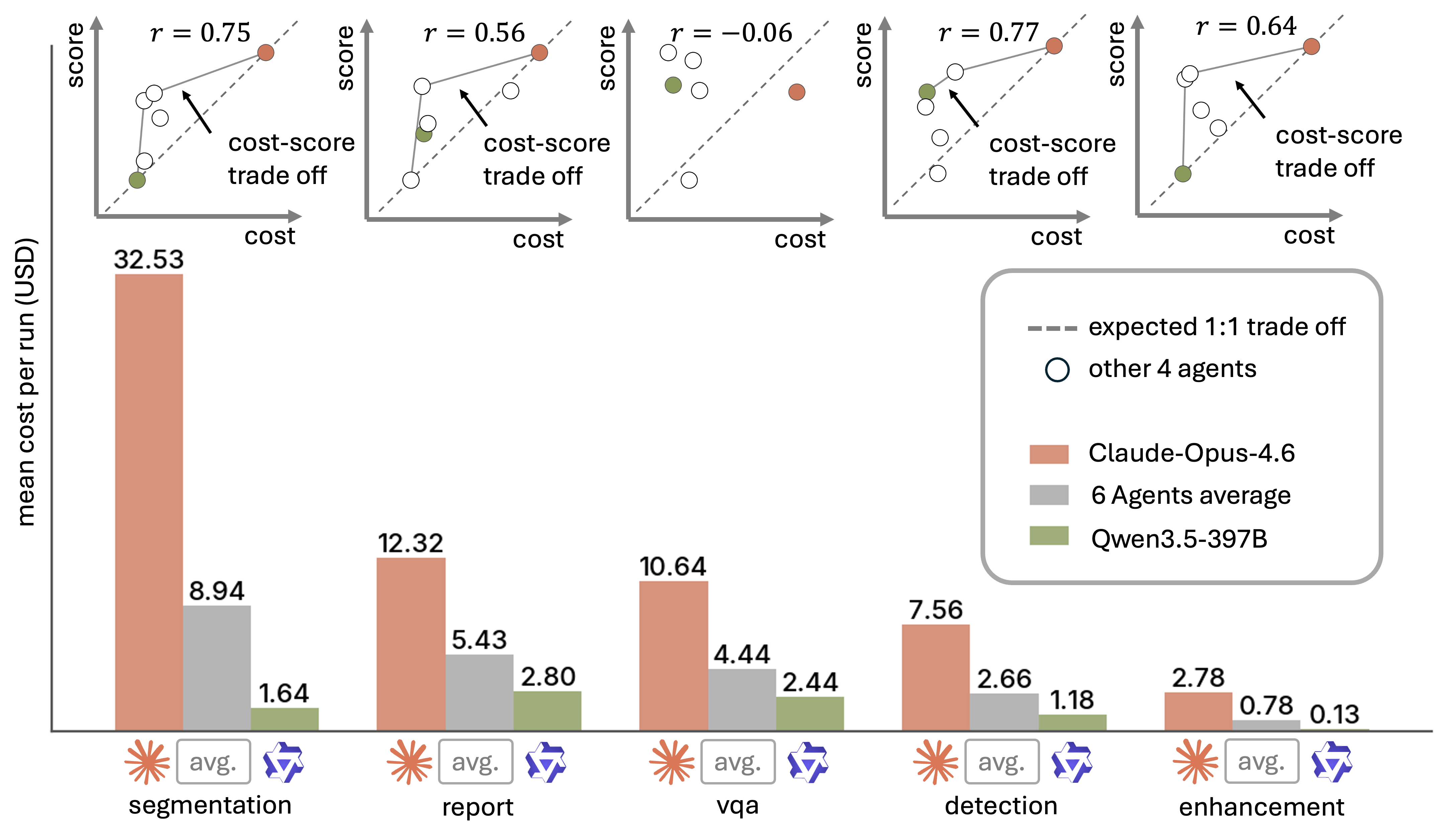
- Spending more isn’t a magic fix: Higher cost (more compute/tokens) doesn’t consistently mean better results. In some areas, spending helps; in others, it barely matters. Using compute wisely (especially for validation and fixing issues) matters more than just using more of it.
