- The paper demonstrates that diffusion models can match or exceed autoregressive models in medical VQA performance, with metrics like 0.863 vs. 0.817 on SLAKE.
- The paper shows that diffusion inference reduces latency by 3.5–4.4× and increases throughput by 5.7–7.1×, enabling near real-time report drafting.
- The paper reveals that bidirectional any-order infill leads to significant gains in token-F1 and LLM-judge accuracy, supporting flexible, interactive editing workflows.
Discrete Diffusion LLMs for Interactive Radiology Report Drafting
Introduction and Problem Statement
This paper systematically evaluates discrete diffusion LLMs (DLMs) as applied to the task of interactive radiology report drafting, contrasting them against autoregressive (AR) counterparts—a dominant paradigm in both general LLMs and medical foundation models. Diffusion models, which generate text by iteratively denoising a bidirectional token canvas, have recently emerged as a scalable and competitive alternative to AR generation. Despite their advances in general and multimodal domains, their efficacy, efficiency, and applicability as medical foundation models, and, critically, their ability to support bidirectional and fragment-based conditioning in clinical workflows, remain unexplored at scale.
Model Design and Experimental Protocol
The primary experimental contrast involves DiffusionGemma-26B—a mixture-of-experts, block diffusion LLM with a SigLIP-lineage vision encoder—against its AR sibling, Gemma-4-26B. The adaptation protocol uses a tightly matched LoRA setup: only the generative paradigm is varied, with all other architectural and data factors held constant, ensuring fidelity of comparison. LoRA rank, layer targets, frozen parameters, and image encoders are identical. Optimization hyperparameters follow standard practice for each paradigm.
Fine-tuning occurs on paired image-text datasets, with the image always fixed and the language target being either a full radiology report (for drafting/infill) or a short-form medical VQA answer. The evaluation is threefold:
- Open-ended medical VQA, scored via a verbosity-robust LLM judge to account for semantic equivalence, not string-matching.
- Inference speed, benchmarked for latency and throughput.
- Any-order infill: the capability to fill gaps from arbitrary, fixed fragments, corresponding to radiologist-driven interactive drafting.
The LLM-judge evaluation on VQA-RAD, SLAKE, and VQA-Med (2019) demonstrates robust performance of the diffusion paradigm:
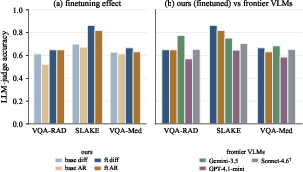
Figure 1: LLM-judge accuracy (Claude Sonnet 4.6). (a) Base vs. finetuned, for diffusion and AR. (b) The finetuned 26B model (3.8B active) against three frontier non-reasoning VLMs.
- Finetuned diffusion equals or exceeds AR on all datasets: e.g., $0.863$ vs. $0.817$ on SLAKE (diffusion vs. AR).
- Diffusion attains or exceeds base AR performance before finetuning: e.g., $0.700$ vs. $0.674$ on SLAKE.
- Performance is competitive with state-of-the-art VLMs (Gemini-3.5-Flash, GPT-4.1-mini, Claude Sonnet 4.6), with diffusion matched or outperforming all but Gemini-3.5-Flash in zero-shot evaluations.
- Statistical significance (McNemar, n=350) of the diffusion-AR gap is moderate and dataset dependent, being robust on closed-format (yes/no) questions.
These results directly challenge the entrenched assumption that next-token prediction is inherently advantageous in clinical VQA, especially for tasks that hinge on image-to-text grounding and semantic nuance.
Inference Speed and Computational Efficiency
Diffusion inference operates on a fixed $256$-token canvas, denoising all unfixed positions in parallel over a small number of steps, while AR decoding remains strictly sequential. The empirical results:
- Drafting speed for diffusion is $3.5$–4.4× lower in latency and $5.7$–7.1× higher in throughput for $0.817$0256 token outputs.
- Speed superiority holds even when AR is favored by shorter outputs, with matched hardware and precision (bf16, H100).
This computational advantage is intrinsic to bidirectional denoising and suggests diffusion LLMs can support iterative, near real-time drafting cycles in clinical user interfaces.
Any-Order Infill: Conditioning Capability and Clinical Alignment
A central contribution is the rigorous operationalization of any-order infill, leveraging diffusion's ability for conditional generation from arbitrary fixed contexts (“fragments”). Experimental design involves deterministic masking of a mid-report sentence (MIMIC-CXR, $0.817$1), followed by filling the gap under two conditions: left-only (strict AR context emulation) and bidirectional (both sides fixed).
