- The paper introduces a discrete translation paradigm using hierarchical residual vector quantization to efficiently encode and synthesize cross-modal physiological signals.
- It demonstrates marked improvements in clinical metrics, achieving an R-peak detection F1-score increase from 0.37 to 0.83 and superior waveform reconstruction.
- The model’s architecture supports real-time edge deployment and lays the groundwork for novel digital biomarkers through interpretable latent space mapping.
Compact Latent Manifold Translation: A Parameter-Efficient Framework for Physiological Signal Synthesis
Introduction
The Compact Latent Manifold Translation (CLMT) architecture addresses substantial limitations in current physiological signal foundation models, specifically tackling modality and frequency gaps across heterogeneous biosignal sources such as electrocardiograms (ECG) and photoplethysmograms (PPG). Existing generative models, which typically operate in continuous latent spaces, are challenged by modal entanglement, limited high-frequency representational fidelity, and impracticable computational footprints for edge deployment. CLMT introduces a two-stage discrete translation paradigm leveraging hierarchical residual vector quantization (RVQ), which fundamentally restructures the representation and synthesis of physiological signals.
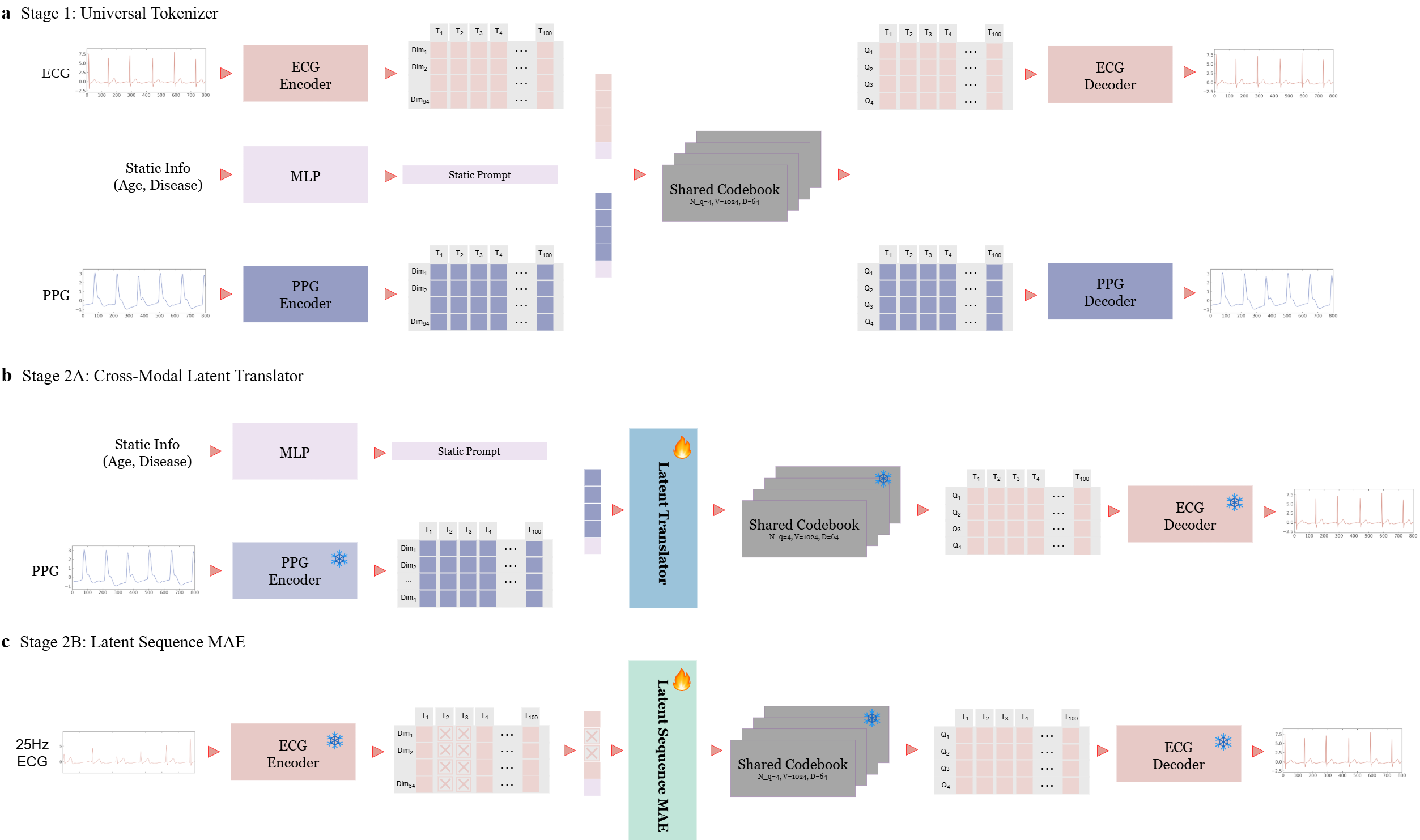
Figure 1: CLMT architecture showing Universal Tokenizer, Cross-Modal Latent Translator, and Latent Sequence MAE modules as a highly parameter-efficient pipeline for cross-modal and cross-frequency signal synthesis.
Architectural Design and Methodology
Universal Tokenizer via Hierarchical RVQ
CLMT introduces a Universal Tokenizer employing hierarchical RVQ to encode multimodal physiological sequences into a shared, discrete latent space. The hierarchical quantization structure captures both macro-rhythmic (low-frequency) physiological features and micro-morphological (high-frequency, modality-specific) details. The encoder utilizes temporal convolutional layers with continuous-time positional encoding, followed by static demographic prompts integrated via MLP-based conditioning. Hierarchical quantization ensures explicit separation of cardiac electrical and mechanical dynamics, resulting in distinct ECG and PPG manifolds, as validated through UMAP projections.