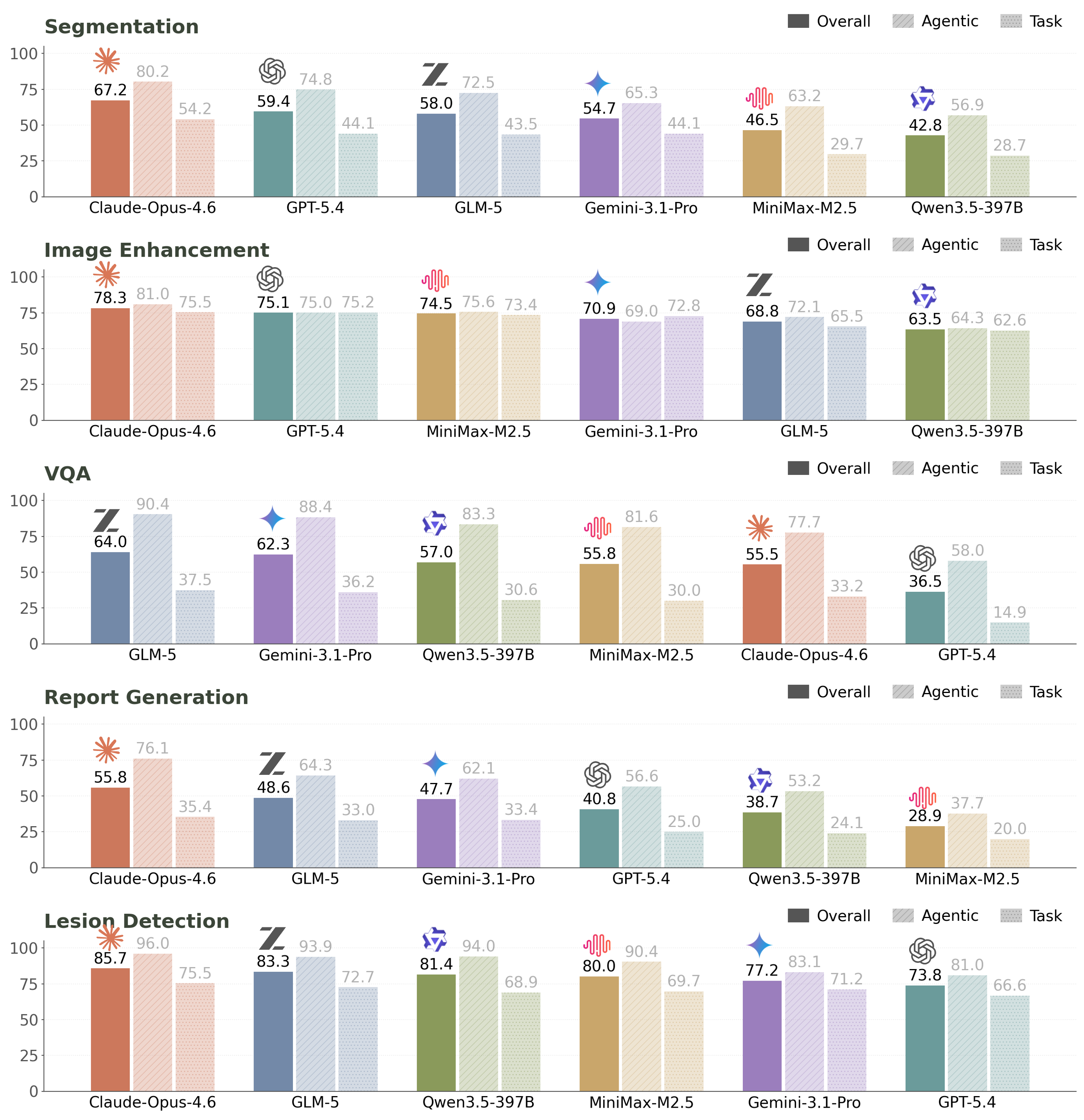
- Different tasks stress different skills: Detection tends to score higher for several agents (it’s a more contained output). VQA and report generation are tougher because they require stronger understanding and language generation. Segmentation of 3D medical images is heavy and complex, even for stronger agents.
