- The paper demonstrates the Manana framework using non-parametric prompt learning and multi-agent roles to adapt LLMs for local epilepsy care.
- It introduces Bayesian Prompt Averaging to aggregate confidence scores, achieving up to 97% EM@3 in monotherapy and robust deferral signals.
- The study shows that evidence-gated prompt updates preserve interpretability and optimize specialist time in low-resource clinical settings.
Teaching LLMs to Recommend and Defer in Underrepresented Epilepsy Care: An Expert Overview
Introduction and Motivation
The paper "Teaching LLMs to Recommend and Defer in Underrepresented Epilepsy Care" (2606.31036) addresses a major gap in AI-driven clinical decision support: the adaptation and deployment of LLM-based prescription systems in low-resource, underrepresented clinical settings, specifically Ugandan pediatric epilepsy care. Standard medical LLM benchmarks and medication recommendation systems predominantly rely on structured data or QA settings from high-resource environments, which misaligns with the practicalities of LMIC healthcare delivery, where prescribing is shaped by local medication availability, cost, and infrastructure limitations.
This work establishes that deploying LLM-based assistants in such settings requires two critical capabilities: (1) adaptation to local prescribing policies, and (2) clear, uncertainty-aware deferral logic to allocate scarce specialist attention efficiently. The research operationalizes these requirements in the context of longitudinal anti-seizure medication (ASM) regimen prediction, analyzing performance relative to real clinician practice directly from unstructured local clinical notes—a setting where distribution shift and calibration failures are unavoidable for off-the-shelf systems.
The Manana Framework: Architecture and Learning
To overcome the domain-miscalibration problem of LLMs pretrained and prompted on Western-centric data, the authors propose Manana, a non-parametric prompt-learning framework that adapts a frozen LLM to local prescribing practices using a small set of region-specific, longitudinal patient records.
The learning protocol involves a modular, multi-agent architecture—split into Predictor, Inspector, and Architect functions:
- Predictor: A frozen LLM generates three candidate regimens per visit, conditioned on the current "memory" state (structured prompt artifact).
- Inspector: An LLM compares predictions to the ground-truth regimen, producing structured error diagnosis and proposing case-level candidate "learnings" (natural language summaries of potentially transferable feedback).
- Architect: Aggregates proposed learnings via an append-only evidence buffer, consolidating only cross-patient recurring patterns into the memory. Two instantiations are studied:
- Manana-Single: The memory is a list of global natural-language correction rules.
- Manana-Multi: The memory is a population of specialist agents, each surfacing a discrete clinical signal (without prescribing), whose outputs are read by the Predictor.
Both variants avoid any LLM weight updates, permitting deployment with minimal data and computational infrastructure, while maintaining interpretability and clinicians' ability to audit the learned prompt memory.
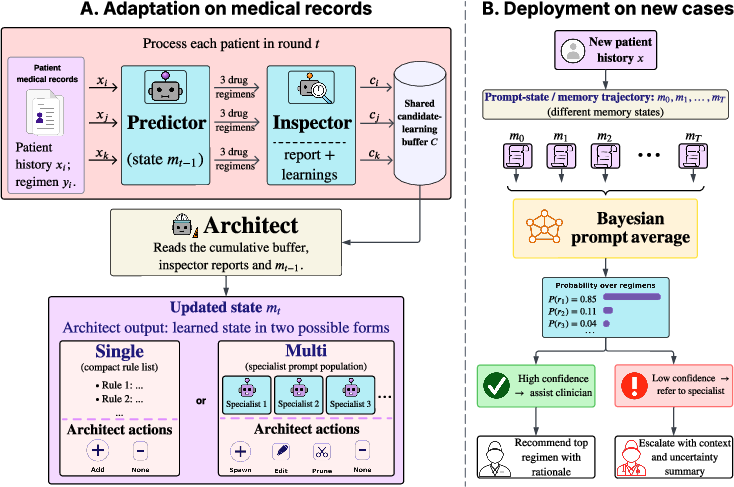
Figure 1: Manana workflow. The adaptation loop processes local cases in batches, accumulating learnings into an auditable memory; at inference, learned prompts are ensembled via Bayesian prompt averaging for probabilistic prescription and deferral signals.