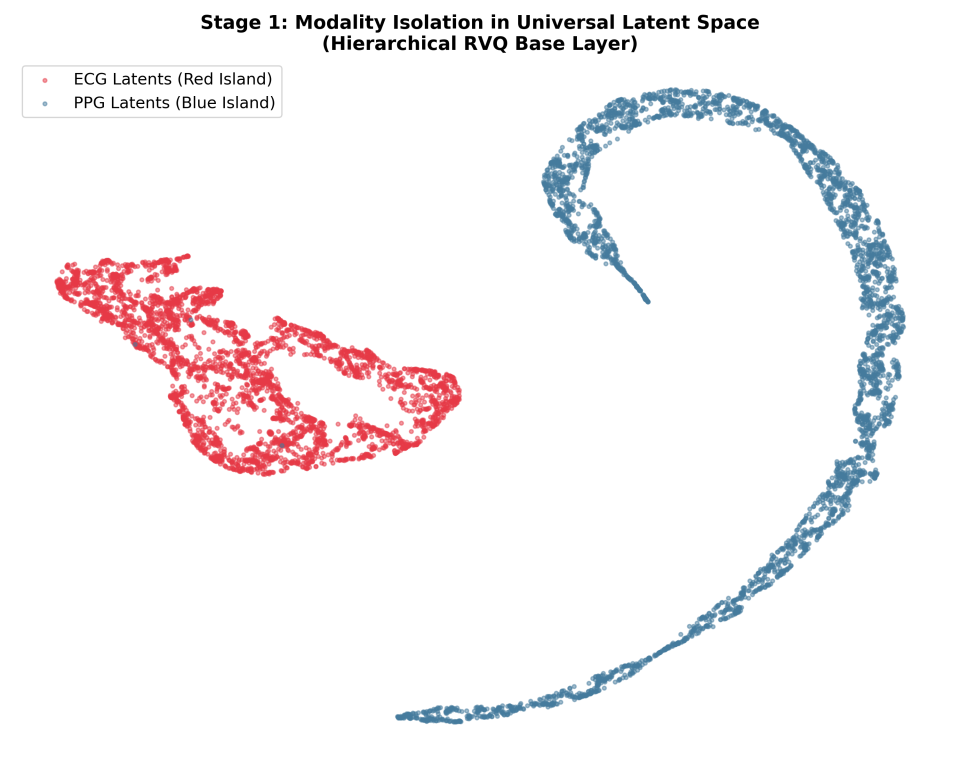
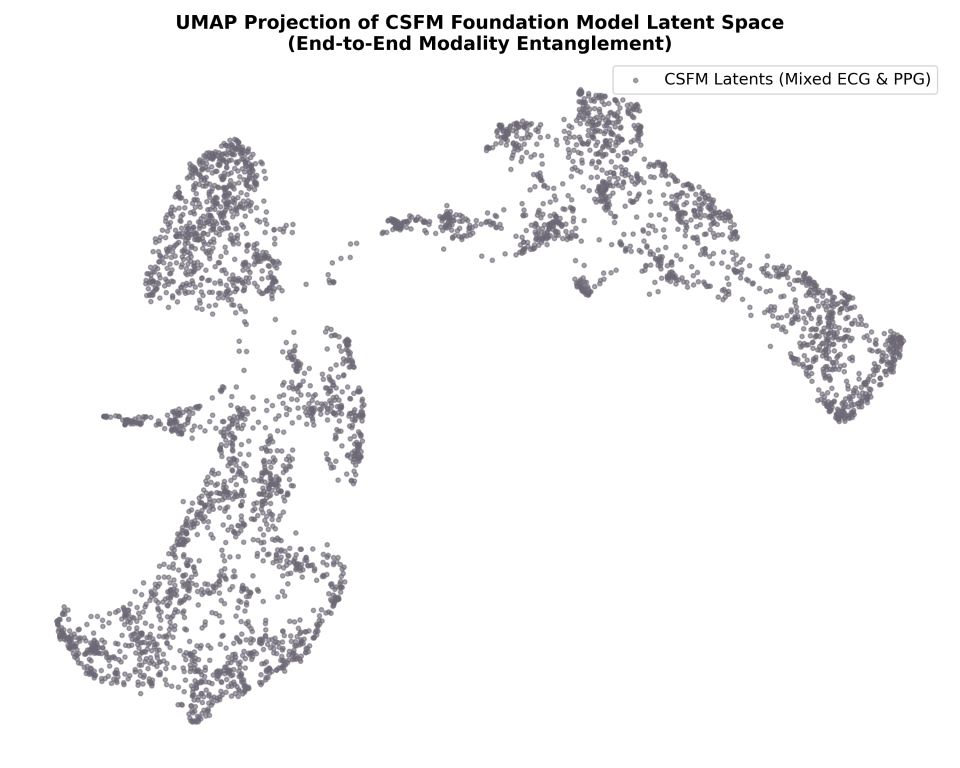
Figure 2: UMAP visualization demonstrates modality-organized discrete latent sub-manifolds for ECG and PPG, compared to blurred, entangled baselines.
Discrete Latent Translation and Super-Resolution
The cross-modal translation is realized through a lightweight Transformer, guided by static prompts and optimized via continuous feature distillation. The transformer output is routed through a frozen RVQ codebook, enforcing a "snapping" effect that aligns the synthesized latent sequence with pre-established physiological priors. This bypasses regression-to-the-mean blurring, prevalent in continuous generative models, and preserves sharp diagnostic landmarks.
For cross-frequency super-resolution, CLMT employs a latent sequence masked autoencoder (MAE) operating in the quantized latent domain. The MAE reconstructs masked high-resolution latent tokens from sparse low-frequency inputs, again leveraging the frozen codebook to enforce clinically meaningful reconstruction.
