- The paper introduces DxChain, a cognitive AI framework that employs panoramic memory anchoring, a Medical Tree-of-Thoughts planner, and dialectical adversarial debate for refined clinical diagnosis.
- It demonstrates state-of-the-art diagnostic accuracy by achieving up to 84.98% accuracy on cardiac cases and 90.67% on abdominal cases, surpassing traditional LLM-based CDSS.
- The method reduces diagnostic hallucinations and enhances error localization, paving the way for robust, interpretable, and clinically trustworthy AI systems.
Cognitive Alignment in Clinical AI: DxChain’s Panoramic Profiling and Dialectical Reasoning
Introduction
The paper "Thinking Like a Clinician: A Cognitive AI Agent for Clinical Diagnosis via Panoramic Profiling and Adversarial Debate" (2604.23605) delineates DxChain, an innovative agentic framework engineered for high-fidelity clinical diagnosis using raw and unstructured EHR data. DxChain departs from standard LLM-based CDSS paradigms by explicitly modeling the iterative, non-linear, and adversarial trajectory of real-world clinical reasoning. Central to the approach are three architectural innovations: Memory Anchoring through panoramic patient profiling, strategic Navigation via a Medical Tree-of-Thoughts planner, and rigorous Verification with a dialectical adversarial debate framework. Evaluations on complex EHR-derived benchmarks indicate substantial and robust improvements in both accuracy and logical coherence, establishing substantive claims regarding cognitive alignment in diagnostic AI.
Methodological Innovations
Panoramic Memory Anchoring
DxChain’s first phase—Memory Anchoring—explicitly tackles the susceptibility of LLMs to "cold-start hallucinations" caused by unfiltered EHR noise and misleading chronic signals. Rather than reactive analysis, the system initializes with a Profile-Then-Plan paradigm: a profiling agent constructs a structured, multi-dimensional patient representation consisting of acute presentations, chronic baselines, and risk factors. This global patient representation, generated before any diagnostic planning commences, constrains all subsequent reasoning to a holistic cognitive baseline rooted in verified clinical facts rather than isolated or spurious findings.