5) Why does this matter?
AutoMedBench shows that if we want AI to be reliable “junior researchers” in medicine, they must do more than know facts. They need to:
- Build robust pipelines,
- Check their work with smart small tests,
- Catch and fix errors early,
- And package results correctly.
By grading both the process and the final result—and by tagging the types of errors—this benchmark helps researchers see exactly where agents fail and how to improve them. That could lead to safer, more trustworthy AI tools in medical research, and the same ideas could help build dependable AI agents in other fields that require careful step-by-step work.
Knowledge Gaps
Knowledge gaps, limitations, and open questions
Below is a single, concrete list of what the paper leaves missing, uncertain, or unexplored, framed to enable actionable follow-up studies:
- External validity to real agent systems: Only single base LLMs (no multi-agent controllers, planners, retrieval/routing frameworks, or domain toolchains) were evaluated; it remains unknown how full-stack agent systems with orchestration, retrieval, memory, and domain-specific tools would perform under the same tasks and workflow.
- Generality beyond six models: Results are based on six frontier base models; the benchmark’s sensitivity to different model sizes, families (e.g., medically-tuned LLMs), vision-language backbones, and open-weight checkpoints remains untested.
- LLM-judge reliability: S1–S3 stage scoring relies on an LLM judge; inter-judge reliability, calibration, bias, and robustness to “style over substance” are not reported, and no adjudication (e.g., multi-judge consensus, rubric perturbation tests) or sensitivity analysis is provided.
- Stage-weight sensitivity: The chosen Agentic stage weights (25/15/35/15/10) are heuristic; no ablation shows how rankings change under alternative weights or task-dependent weighting.
- Error-code assignment validity: Post-run error codes (E1–E5) are used diagnostically, but the assignment process, inter-rater agreement, automation vs. manual components, and error-detection precision/recall are not quantified.
- Causal attribution of failures: While Validate (S3) is the weakest stage, the benchmark does not disentangle root causes (e.g., inadequate test cases, absent sanity checks, metric misuse, poor visualization) or test which targeted interventions (checklists, executable tests, reference pipelines) improve S3.
- Tier design effects: Lite vs. Standard affects performance non-monotonically, but the paper does not analyze which specific scaffolding elements help or harm (e.g., dependency lists vs. method suggestions vs. step-by-step prompts), nor whether “scaffolding minimalism” outperforms heavier guidance.
- Cost and efficiency modeling: Cost analyses use an API price snapshot but do not standardize the compute accounting for self-hosted/open-weight models (GPU time, memory, energy), nor quantify cost variance from model updates, rate changes, or caching across replications.
- Temporal reproducibility: Hosted models can drift (weight updates, safety filters, rate limits); the benchmark does not report time-stamped model versions, judge versions, or re-run reproducibility (confidence intervals over time).
- Statistical uncertainty: Although multiple replications per cell are run, the paper does not report confidence intervals, variance decomposition (between-run vs. between-task), or statistical significance testing for leaderboard differences.
- Outcome validity beyond automatic metrics:
- Report generation is scored by n-gram overlap and RadGraph F1; the correlation with radiologist adjudication is unknown.
- Enhancement uses SSIM; diagnostic/clinical perceptual quality is unverified by experts.
- VQA uses accuracy; synonym handling, medical ontology grounding, and answer-set ambiguity are not addressed.
- No reader studies or expert audits are included.
- Clinical safety and harms: The benchmark does not evaluate whether agent outputs could induce clinically unsafe recommendations or misinterpretations; no safety auditing, harm taxonomies, or red-teaming results are provided.
- Data leakage risks via the open internet: Agents have network access; the paper does not demonstrate that tasks use splits whose references cannot be downloaded or inferred online (e.g., public leaderboards/ground truths), nor audit for leakage attempts.
- Real-world workflow coverage: Training/fine-tuning and adaptation are prohibited; the benchmark does not cover prevalent research steps such as domain adaptation, hyperparameter tuning, cross-validation, ablation studies, dataset curation/cleaning, bias audits, or uncertainty estimation.
