- The paper introduces ClaMPAPP, a hybrid LLM-ML system that uses LLMs for interface feature extraction and XGBoost for risk prediction, achieving high sensitivity in pediatric appendicitis diagnosis.
- The paper demonstrates that decoupling narrative processing from deterministic prediction enhances robustness against narrative perturbations and cohort variability.
- The paper shows that external calibration and validation across heterogeneous cohorts are crucial for ensuring reliable and auditable clinical decision support.
Hybrid Clinical Decision Support via LLM-ML Integration for Pediatric Appendicitis
Introduction
The paper "LLMs as Interfaces, Not Oracles: A Hybrid LLM-ML System for Pediatric Appendicitis" (2606.19183) presents ClaMPAPP, a hybrid clinical decision-support architecture that leverages LLMs for interface and feature extraction from clinical narratives while delegating risk prediction to a deterministic supervised ML model, specifically XGBoost. This paradigm addresses fundamental limitations of end-to-end LLMs in clinical decision-making, including susceptibility to hallucination, positional bias, and unstable sensitivity–specificity trade-offs, and mitigates the usability constraints of tabular ML systems in real-world workflows.
System Architecture
ClaMPAPP’s pipeline consists of four principal stages: ingestion of unstructured clinical notes; LLM-based schema-constrained feature extraction; deterministic safety validation of extracted features; and final risk prediction using an XGBoost classifier trained on validated clinical, laboratory, and sonographic data. The safety validator acts as a quality gate by enforcing physiological plausibility and type checks, mapping out-of-range or invalid features to NaN where necessary. The system is disease-agnostic and can, in principle, be applied to other modalities where structured prediction models are available.
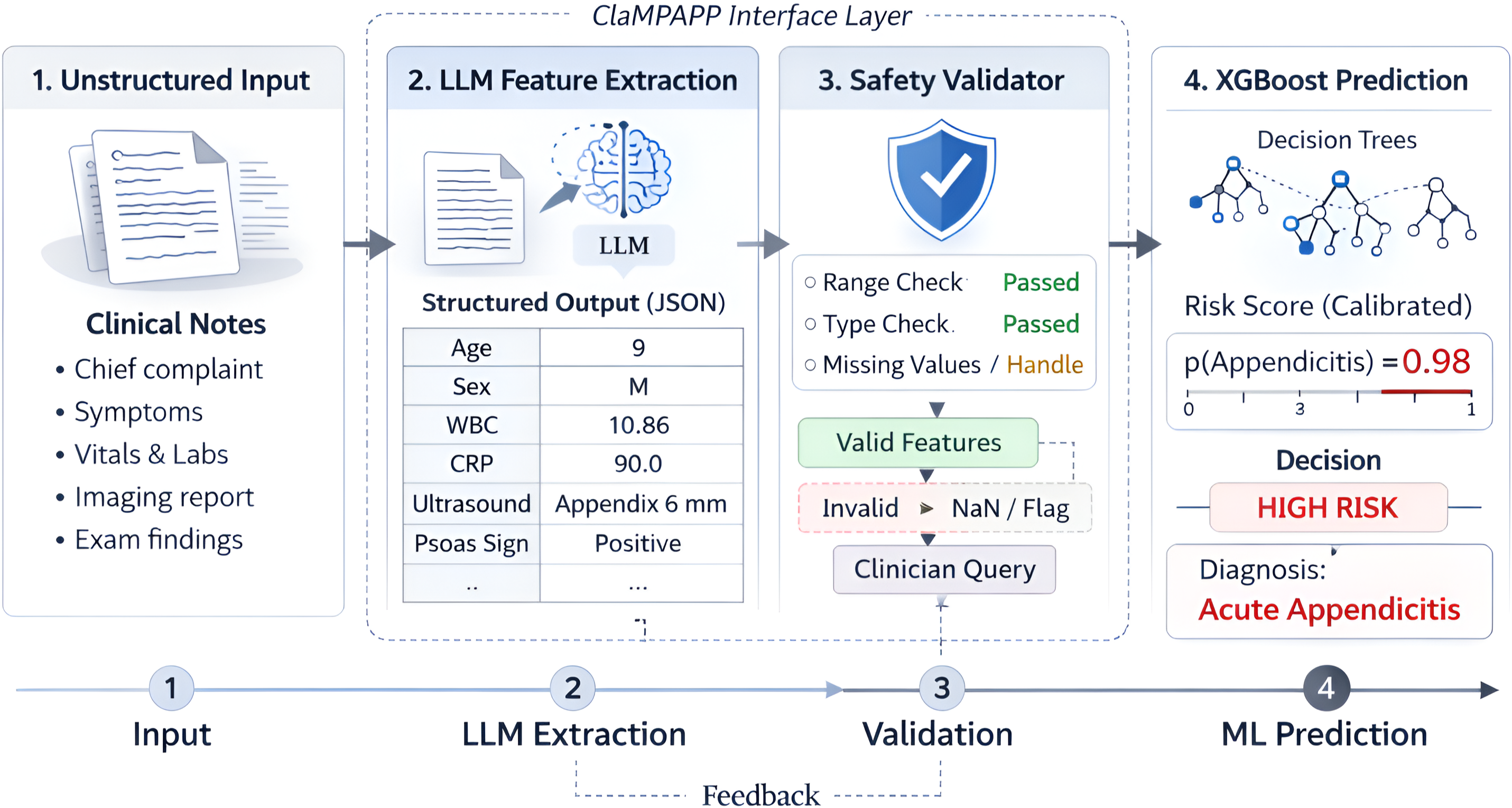
Figure 1: ClaMPAPP architecture showing LLM-based feature extraction, deterministic validation, and ML-based diagnosis.