Empirical Analysis
Cross-Modal PPG-to-ECG Translation
CLMT exhibits statistically significant superiority in cross-modal generation. Compared with P2E baselines, CLMT improves the R-peak detection F1-score from 0.37 to 0.83, reduces RMSE from 0.68 to 0.42, and halves the Fréchet Distance, demonstrating robust preservation of high-frequency diagnostic anchors in synthesized ECG. Waveform reconstructions further confirm sharper morphological fidelity with precise QRS complexes, closely paralleling intra-modal autoencoding upper bounds.
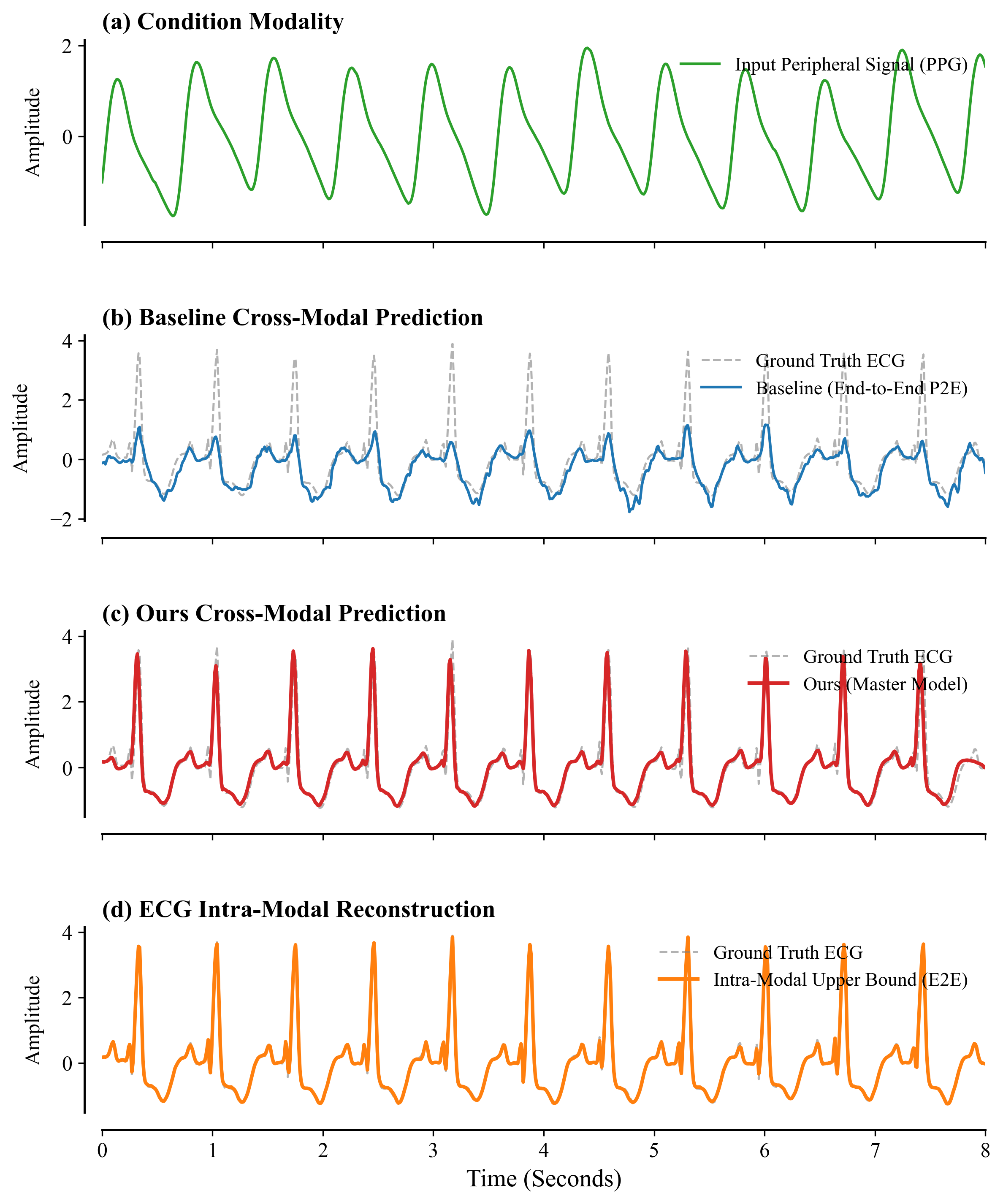
Figure 3: Qualitative waveform comparison highlights the CLMT model’s restoration of sharp QRS complexes, contrasted against baseline attenuation and phase drift.