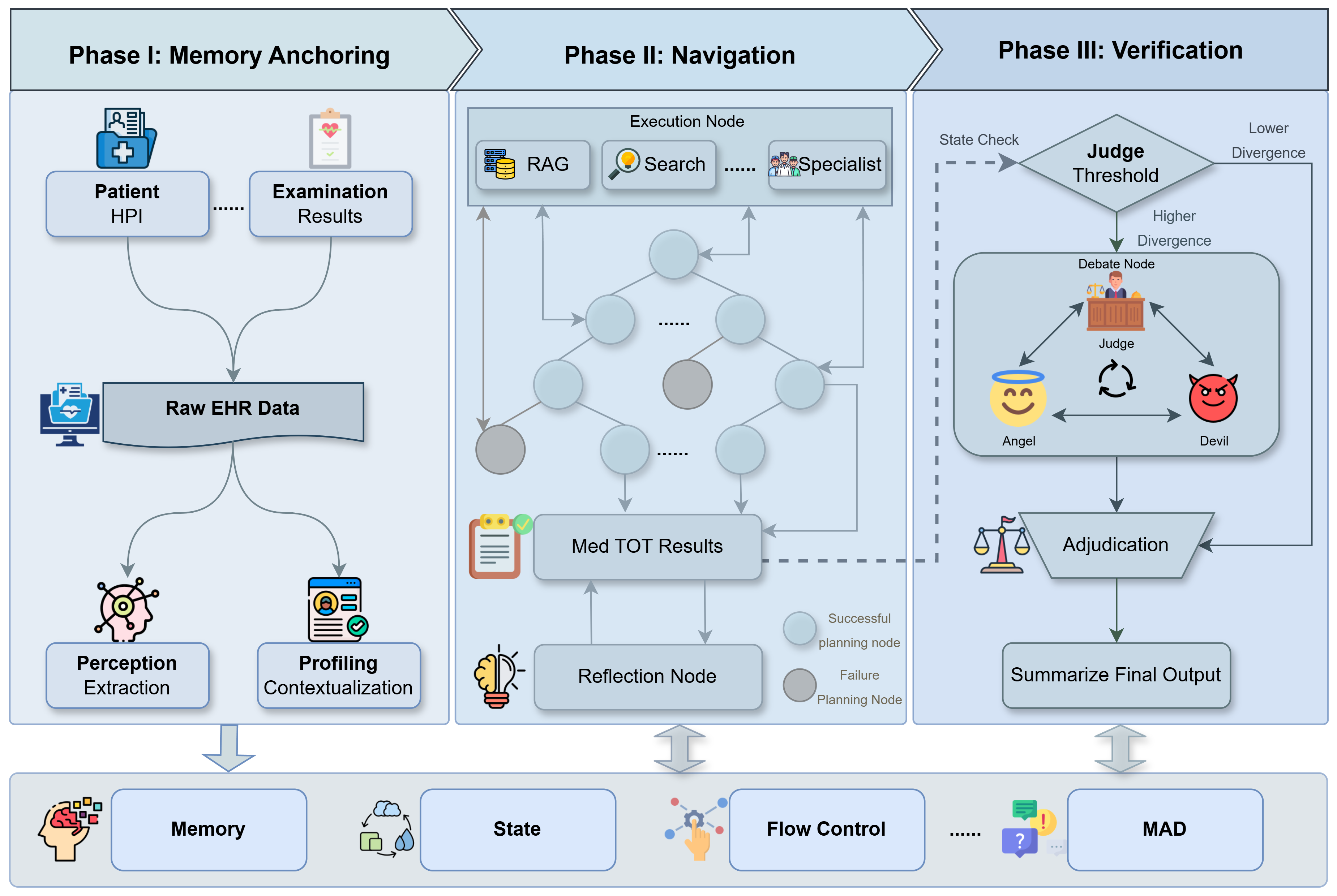
Figure 1: Overview of the DxChain framework illustrating phase-wise anchoring, navigation over a Medical Tree-of-Thoughts, and dialectical multi-agent diagnosis arbitration.
Navigation via Medical Tree-of-Thoughts
The Navigation phase advances beyond linear Chain-of-Thought reasoning, leveraging a Medical Tree-of-Thoughts (Med-ToT) planner. The diagnostic process is modeled as a stateful, cyclic graph whose nodes capture domain-specific cognitive modules and whose edges enact metacognitive cycles for iterative, hypothetico-deductive exploration. The planner simulates lookahead branching, conditioned not only on previous findings but the persistent contextual patient profile. Each node expansion is guided by medically-informed strategy stacks (e.g., "Rule out Emergency") while dynamically pruning implausible trajectories. Upon significant discordance between expectation and observation, a Discrepancy-Driven mechanism triggers automatic backtracking or replanning, reducing premature closure errors and ensuring robust handling of conflicting evidence.
Dialectical Verification via Angel-Devil Debate
For ambiguous or evidence-conflicted cases, DxChain introduces a third phase: dialectical adjudication by multi-agent adversarial debate. Here, candidate diagnoses produced by the planner are subjected to an adversarial contest: a proponent ("Angel" agent) aggregates positive, confirming findings, while an opponent ("Devil" agent) interrogates for negative evidence, noise, or insufficiently justified conclusions. An impartial Judge agent synthesizes these arguments and updates hypotheses, retaining only diagnoses that withstand this adversarial scrutiny. This selective instantiation prevents redundant computational expense while strictly enforcing logical soundness and balancing diagnostic precision and recall.