The architecture robustly integrates narrative clinical documentation with structured ML-based prediction, advancing a more auditable and safety-aligned decision-support pipeline over unconstrained generative diagnosis.
Data Representation and Narrative Generation
A notable methodological element is the controlled synthesis of note-like clinical narratives from structured EHR variables. This is achieved in a four-stage pipeline: tabular EHR extraction, template rendering, constrained LLM rewriting (Llama-3.1-8B), and bipartite sentence-order permutation to probe robustness to permutation effects. Strict constraints were applied during rewriting to maintain ground truth fidelity, with manual audits confirming >96% preservation of clinical features across samples.
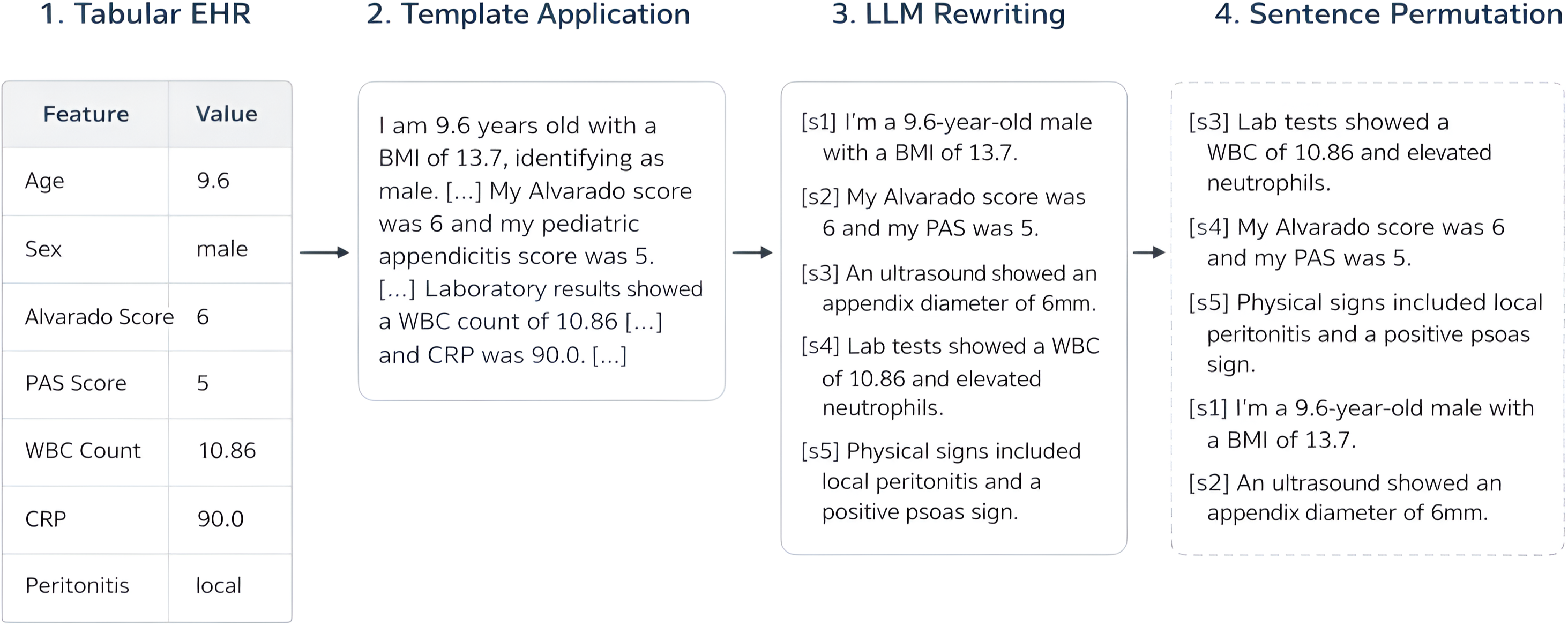
Figure 2: Data pipeline converting structured EHR to synthetic clinical narratives for downstream evaluation.