Latent temporal dynamics visualized via 3D t-SNE reveal that CLMT maps translated and ground-truth ECG into coherent, phase-aligned helical manifolds, strictly segregating modality embeddings and capturing the intrinsic cardiac phase progression, in stark contrast to the phase collapse in continuous baselines.
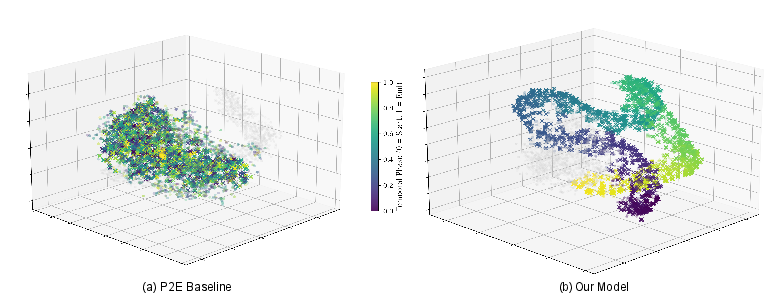
Figure 4: 3D t-SNE of latent temporal dynamics shows phase-aligned separation of translated ECG in CLMT versus entanglement in baseline approaches.
Cross-Frequency Signal Super-Resolution
For extreme super-resolution ($25$Hz→100Hz), the latent MAE operating in discrete space outperforms CNN-based interpolations. CLMT achieves a Pearson correlation of $0.9956$ and an R-peak F1 of $0.92$, markedly exceeding baselines for both morphological and spectral fidelity. The discrete MAE cleanly restores harmonics >20Hz that are lost with continuous regression methods.
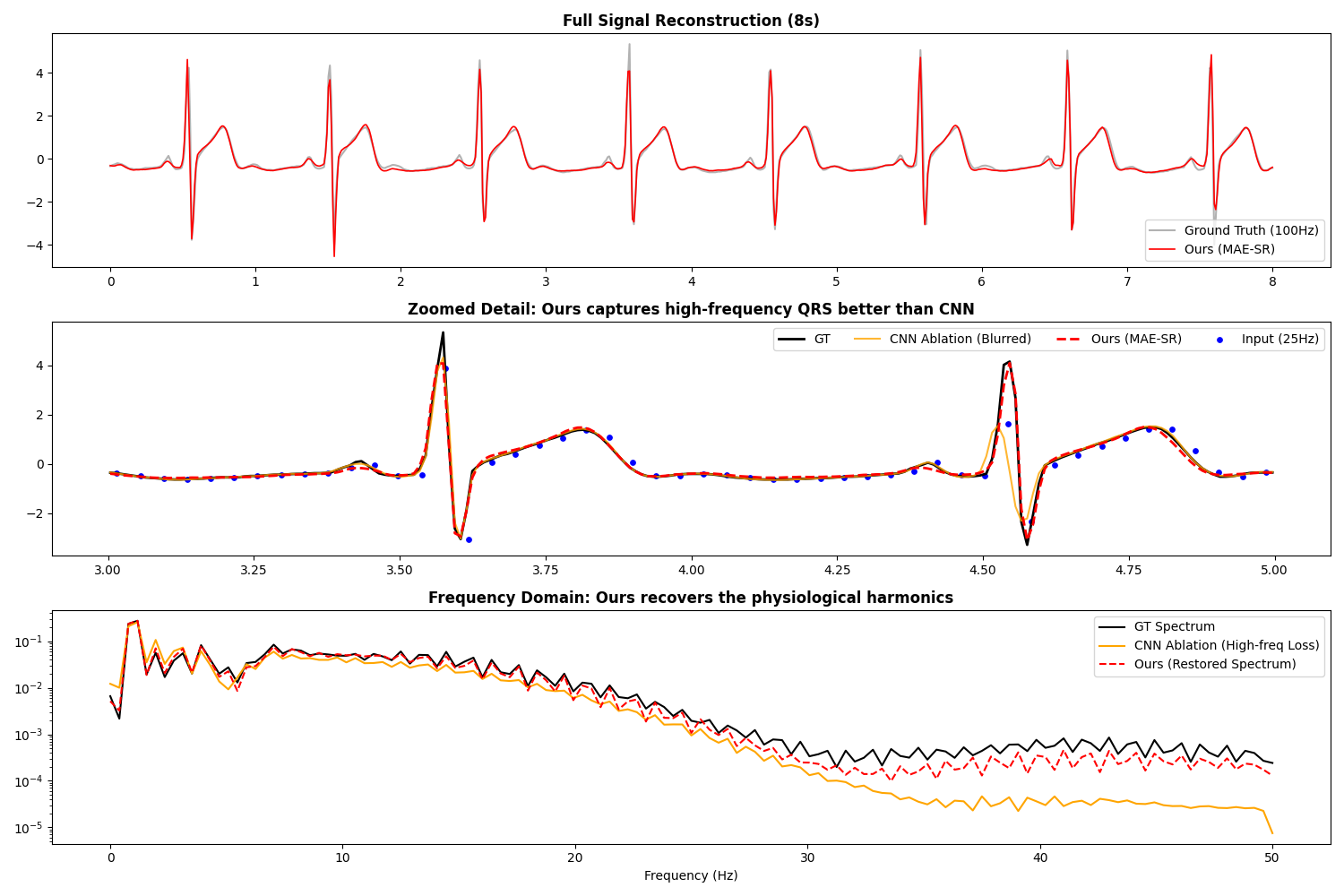
Figure 5: Super-resolution results demonstrate faithful tracking of ground truth and restoration of high-frequency spectral components absent in baseline reconstructions.
Ablation and Component Analysis
Ablation studies confirm the necessity of the two-stage translation paradigm; eliminating Stage 2 translation degrades clinical F1 from $0.83$ to $0.37$. Static prompt embedding is similarly critical for personalized waveform estimation, with its ablation causing substantial increases in RMSE and distributional deviation (Fréchet Distance). These results demonstrate functional dissociation: temporal rhythm alignment is transformer-governed, while static prompts modulate amplitude scaling and individual morphological features.
Practical and Theoretical Implications
CLMT represents a shift from continuous, modality-entangled representations to discrete, modality-organized latent spaces, enabling ambiguity-free cross-modal translation and high-fidelity generative synthesis. The 0.09B parameter footprint, a 23% reduction from contemporary foundation models, permits real-time edge deployment without compromising clinical-grade fidelity. The hierarchical quantization structure lays the groundwork for interpretability, with potential mapping between discrete latent codebook trajectories and specific disease phenotypes, enabling the emergence of novel digital biomarkers.
Out-of-distribution sensitivity and reliance on patient-specific conditioning represent current limitations, which future research could address by corpus expansion and further stratification of the codebook space.
Conclusion
CLMT establishes a parameter-efficient, discrete latent foundation for cross-modal and cross-frequency physiological signal synthesis. By decoupling morphological and rhythmic dynamics and enforcing physiological priors via hierarchical RVQ, it surpasses continuous generative approaches in clinical landmark preservation and distributional fidelity. The architecture enhances both efficiency and interpretability, signifying a robust trajectory for multimodal medical AI, with substantive implications for edge-deployable diagnostics, precision medicine, and biomedical signal foundation modeling.