Bayesian Prompt Averaging for Confidence and Deferral
A notable theoretical and practical contribution is the introduction of Bayesian Prompt Averaging (BPA). Manana's adaptation produces a trajectory of prompt memories, each representing an estimator of local prescribing policy. BPA aggregates the outputs of these learned memories using Bayesian model averaging, assigning weights according to marginal likelihood on validation data:
- For each memory, the number and position of times the physician's actual regimen appears in the top 3 predictions (with position priors empirically estimated) provide a marginal Beta-Binomial likelihood.
- Posterior weights are computed with temperature smoothing to prevent posterior collapse.
- At inference, the predicted regimens from all retained prompt states are merged, and their aggregated posterior probability mass forms a predictive distribution over regimens.
The BPA predictive confidence serves as the basis for selective prediction and deferral: cases above a user-defined confidence threshold can be auto-handled by the model, while uncertain cases are triaged to scarce human experts.
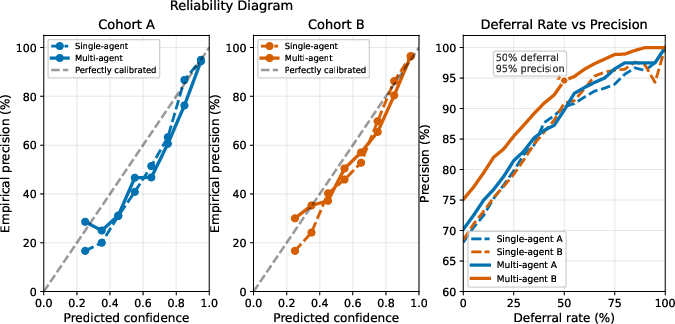
Figure 2: BPA confidence tracks empirical accuracy. The right panel shows that, by deferring the least confident 50% of cases, Manana-Multi reaches 95% agreement with expert prescriptions in the remainder.
Experimental Setting
Two pediatric epilepsy cohorts from Ugandan referral centers form the main evaluation, providing over 2,500 serial clinical visits across 699 patients, with notable regimen complexity and feature/medication-use distribution shifts (Figure 3). Each visit prediction uses only the clinical history notes up to that point. The evaluation metric is stringent: exact match within the top-3 (EM@3) of predicted active drug sets with physician prescription, stratified by mono/polytherapy.
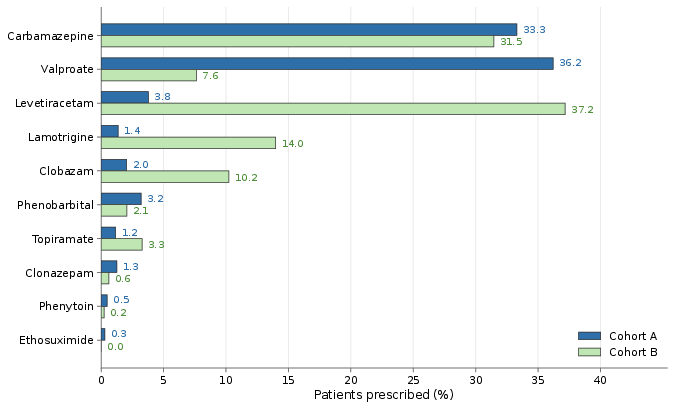
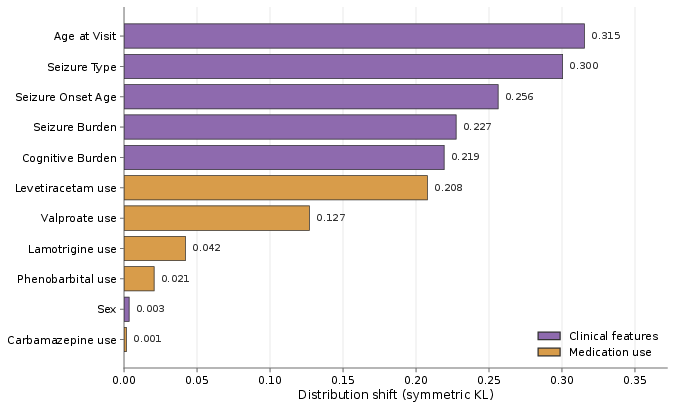
Figure 3: Medication-use profiles and KL-divergence between cohorts reveal substantial domain shift, further highlighting the necessity of localized adaptation.