This setup enables rigorous assessment of extraction, decision-making, and robustness under realistic narrative perturbation while preserving true clinical content.
Cohort Design and Experimental Setting
The paper utilizes two independent pediatric cohorts from German hospitals: Regensburg (internal) and Düsseldorf (external). The Regensburg cohort is split for XGBoost training and internal validation, whereas Düsseldorf serves solely for external validation. This design facilitates analysis of both internal performance and out-of-site generalization and robustness.
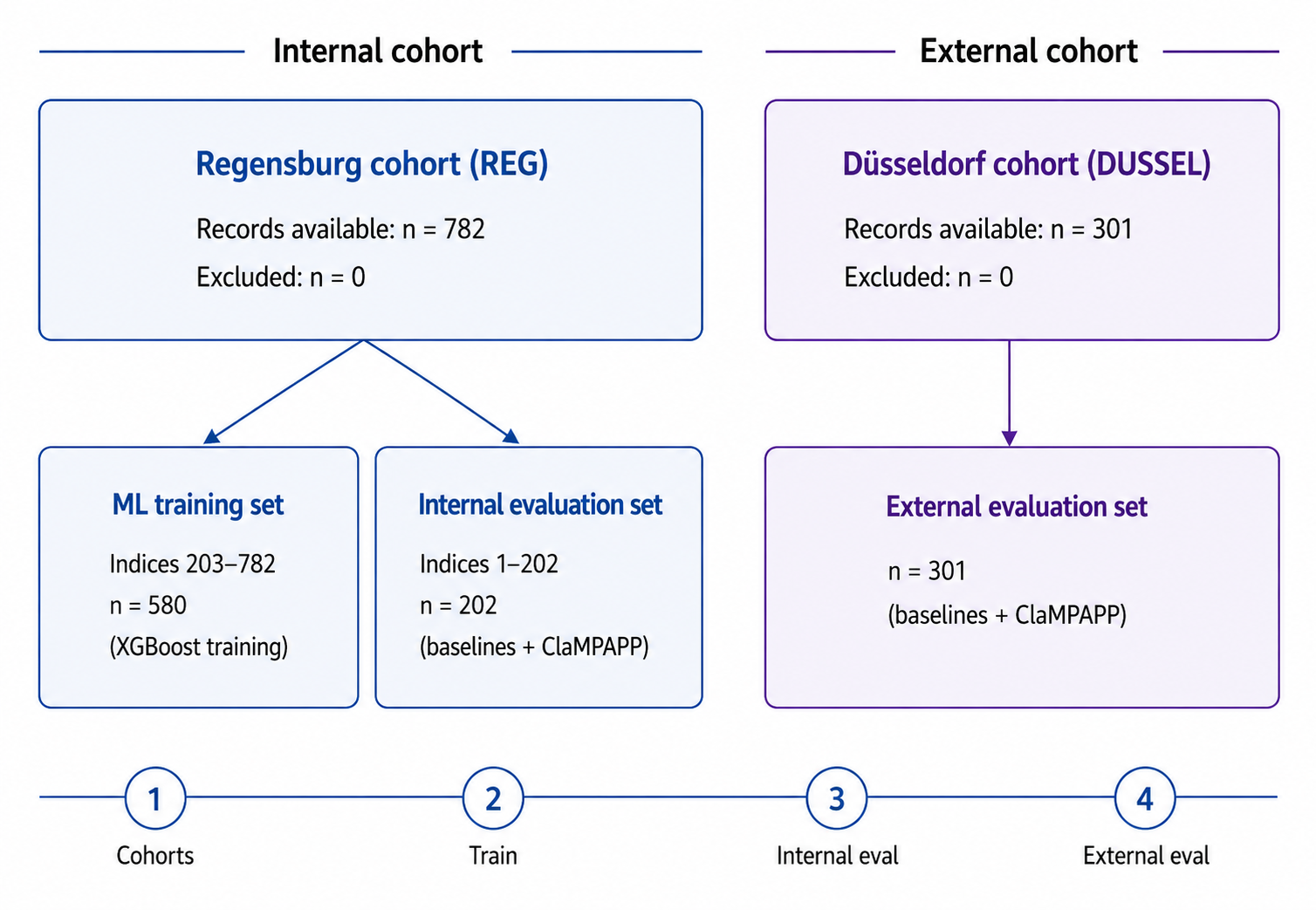
Figure 3: Patient cohort flow, showing splitting of Regensburg and external validation on Düsseldorf.