- Missing task families and modalities: Important medical-AI workflows are absent (e.g., registration, classification/triage, radiotherapy planning/QA, longitudinal/time-series modeling, genomics, multi-omics, EHR+imaging fusion), limiting conclusions about “auto-research” breadth.
- Demographic fairness and subgroup robustness: No analysis is provided on performance across patient demographics, devices, institutions, or acquisition protocols; subgroup disparities and dataset shifts remain unmeasured.
- Environment robustness: Tasks run in curated containers; the benchmark does not test resilience to real-world environment variability (library version drift, CUDA/driver mismatches, missing codecs), nor the agent’s capacity for dependency conflict resolution.
- Security and adversarial robustness: The agent has code execution and network access, yet the benchmark does not test for prompt injection, data poisoning, malicious packages, or unsafe tool-use behaviors in the research pipeline.
- Provenance and reproducibility artifacts: S1 requires plan.md, but the benchmark does not require or score computational provenance (environment manifests, runtime seeds, deterministic pipelines), dataset cards, or experiment traceability.
- Submission and schema rigidity: S5 checks schema compliance but does not evaluate robustness to minor schema/spec changes, backward compatibility, or schema negotiation behaviors that are common in real evaluation servers.
- Turn-horizon and memory scaling: Average 33 turns are reported, but the benchmark does not explore how agent performance scales with longer horizons, larger projects (multi-experiment sequences), or persistent memory across runs.
- Interpretability and introspection: The paper identifies verification as a bottleneck but does not evaluate whether agent-accessible telemetry (e.g., uncertainty maps, saliency, unit tests) or interpretable failure reports improve S3 outcomes.
- Human-in-the-loop augmentation: No experiments assess partial human oversight (e.g., one-click approvals at S3 or S5), escalation policies, or optimal human-agent collaboration points to mitigate catastrophic failures.
- Cross-task generalization: It is unclear whether agents that devise a working pipeline for one task can reuse or adapt it efficiently to related tasks (transfer and reuse of code, configs, and validation checks are not measured).
- Leaderboard stability under task changes: The benchmark does not test sensitivity of rankings to alternative datasets, splits, or updated challenges within each track.
- Ethical/compliance dimensions: The study does not examine HIPAA/PHI handling in code, de-identification, licensing constraints of downloaded models, or compliance-aware tool use during network access.
- Multilinguality and global applicability: All briefs and tasks appear English-centric; the benchmark does not assess multilingual task briefs, non-English reports, or cross-lingual clinical contexts.
- Ground-truth provenance and uncertainty: The paper assumes fixed “private references” but does not discuss inter-rater variability in labels (e.g., segmentation masks), label noise, or evaluation under uncertain/ambiguous ground truth.
- Intervention studies: While common failure modes are identified (verification/submission), no controlled interventions (e.g., schema validators, auto-unit-tests, canonical pipelines, sandboxed checklists) are benchmarked to quantify achievable improvements.
- Time-cap sensitivity: Wall-time caps are fixed but not analyzed; it is unknown whether allowing more time (or adaptive time allocation across stages) would materially change stage-wise or overall outcomes.
- Fairness of overall aggregation: Overall equals 0.5×Agentic + 0.5×Task averaged across tracks; the impact of alternative aggregation schemes (e.g., outcome-only, track-weighted by case difficulty, safety-weighted) on rankings is not explored.
- Public release sustainability: With many upstream datasets and evolving models, the long-term maintainability of the harness, data access dependencies, and anti-leakage safeguards is not evaluated; no evergreen or rolling-benchmark protocol is specified.
- Cost–quality trade-off policies: While the paper notes weak cost–performance correlations, it does not propose or test budgeting policies (compute caps per stage, early-stopping rules, adaptive validation depth) that optimize return on spend.
- Baseline pipelines and oracles: There are no oracle baselines (e.g., human-coded reference pipelines per task, gold validation scripts) to quantify the performance gap between current agents and competent human researchers at each stage.
