- The paper introduces a novel hierarchical graph framework that encodes clinical pathways to integrate multimodal features for improved survival prediction in head and neck cancer.
- It employs relation-specific attention mechanisms and dynamic graph construction to handle missing modalities and capture temporal dependencies.
- Experimental results show that ChronoSurv outperforms classical and deep/multimodal methods, achieving a C-index of 0.702 and robust calibration.
ChronoSurv: Clinical Pathway-Guided Hierarchical Graphs for Multimodal Survival Analysis
Context and Motivation
Survival prediction in head and neck cancer (HNC) is fundamentally hindered by the high dimensionality, variable data quality, and pronounced heterogeneity across multimodal clinical data (structured tabular variables, pathology images, and clinical text). Most prior approaches leverage late or static fusion of modality-specific features, disregarding the sequential, decision-driven structure inherent to clinical care pathways. This leads to models that capture neither the relational dependencies among modalities nor the temporal trajectory of care—key determinants of outcome in complex malignancies.
ChronoSurv addresses these limitations by introducing a heterogeneous hierarchical directed graph framework that explicitly encodes the hierarchical and temporal structure of the clinical workflow and enables robust, progression-aware multimodal fusion for survival analysis in HNC.
Model Architecture
ChronoSurv consists of four key components: multimodal feature initialization, hierarchical directed patient-level graph construction, heterogeneous message passing, and a survival prediction head.
All sub-modalities are embedded into a shared latent space using frozen encoders and learnable projectors: clinical data via MLPs, WSIs via pretrained visual encoders, and text via LLMs. Each patient is represented as a graph with three hierarchical levels: (i) leaf nodes for each available modality-specific feature, (ii) clinical step nodes corresponding to sequential care stages (background, diagnosis, surgical intervention), and (iii) a global patient node. Edges encode both intra-stage and temporal inter-stage relationships, with directionality mapped to the ordering of real-world clinical decisions.
The graph topology is dynamically constructed per-patient to accommodate missing modalities natively, avoiding zero-imputation artefacts and enabling flexible deployment in heterogeneous cohorts.
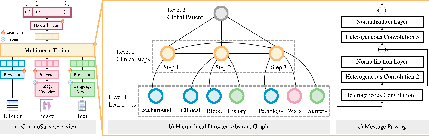
Figure 1: ChronoSurv schematic—dedicated multimodal fusion (a), hierarchical and temporally ordered directed patient graphs (b), and cross-level (heterogeneous) message passing (c).
Heterogeneous message passing is realized via relation-specific graph attention mechanisms. Three stacked layers effect bottom-up aggregation: (1) fine-grained modality features to clinical step nodes, (2) temporally ordered clinical step message passing (including skip edges for non-consecutive steps), and (3) fusion of the enriched step nodes into the patient node. This hierarchical, relation-aware design enables the model to encode complex, asymmetric dependencies reflective of real-world clinical reasoning. Final discrete-time survival hazard estimation is performed via a bin-wise hazard head, supervised using a negative log-likelihood formulation with an explicit differentiable calibration penalty for reliable survival probability estimation.
Experimental Analysis
ChronoSurv is benchmarked on two public HNC datasets: HANCOCK (763 samples; rich multi-modality, including WSIs, text reports, bloodwork) and TCGA-HNSC (526 samples; limited modality availability), plus a concatenated multi-cohort setup (UniHNC, 1,289 samples) to gauge robustness under varying modality and cohort compositions. All feature extractors are frozen during training to isolate the graph-level contribution.
ChronoSurv achieves a Cindex of 0.702 (±0.039) and IBS of 0.153 (±0.019) on UniHNC—outperforming all unimodal, classical, and competing deep/multimodal methods. This superiority holds across both the HANCOCK and TCGA-HNSC subsets for discrimination (risk ranking) and probability calibration (measured via Integrated Brier Score and D-Calibration; consistently passing calibration tests across all folds), clearly demonstrating the value of explicit clinical-pathway modeling. Ablation studies confirm that hierarchical step modeling, message passing heterogeneity, and temporal directionality are all indispensable—removal of any yields pronounced performance deterioration, particularly omission of diagnostic and surgical steps. ChronoSurv also surpasses alternative aggregation mechanisms (mean/max/attention pooling, late fusion, bilinear models), establishing the criticality of structured, relation-aware fusion over naive combinations.
Model Interpretability
Qualitative analysis reveals how information traverses the hierarchical graph: the background step remains largely isolated; initial diagnosis aggregates predominantly from background; local surgery nodes integrate information from both precursors. At the global node, both background and surgery steps contribute most to survival estimates, closely mirroring clinical evidence on the importance of both historic and perioperative factors for HNC prognosis.
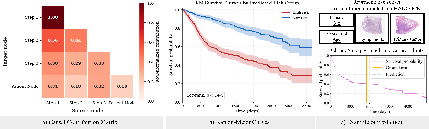
Figure 2: (a) Message-passing contributions at each graph level, (b) Kaplan-Meier curves stratified by predicted risk groups, (c) Example individual survival curve and estimated time.
Stratifying patients by predicted risk yields Kaplan-Meier curves with substantial separation (log-rank p<10−4), confirming the clinical meaningfulness of ChronoSurv’s risk grouping.
Broader Implications and Future Directions
ChronoSurv advances multimodal survival prediction by integrating the clinical workflow into the architectural design, moving beyond flat late-fusion paradigms common in prior work (2606.19140). The hierarchical, directed, and heterogeneous graph construction natively supports missing modalities, patient-specific graphs, and progression-aware modeling, making it adaptable to real-world, imperfectly measured clinical data.
The explicit modeling of clinical trajectories represents a shift to incorporating domain knowledge at the graph-topological level. This concept is extensible: additional clinical steps, imaging modalities, molecular assays, or treatment interventions can be incorporated as further nodes/edges. The approach is expected to scale to larger, more diverse cohorts and could be generalized to other malignancies with well-defined care pathways.
Further improvements can be anticipated by developing trainable initial feature encoders (rather than fully frozen backbones), leveraging larger-scale foundation models, or introducing additional supervision (e.g., contrastive or counterfactual learning) on clinical step representations. Integrating event-type modeling would enable direct handling of competing risks, and augmenting prediction tasks to adverse events or recurrence would expand the clinical impact.
Conclusion
ChronoSurv introduces a rigorous graph-based multimodal survival model that encodes temporal and hierarchical aspects of the clinical pathway, achieving state-of-the-art discrimination and calibration in head and neck cancer. Its explicit, modular design for care trajectory modeling both augments performance and enhances interpretability, advocating for similar approaches in broader clinical AI and multimodal learning contexts.