ClaMPAPP is benchmarked against a spectrum of LLM baselines—open-source and proprietary—with discrete binary predictions for appendicitis diagnosis. The XGBoost backbone is selected via performance comparison with alternative classifiers (LightGBM, Random Forest, Decision Tree, Logistic Regression) for optimal discrimination and robustness under cohort shift. On internal validation, ClaMPAPP achieves accuracy of 85.1% and sensitivity of 97.7%, missing only 2 confirmed appendicitis cases, an outstanding safety profile for triage.
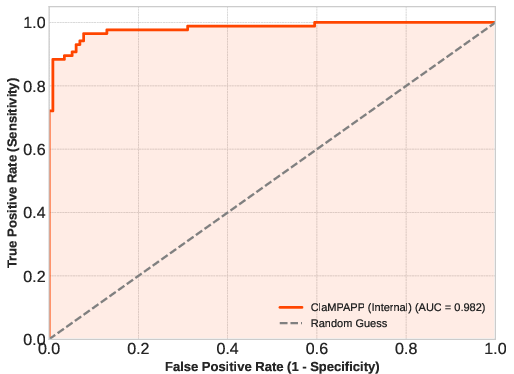
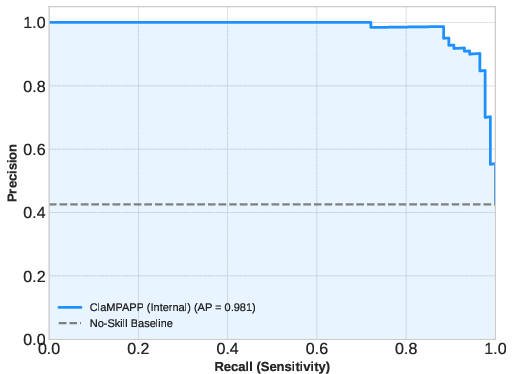
Figure 4: ROC curve for ClaMPAPP in internal cohort (AUC=0.982).
Externally, ClaMPAPP achieves accuracy 80.7% and sensitivity 93.5%, consistently outperforming LLM baselines, which either exhibit high specificity but low sensitivity (leading to unacceptable missed cases for triage) or collapse under prompt perturbation.
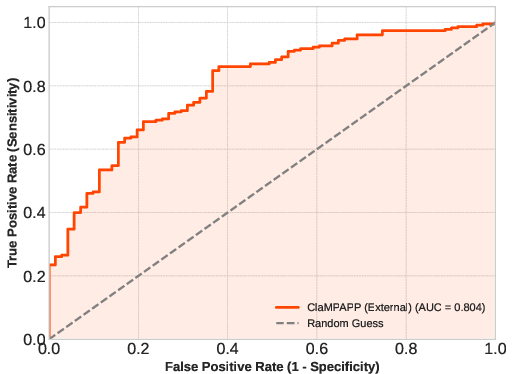
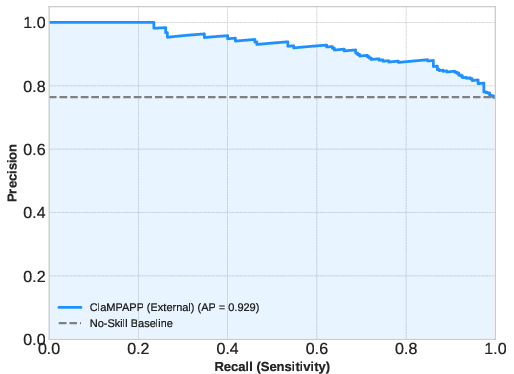
Figure 5: ROC curve for external validation (AUC=0.804).