- Documentation and skill artifacts: Lite tier provides “skill files,” but the content quality, coverage, and ablations on their granularity are not analyzed; it remains unclear which skills most limit performance per track and how to teach them.
- Reuse of third-party code/models: Agents can download models, but the benchmark does not analyze licensing conflicts, model-card compliance, or the effect of pretraining provenance (medical vs. general) on performance and safety.
Practical Applications
Immediate Applications
Below are practical, deployable uses that directly leverage AutoMedBench’s workflow design (Plan–Setup–Validate–Inference–Submit), stage-level scoring, diagnostic error codes, isolation sandbox, and open-source harness.
- Bold procurement benchmarking for agentic AI in medical AI R&D
- Sectors: healthcare providers, imaging vendors, AI vendors, payers
- What: Run vendor models through the same five-stage benchmark to compare capability, reliability, and cost across segmentation, enhancement, VQA, reporting, and detection.
- Tools/products/workflows: Benchmark-as-an-internal service; scorecards combining Agentic, Task, and cost metrics; procurement RFP templates referencing S1–S5 gates.
- Assumptions/dependencies: Access to benchmark data (including any credentialed datasets), GPU capacity, adherence to inference-only policy, and acceptance of LLM-judge rubrics for S1–S3.
- Bold CI/CD gates for agentic pipelines
- Sectors: software/MLOps, healthcare AI labs, imaging software vendors
- What: Integrate S1–S5 checks into CI to block merges when validation or submission gates fail; detect “silent” regressions that final metrics miss.
- Tools/products/workflows: Git hooks, pre-merge “Validate” pilots on a small case set, schema verifiers for S5, automated stage reports in PRs.
- Assumptions/dependencies: Containerized execution, reproducible environments, stable pilot datasets, and time caps to keep CI fast.
- Bold Validation-first toolkits and checklists
- Sectors: healthcare, software
- What: Package reusable “Validate” components (pilot case runners, output sanity checks, failure heuristics) since Validate is the weakest stage in the findings.
- Tools/products/workflows: Auto-sanity check library (e.g., empty/NaN masks, out-of-range intensities, shape mismatches), visual diffs, alerting.
- Assumptions/dependencies: Domain-appropriate checks per modality, consistent file schemas.
- Bold Submission schema verifiers and artifact linters
- Sectors: healthcare, challenge organizers, model hubs
- What: Prevent malformed submissions (a top error class) via pre-submit validators and fix-it suggestions.
- Tools/products/workflows: CLI/SDK that validates filenames, JSON schemas, image/mask dimensions; preflight “dry run” evaluator.
- Assumptions/dependencies: Up-to-date schemas; tight coupling to evaluator’s parsing rules.
- Bold Cost-performance planning and model selection
- Sectors: healthcare, finance/ops for R&D, cloud providers
- What: Use benchmark logs to choose the most cost-effective agent for a given track; plan budgets recognizing weak cost–performance correlation.
- Tools/products/workflows: Dashboards plotting score vs. spend per track; budget-aware orchestration (e.g., choose lower-cost agent for detection).
- Assumptions/dependencies: Stable API pricing, consistent decoding settings, representative workloads.
- Bold Diagnostic training data for agent improvement
- Sectors: academia, AI vendors
- What: Use traces and error-code labels (E1–E5) to supervise finetuning, RLAIF/RLHF, or tool-use policies targeting verification and submission failures.
- Tools/products/workflows: Process-level reward models; curriculum that emphasizes S3 (Validate) and S5 (Submit).
- Assumptions/dependencies: Rights to use traces for training; careful judge consistency for S1–S3 labels.
- Bold Reproducible challenge hosting with process scoring
- Sectors: academic challenge organizers, societies, conferences
- What: Host tasks with isolation, hidden references, and S1–S5 rubrics to emphasize engineering reliability, not just final accuracy.
- Tools/products/workflows: Container templates, offline evaluators, tiered briefs (Lite/Standard), public leaderboards with stage breakdowns.
- Assumptions/dependencies: Compliance with dataset licenses, secure infrastructure for private references.