Baselines include direct LLM prompting, expert-designed prompts, classical ML predictors on structured features, rule-based systems (e.g., EpiPick), and recent prompt-optimization approaches (e.g., TextGrad, ExpeL, DSPy).
Numerical Results
Across both in-domain and held-out cohorts:
- Manana-Multi achieves up to 97% EM@3 in monotherapy (V3, Cohort A) and outperforms all classical and neural baselines in most polytherapy and transfer settings, especially under distribution shift (Table 1).
- The Manana architecture's evidence-gated, consolidative memory update regularizes prompt learning, avoiding overfitting to noisy per-case signals—a key structural difference from prior textual-gradient and reflection-based prompt optimization.
BPA produces robust uncertainty estimates:
- BPA calibration is tight: BPA-assigned confidence tracks real accuracy across both cohorts.
- Selective deferral: On held-out (Cohort B), the system achieves 99% precision on the 25% most confident cases, and 95% when auto-handling half of all visits, optimizing the allocation of limited expert time.
Qualitative Expert Audit and Multi-Agent Reasoning
Neurologist audit (Figure 4) reveals that baseline LLMs make systematic errors when Western prescribing priors or specialist reasoning shortcuts fail under local constraints. Manana's memory-state artifacts are both interpretable and auditable by clinicians, and the multi-agent structure of Manana-Multi is found to correct for longitudinal drift, specialist nuance, and context-specific idiosyncrasies in drug choice.
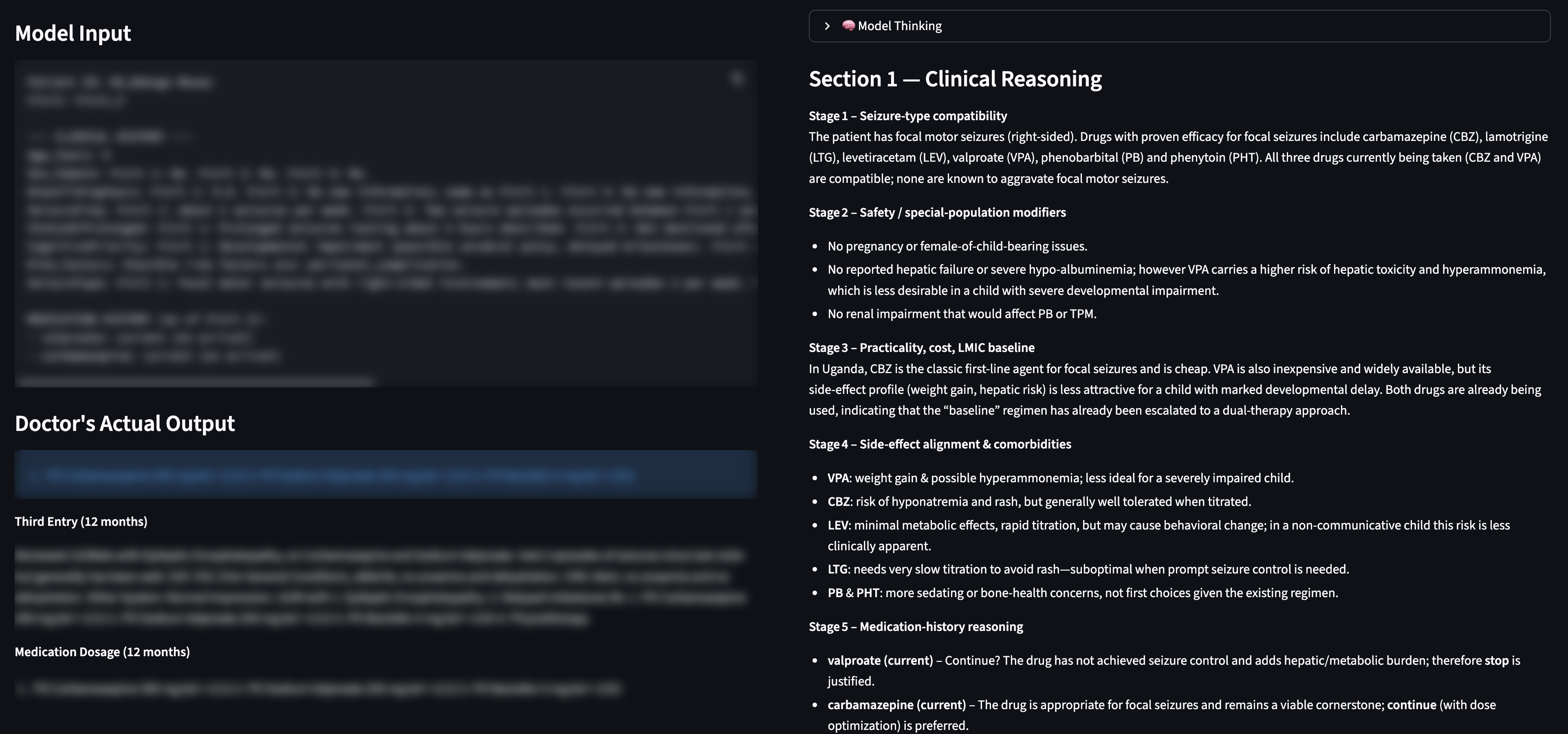
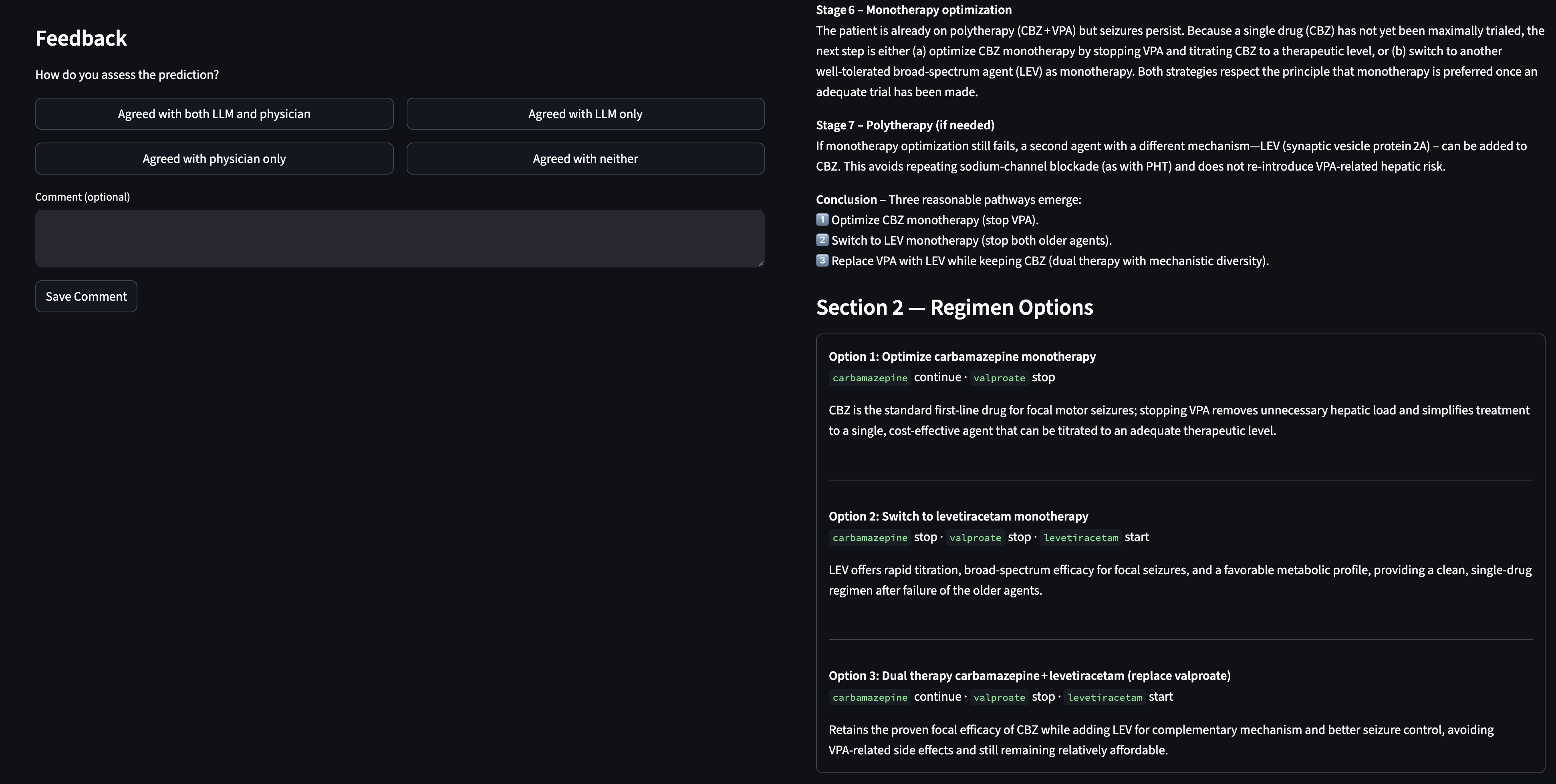
Figure 4: Custom neurologist audit interface for reviewing and adjudicating LLM-system recommendations and reasoning traces.
Further, the hand-designed Consilium multi-specialist system (Figure 5) validates, in expert-craft, the advantage of clinical lens decomposition; however, Manana surpasses it in learnability from local data and in its ability to produce actionable confidence for deferral.
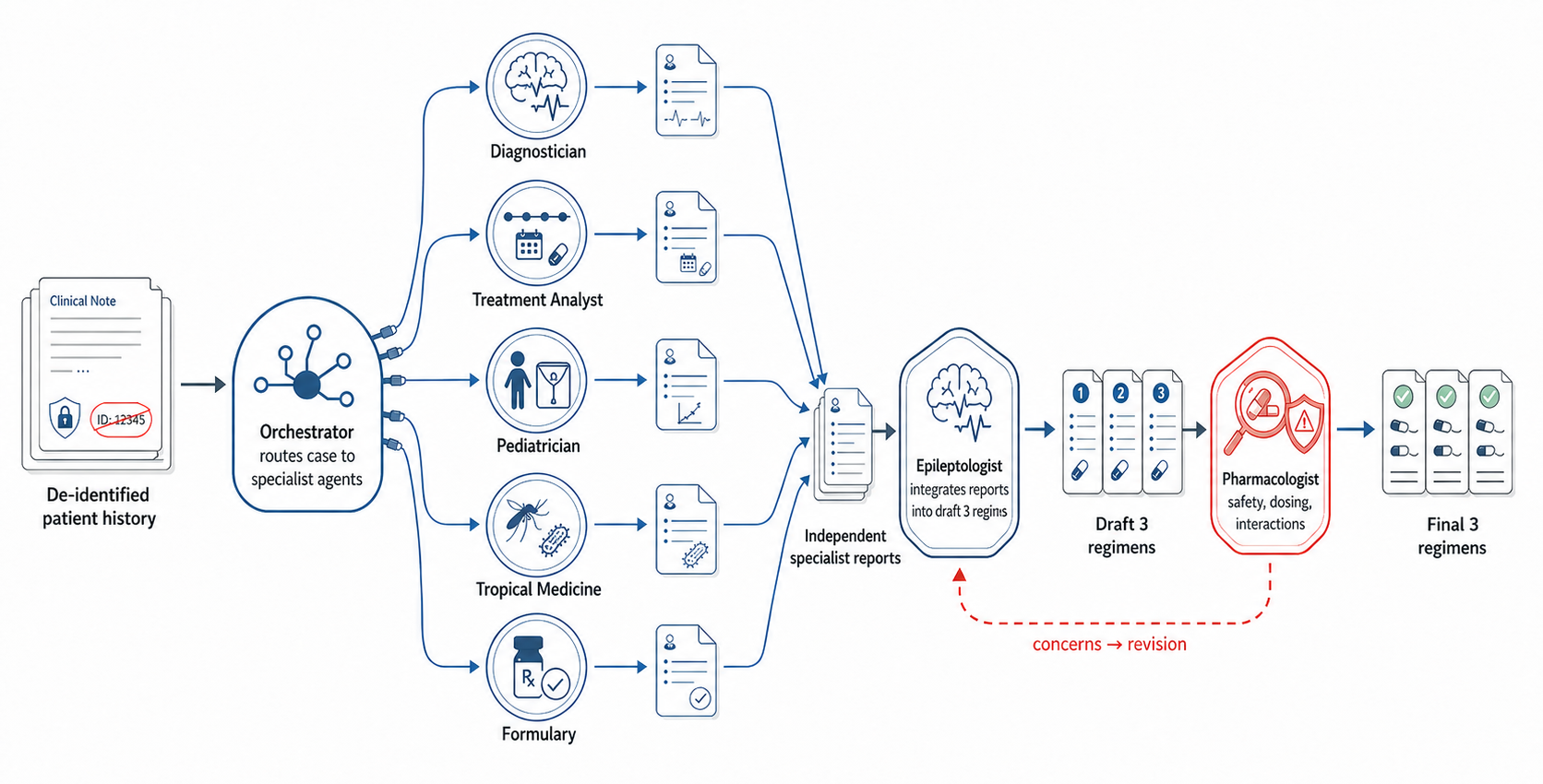
Figure 5: Consilium multi-agent workflow: explicit division of labor among clinical specialists with downstream aggregation and pharmacological safety check.
Implications and Limitations