Probability Calibration
Raw predicted probabilities from ClaMPAPP are well-discriminated but imperfectly calibrated, especially regarding the probability scale. Exploratory logistic recalibration improves calibration metrics on both cohorts, indicating that predictive ranking is robust but direct probability interpretation requires post hoc adjustment.
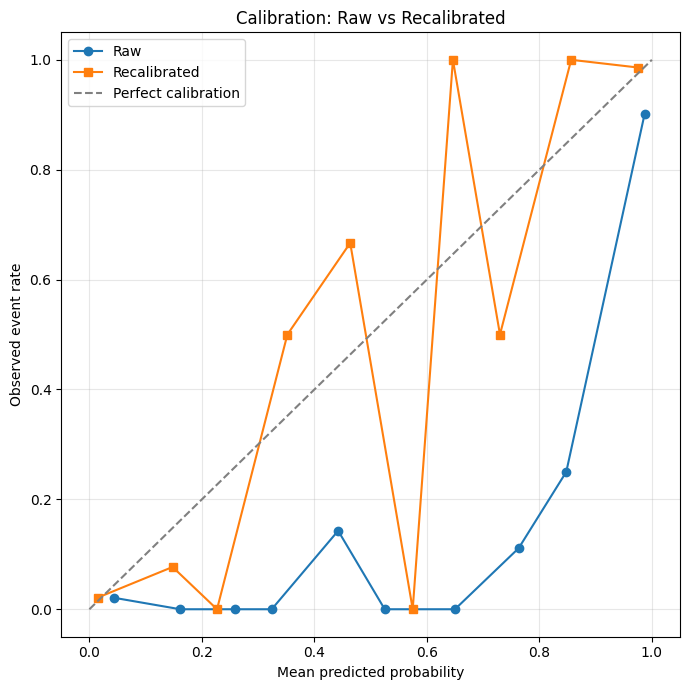
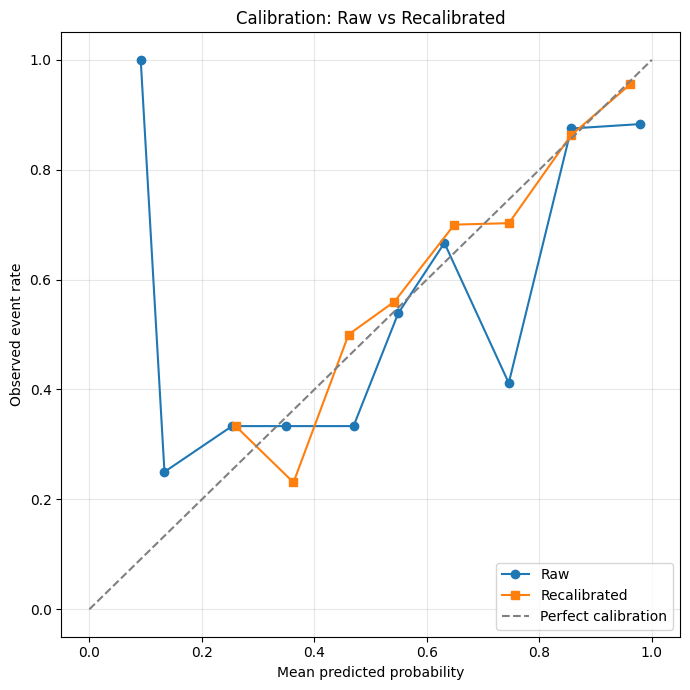
Figure 6: Reliability diagram for Regensburg cohort; recalibration improves correspondence between predicted risk and observed incidence.
Robustness to Narrative Perturbation
Sentence-order permutation—bipartite structural inversion—exposes significant positional vulnerability in pure LLM baselines, with accuracy drops of up to 30%. ClaMPAPP, by separating extraction from deterministic prediction, maintains high architectural robustness, showing only a 5.2% decrease in accuracy internally and strong safety profile externally (FN=17). Feature validation and structured downstream ML dramatically reduce the impact of positional and prompt biases, critical for real-world deployment.