- Bold Laboratory audit trails for research QA
- Sectors: academia, industry labs, publishers
- What: Archive conversation traces, stage artifacts, and fired error codes to support internal QA and external reproducibility checks.
- Tools/products/workflows: “Experiment dossier” including plan.md, dependency manifests, pilot outputs, submission snapshots.
- Assumptions/dependencies: Data governance aligned with IRB/ETHICS; storage policies for logs.
- Bold Curriculum modules for end-to-end medical-AI workflows
- Sectors: education (biomedical engineering, CS, data science), continuing medical education
- What: Teach students to plan, set up, validate, infer, and submit under controlled tiers; grade both process and outcome.
- Tools/products/workflows: Course assignments mapped to S1–S5; rubrics mirroring the benchmark’s.
- Assumptions/dependencies: Institutional access to public datasets; limited compute for class scale.
- Bold Secure agent sandbox patterns for hospitals
- Sectors: healthcare IT, security
- What: Adopt the two-container isolation design (agent vs. offline evaluator) to safely run code-executing agents on on-prem data.
- Tools/products/workflows: Strict read/write mounts, network policy, policy-based termination on sandbox violations.
- Assumptions/dependencies: On-prem GPU servers, container orchestration (Kubernetes), security review.
- Bold Scaffold sensitivity testing
- Sectors: AI vendors, research labs
- What: Use Lite vs. Standard briefs to assess whether added instructions help or hinder an agent’s reliability and efficiency.
- Tools/products/workflows: A/B testing of prompts; remove brittle steps; tune scaffolds to boost validation.
- Assumptions/dependencies: Comparable time caps and data across tiers; method-agnostic prompts.
- Bold Journal and grant review checklists
- Sectors: publishing, funding agencies, policy
- What: Encourage submissions to include stage evidence (plans, validation artifacts, schema checks), not only final metrics.
- Tools/products/workflows: Reviewer forms aligned to S1–S5; attach stage-level logs in supplementary materials.
- Assumptions/dependencies: Willingness of venues to adopt process-aware standards; author compliance.
Long-Term Applications
These opportunities build on the paper’s methodology and findings but require further research, scaling, or ecosystem development.
- Bold Autonomous medical-AI research assistants
- Sectors: healthcare R&D, imaging vendors
- What: Agents that reliably plan, assemble, validate, and submit pipelines across modalities, with robust error recovery.
- Tools/products/workflows: Self-correcting Validate loops; multi-case pilot sampling; automatic fix proposal and re-run.
- Assumptions/dependencies: Significant advances in verification, tool-use reliability, and long-horizon memory; broader evaluation beyond benchmark tasks.
- Bold Regulatory sandboxes and pre-market evaluation protocols
- Sectors: policy/regulation (e.g., FDA, MHRA), standards bodies
- What: Stage-aware acceptance tests for agentic systems; require evidence of validation and submission correctness for approval in research settings.
- Tools/products/workflows: Standardized S1–S5 audit packages, process KPIs (recovery rates, error mixes), locked-down evaluators.
- Assumptions/dependencies: Consensus on process metrics; expansion to clinical safety criteria; secure infrastructure for protected data.
- Bold On-prem AutoResearch platforms integrated with hospital systems
- Sectors: healthcare IT, PACS/VNA vendors
- What: Private AutoMedBench-like platforms that connect to data lakes and run agentic studies safely on local images.
- Tools/products/workflows: DICOM/PACS connectors; policy-compliant access controls; automatic de-identification and logging.
- Assumptions/dependencies: Strong governance, HITRUST/ISO alignment, data-use agreements, and reliable container isolation.
- Bold Process-level training paradigms (rewarding S1–S5 behavior)
- Sectors: academia, AI vendors
- What: Train agents with process rewards (planning quality, validation rigor, submission correctness) in addition to outcome metrics.
- Tools/products/workflows: Multi-objective RL using stage scores and deterministic task outcomes; curriculum prioritizing verification.
- Assumptions/dependencies: Stable and unbiased LLM judging; scalable, cost-efficient feedback pipelines.