Theoretical advances:
- This work rigorously demonstrates that non-parametric, evidence-gated prompt learning with multi-agent role decomposition confers substantial gains over textual feedback or monolithic prompting in high-shift, low-resource clinical settings.
- The BPA ensembling approach provides a formal mechanism for yielding calibrated prescription probabilities and practical, actionable uncertainty signals, addressing a major unmet need in safe clinical AI.
Practical consequences:
- LLMs can adapt to local, resource-constrained clinical workflows without retraining or infrastructure for continuous parameter updates.
- Systems are rendered interpretable and inspectable by design, critical for auditing and regulatory pathways in medical AI deployments.
- BPA-based deferral enables the deployment of LLM clinical aids that optimize for high-value use of limited specialist time—potentially generalizable to other decision support domains with similar constraints.
Limitations:
- The endpoint is agreement with physician prescription, not clinical outcome or therapeutic optimality—a critical direction for subsequent validation and audit.
- BPA provides a retrospective confidence score that should be prospectively calibrated in real-world deployment.
- Extensions to outcome-prediction and broader disorder types remain open problems.
Conclusion
This work advances the methodology for LLM-driven clinical decision support in underrepresented, resource-limited environments with high practical and scientific rigor. By integrating non-parametric prompt learning, modular error analysis, and Bayesian ensembling for uncertainty-aware deferral, the Manana framework achieves superior adaptation to local practice, robust performance under distribution shift, and actionable selective prediction properties, which are directly relevant for safe, equitable AI deployment in global healthcare. Future work will be required to tie system recommendations to clinical endpoints, operationalize deferral in live settings, and further generalize these mechanisms to other specialties and modalities.
References:
Full experimental and methodological details, including cohort statistics and prompt artifacts, are detailed in the paper appendices (2606.31036).