- The paper identifies that explicit task and outcome assumptions underpin the evaluation–deployment gap in healthcare LLM benchmarks.
- It empirically decomposes performance gaps, attributing nearly equal losses to task mismatches and inadequate outcome alignment using retrospective clinical RCT data.
- The study introduces BenchmarkCards and a staged evaluation protocol to enhance transparency and guide LLM deployment in clinical settings.
Explicit Assumptions and the Evaluation–Deployment Gap in Healthcare LLM Benchmarks
Motivation and Critique of Benchmark-Driven Evaluation
The paper "Healthcare LLM Benchmarks Are Only as Good as Their Explicit Assumptions" (2605.22612) asserts that the persistent gap between benchmark evaluation and real-world deployment of LLMs in healthcare is not primarily caused by inadequate benchmarks, but rather by the implicit assumptions underpinning these evaluation protocols. Benchmarks, while effective as initial screening tools, fall short in representing the complex, interaction-driven, and context-dependent realities of clinical deployments. Empirical evidence from prior studies shows substantial drops in LLM performance when transitioning from controlled benchmark settings to clinical environments, highlighting the critical need to scrutinize the underlying assumptions within evaluation frameworks.
Classification of Assumptions in Evaluation Protocols
The authors propose a dichotomous taxonomy for assumptions:
- Task Assumptions: These concern the faithfulness of the benchmark's conversational environment in reflecting deployment conditions (e.g., whether prompts are single-turn versus multi-turn, or if queries are authored by experts versus patients). Task assumptions are empirically testable using conversational data.
- Outcome Assumptions: These address whether the benchmark's objective aligns with real-world clinical decision-making and outcomes. Testing outcome assumptions requires outcome data and behavioral studies, such as RCTs, since they depend on human interactions and decisions.
This framework formalizes how the evaluation–deployment gap can be decomposed, making clear which facets of performance are addressable through improved benchmarking versus those that necessitate real-world experimentation.
Through retrospective analysis of a clinical RCT, the paper demonstrates that the evaluation–deployment gap splits almost equally between unmet task and outcome assumptions. For example, in the study "Reliability of LLMs as medical assistants for the general public" [nature_ai_medical_assistants], LLMs scored 95% during benchmark evaluation but only 34% in deployment.
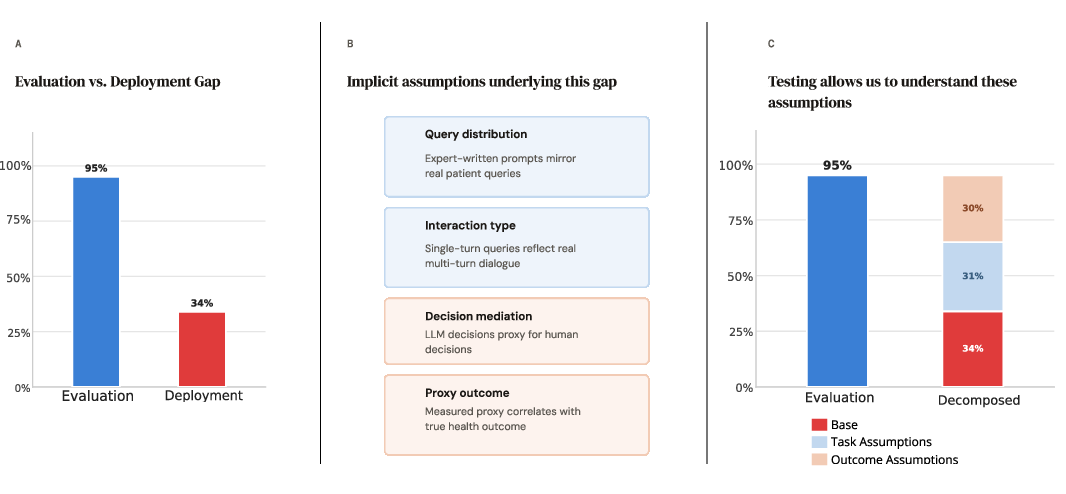
Figure 1: Explicitly stated assumptions enable decomposition of the evaluation–deployment gap observed between benchmark performance and deployment in clinical RCTs.
Using sensitivity analysis, the authors attribute 31 percentage points of performance loss to task assumptions (query and interaction mismatch) and another 30 to outcome assumptions (differences in decision mediation and measured outcomes). This technique is reflective of causal inference methodologies for diagnosing gaps due to assumption violations.
BenchmarkCards: Systematic Documentation of Assumptions
To operationalize transparency in evaluation, the authors introduce BenchmarkCards—a structured artifact analogous to Model Cards and Datasheets—that mandates explicit articulation of both task and outcome assumptions associated with each benchmark. BenchmarkCards enable practitioners to formally assess whether a benchmark's underlying assumptions are met in their specific deployment context, aiding in the selection or development of more appropriate evaluation tools and signaling where new benchmarks are required.
Staged Evaluation Protocol for Deployment Readiness
The paper advocates a staged evaluation protocol for LLMs in healthcare:
- Benchmark Assessment: Initial evaluation using established benchmarks.
- Assumption Scrutiny: Comparison of BenchmarkCard assumptions against deployment requirements.
- Data Collection and Testing: Empirical validation of task assumptions using deployment-context conversational data.
- Outcome Validation: Behavioral or clinical studies to address outcome assumptions lacking supporting evidence.
- Iterative Refinement: Targeted improvements in model or evaluation procedures based on observed gaps.
This protocol supports empirical ranking of assumptions by impact, enabling efficient prioritization and resource allocation. The authors also propose an assumptions database analogous to clinical trial registries, facilitating knowledge transfer and reducing redundant effort across future studies.
Implications, Limitations, and Extensions
The paper's approach extends beyond healthcare to any domain where deployment contexts are non-sandboxable (e.g., law, finance), making explicit assumption documentation and staged evaluations universally relevant for high-stakes AI applications. One limitation acknowledged is the binary categorization of assumptions; in practice, assumptions may span a continuum and require mixed-methods data for testing.
Conclusion
This work provides a rigorous framework for addressing the notorious evaluation–deployment gap in healthcare LLMs, underpinning benchmark-driven evaluation with explicit documentation and empirical validation of assumptions. By categorizing assumptions into task and outcome, introducing BenchmarkCards, and advocating for staged evaluation protocols, the paper establishes practical methodologies to ensure benchmarked performance translates to real-world utility and safety. This supports practitioners and regulatory bodies in making informed deployment decisions, emphasizing that improved benchmarks are necessary but not sufficient without systematic assumption scrutiny.