- Bold Cost-aware orchestration and scheduling
- Sectors: cloud platforms, MLOps, finance/ops
- What: Dynamically route tasks to cost-efficient agents by track, auto-scale pilots, and cap spend while keeping quality targets.
- Tools/products/workflows: Budget-aware controllers, early-stop heuristics, tier-switching (Lite↔Standard) based on progress signals.
- Assumptions/dependencies: Accurate cost telemetry; predictable performance under variable prompts and tool stacks.
- Bold Cross-domain extensions of the S1–S5 protocol
- Sectors: software engineering, robotics, energy, finance
- What: Adapt the workflow and error taxonomy to other long-horizon, code-executing agent tasks (e.g., robotics experiments, energy forecasts).
- Tools/products/workflows: Domain-specific Validate checks and schemas; new evaluators with private references.
- Assumptions/dependencies: Availability of deterministic, ground-truthable outcomes; safe execution sandboxes.
- Bold Marketplace/clearinghouse for agent reliability
- Sectors: platforms, model hubs, challenge organizers
- What: Public leaderboards augmented with process metrics, recovery rates, and error-code profiles to certify agent readiness.
- Tools/products/workflows: “Reliability badges,” sector-specific acceptance criteria, continuous evaluation feeds.
- Assumptions/dependencies: Community buy-in; standardized reporting; anti-gaming safeguards.
- Bold Automated remediation bots for failed submissions
- Sectors: healthcare R&D, challenge hosts
- What: Bots that detect failure patterns (E3/E5) and propose targeted fixes (rename files, patch shapes, re-run pilots).
- Tools/products/workflows: Playbooks keyed to error codes; safe “fix-and-try-again” loops.
- Assumptions/dependencies: Accurate failure classification; safe code patching; bounded risk of cascading errors.
- Bold Educational simulators for collaborative human–agent research
- Sectors: education, workforce training
- What: Simulated labs where students guide agents through S1–S5, learning best practices for verification and submission discipline.
- Tools/products/workflows: Interactive sandboxes, rubric-based grading, reflection prompts after validation failures.
- Assumptions/dependencies: Scalable compute, instructor adoption, curricular alignment.
- Bold Low-risk clinical workflow automation (pre-processing and reporting scaffolds)
- Sectors: healthcare delivery
- What: Use agents to automate non-diagnostic steps (e.g., DICOM curation, image pre-processing, report template population) with strong validation and submission checks.
- Tools/products/workflows: Guardrailed pipelines with schema contracts and human-in-the-loop acceptance.
- Assumptions/dependencies: Clear risk categorization; human oversight; compliance with data privacy and safety regulations.
- Bold Meta-benchmark generation and continual evaluation
- Sectors: research platforms
- What: Automatically generate new tasks and variants with hidden references to prevent overfitting and to stress specific failure modes (e.g., validation neglect).
- Tools/products/workflows: Task templating, synthetic-but-checkable cases, rotating evaluation seeds.
- Assumptions/dependencies: Reliable synthetic data fidelity; governance against leakage.
- Bold Provenance-centric compliance automation
- Sectors: policy/compliance, healthcare IT
- What: Leverage rich traces to automate provenance reports, risk scores, and compliance attestations for agent-driven research.
- Tools/products/workflows: Trace-to-report compilers; conformance checks tied to S1–S5 evidence.
- Assumptions/dependencies: Standardized provenance schemas; acceptance by auditors/regulators.
Notes on feasibility and dependencies common across applications:
- The benchmark enforces inference-only runs; applications requiring training will need extensions.
- Stage scores S1–S3 rely on LLM-judge assessments; long-term robustness requires judge calibration and guardrails.
- Access to credentialed medical datasets and secure, containerized compute is often necessary.
- Results show validation and submission are dominant failure modes; prioritizing these stages yields the highest practical payoff.
- Cost does not reliably predict performance; operational tooling should emphasize efficient validation and recovery, not just budget increases.