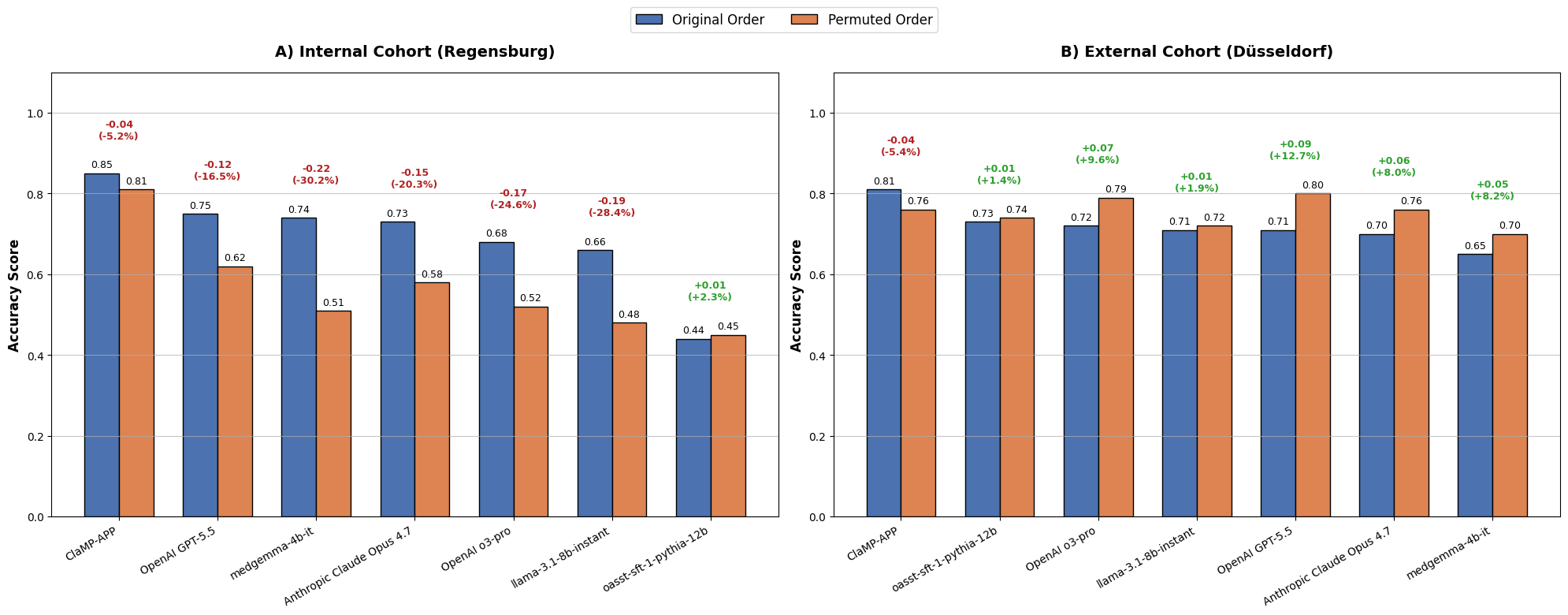
Figure 7: Robustness analysis—ClaMPAPP retains accuracy under sentence-order permutation, outperforming LLM baselines.
Implications and Discussion
These results substantiate several key claims:
- LLM-as-interface, ML-as-predictor paradigm is superior for clinical safety and robustness: By constraining LLM involvement to feature extraction and validation, ClaMPAPP delivers deterministic, auditable, and explainable predictions; it outperforms end-to-end LLMs in both accuracy and minimizing missed diagnoses.
- Robustness to information order and distribution shift is markedly improved: The hybrid architecture maintains diagnostic integrity despite narrative permutations and external cohort shift, while end-to-end LLMs suffer from pronounced instability and positional bias.
- Probability calibration remains a critical challenge: External calibration is essential for deploying risk-based counseling and resource allocation; the hybrid pipeline facilitates post hoc calibration, but external validation is needed.
- Generalizability across disease domains is enabled: The architecture is transferable to other conditions with validated structured predictors and narrative documentation.
Theoretical implications include confirmation of the inadequacy of unconstrained generative models for high-stakes triage, reinforcement of Good Machine Learning Practice principles (validation, transparency, interface separation), and demonstration that hybrid architectures bridge usability and reliability gaps in clinical AI. Practically, ClaMPAPP offers a viable pathway to integrate ML models into narrative-centric clinical workflows without sacrificing safety.
Conclusion
ClaMPAPP exemplifies a robust, safety-oriented hybrid LLM-ML system for pediatric appendicitis decision support, achieving high sensitivity, strong F1 scores, and architectural robustness across cohorts and narrative perturbations. By reassigning the LLM role to interface and feature extraction and delegating prediction to structured ML, the design fundamentally advances clinical usability, reliability, and auditability. The architecture is readily adaptable to other diagnostic domains with validated structured predictors and narrative documentation, warranting prospective validation and extension to broader clinical applications.