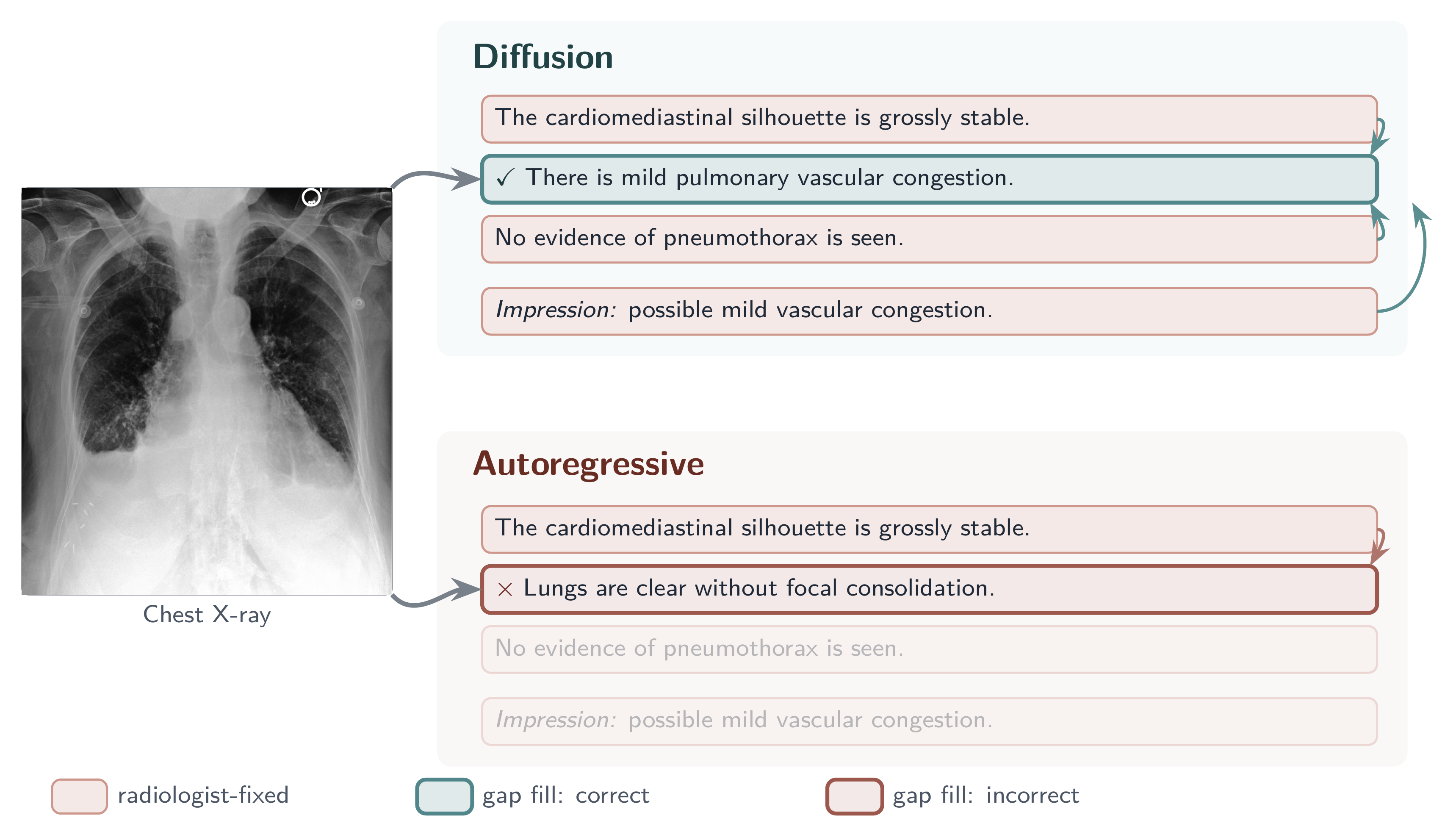
Figure 2: Completing a gap from both sides. One sentence of a chest X-ray report is masked (the gap) and filled from the surrounding fixed fragments. Top: the diffusion model draws on fragments on either side and recovers the sentence correctly. Bottom: the autoregressive sibling sees only the fragments before it, the rest greyed out, and reconstructs it incorrectly. Real MIMIC-CXR example.
- Diffusion models exhibit strong exploitation of right-side context: bidirectional infill yields $0.817$2 token-F1 and $0.817$3 LLM-judge accuracy gains ($0.817$4) over left-only.
- AR models, even when prompted with both sides, do not benefit: the right context is ignored, reflecting the structural left-to-right constraint.
- Significant model$0.817$5context interaction, with diffusion benefiting $0.817$6 more from bidirectional context than AR, demonstrating a unique inductive bias in DLMs for interactive clinical drafting.
This property is functionally important for real-world report editing, where clinicians frequently revise, append, or correct text at arbitrary positions, necessitating non-causal, fragment-respecting generation—a workflow that AR decoders cannot natively support.
Practical and Theoretical Implications
The results have immediate implications for the design of clinical AI interfaces:
- DLMs are viable “drop-in” replacements for AR models with respect to output quality, finetuning tractability, and vision-language grounding on medical questions.
- Bidirectional generative conditioning inherent to diffusion is pragmatically aligned with the way radiologists author, revise, and finalize reports, supporting genuine human-AI co-editing rather than just auto-drafting.
- Faster decoding supports integration into interactive applications, reducing friction in clinical environments with strict latency constraints.
At the modeling paradigm level, this study provides empirical evidence that supports a fundamental advantage for discrete diffusion in domains with fine-grained, user-driven draft manipulation, highlighting the limitations of the left-to-right factorization even when supplemented with tricks such as right-context grounding in prompts.
Future Directions
- Extension to full multimodal, longitudinal workflows (e.g., series-level radiology, multi-slice cross-report referencing).
- Exploration of larger context windows and memory-augmented denoising samplers.
- Generalization to other domains with document or code editing tasks, where any-order revision is integral.
Conclusion
This paper delivers a robust, controlled evaluation of diffusion-based LLMs for medical report drafting, demonstrating parity with state-of-the-art AR and VLM models on medical VQA, a marked advantage in any-order infill and interactive drafting, and strong computational efficiency. These findings establish a new paradigm for clinical LLM deployment, prioritizing flexibility, speed, and direct alignment with clinician workflows by leveraging the intrinsic strengths of diffusion decoders.