Glossary
- Agentic score: A process-oriented measure of how well an agent completes the benchmark’s five workflow stages. "Each run receives an Agentic score based on S1--S5 workflow completion"
- AutoResearch: An emerging direction where AI agents autonomously conduct research workflows end to end. "This emerging direction, often referred to as AutoResearch, raises a fundamental question:"
- BLEU: A machine translation-style n-gram overlap metric used to evaluate generated text such as reports. "For report generation, we use the unweighted mean of BLEU, METEOR, ROUGE-L, F1RadGraph, and micro precision, recall, and F1."
- Deterministic held-out evaluation: An assessment method where performance is computed reproducibly against hidden references not visible to the agent. "deterministic held-out evaluation using private references."
- EHR: Electronic Health Records; structured clinical data systems used in healthcare. "EHR/FHIR interaction"
- F1RadGraph: A radiology-specific information extraction metric measuring graph-based clinical correctness. "For report generation, we use the unweighted mean of BLEU, METEOR, ROUGE-L, F1RadGraph, and micro precision, recall, and F1."
- FHIR: Fast Healthcare Interoperability Resources; a standard for exchanging healthcare information electronically. "EHR/FHIR interaction"
- Held-out references: Ground-truth data used for evaluation that remains hidden from the agent during execution. "Held-out references are never visible to the agent and are mounted only inside the offline evaluator after the run terminates."
- Inference-only protocol: A restriction that allows agents to run pre-trained models but forbids training or fine-tuning during a benchmark run. "To ensure fair and reproducible evaluation under this isolation design, AutoMedBench enforces an inference-only protocol."
- IoU: Intersection over Union; an overlap metric used in detection/segmentation to compare predicted and true regions. "mAP at IoU $0.5$"
- Isolation policy: Rules that enforce strict separation between the agent’s environment and private evaluation resources. "bypass the sandbox, or otherwise violate the isolation policy, the benchmark harness flags the run"
- LLM judge: An evaluation method where a LLM scores qualitative aspects of an agent’s planning, setup, or validation. "S1--S3 are evaluated as LLM judge scores from saved artifacts and execution traces"
- Macro Dice: The class-averaged Dice coefficient used to evaluate segmentation performance across categories. "We use macro Dice for segmentation"
- [email protected]: Mean Average Precision computed at an IoU threshold of 0.5, commonly used for object detection. "Detection~([email protected])"
- METEOR: A text generation metric that considers synonyms and stemming to better capture semantic similarity. "For report generation, we use the unweighted mean of BLEU, METEOR, ROUGE-L, F1RadGraph, and micro precision, recall, and F1."
- MR-Linac: A medical imaging and radiotherapy system combining MRI with a linear accelerator. "T1-w MR-Linac"
- Offline evaluator: A separate, isolated component that has access to hidden references and computes final scores after the agent’s run ends. "mounted only inside the offline evaluator after the run terminates."
- Public-input/private-reference split: A protocol where agents can read only public inputs while hidden references are reserved for evaluation. "All tasks follow the public-input/private-reference split described in Section~\ref{sec:method}."
- ROUGE-L: A sequence overlap metric focusing on the longest common subsequence between generated and reference texts. "For report generation, we use the unweighted mean of BLEU, METEOR, ROUGE-L, F1RadGraph, and micro precision, recall, and F1."
- Sandbox: A controlled execution environment that restricts file system and network access to enforce benchmark rules. "bypass the sandbox"
- Segmentation mask: A pixel-wise or voxel-wise labeled output delineating structures in medical images. "segmentation masks"
- Submission schema: The required file format and structure for submitted artifacts to be scored. "Verify the submission schema and submit the final artifacts."
- SSIM: Structural Similarity Index Measure; a perceptual metric for comparing image quality. "We use macro Dice for segmentation, mean SSIM for image enhancement"
- Two-container isolation: A security design that separates the agent’s runtime from the evaluator to prevent leakage of private references. "Each task is executed under two-container isolation."
- VQA: Visual Question Answering; tasks where models answer questions about images, here in medical contexts. "visual question answering (VQA)"
- Wall-time cap: A fixed maximum run time after which the agent is stopped and partial outputs are evaluated. "Each task has a fixed wall-time cap that is held constant across agents and difficulty tiers."
Collections
Sign up for free to add this paper to one or more collections.