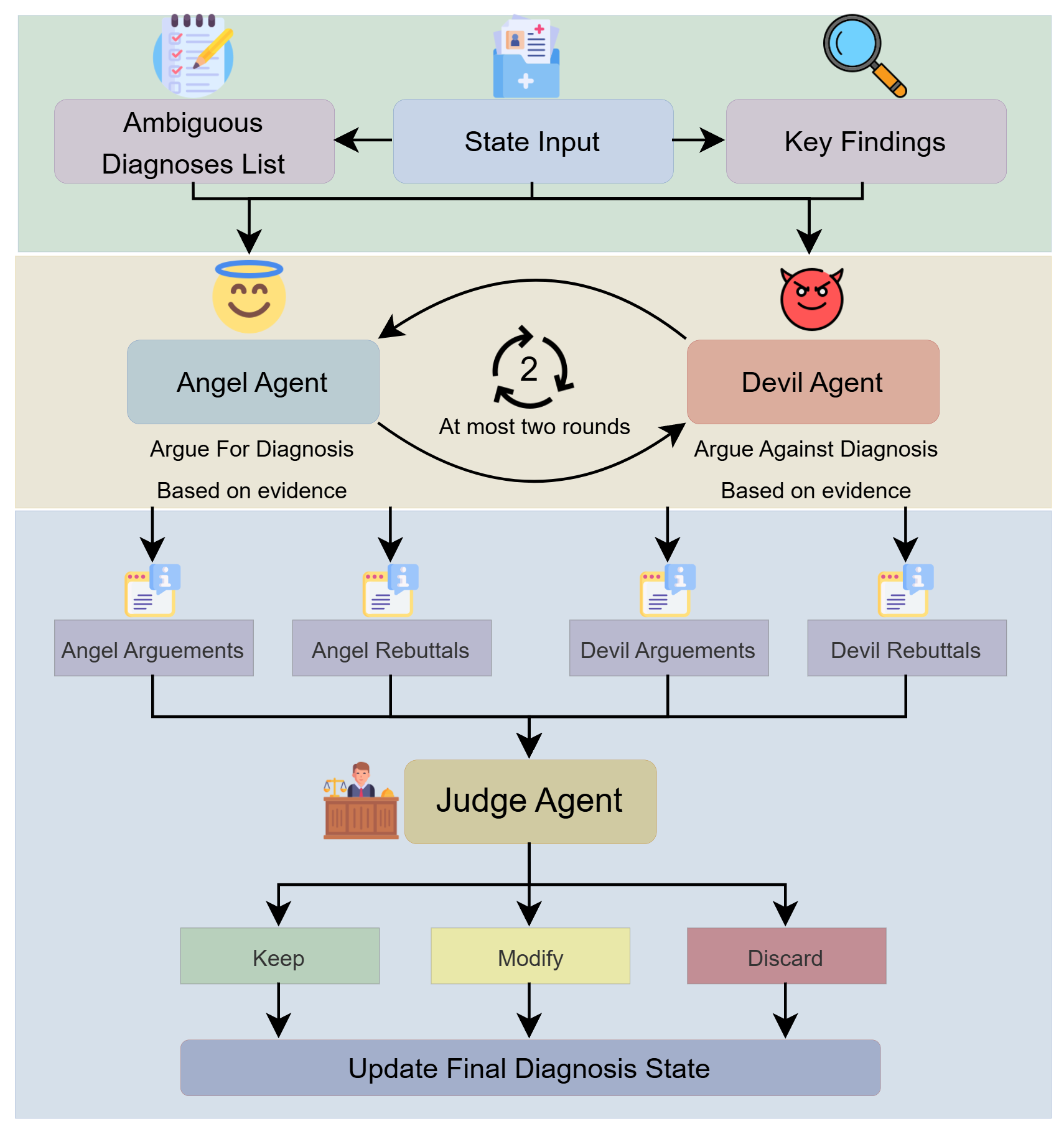
Figure 2: The Dialectical Verification phase, implementing an Angel-Devil adversarial debate whose outcome is judged to finalize diagnosis hypotheses.
Empirical Evaluation
Experimental Protocols
DxChain is evaluated on two EHR-derived datasets from the MIMIC-IV database to reflect the real-world, unstructured diagnostic landscape:
- Cardiac Disease: 4,761 cases; high complexity with an average of 14.21 diagnoses per patient.
- Clinical Decision Making (CDM): 2,400 abdominal cases with lower diagnostic density but requiring multi-step reasoning.
Performance metrics include Primary Diagnosis Accuracy (semantic soft-matching), Semantic Textual Similarity (STS), and BERTScore for both recall and F1.
Results and Analysis
State-of-the-Art Diagnostic Accuracy and Robustness
DxChain achieves an absolute Primary Diagnosis Accuracy of 84.98% on Cardiac Disease (GPT-4.1-Mini), markedly surpassing all baselines including MedAgents, MDAgents, and KAMAC by a margin exceeding 7%. On the CDM dataset, the framework attains 90.67% accuracy, with exceptional STS and BERT-based comprehensiveness—evidence of superior recall for comorbidities and less frequent pathology.
Further, the architecture exhibits consistent performance regardless of backbone (GPT-4.1-Mini or GPT-5-Nano), directly supporting its claimed model-agnostic robustness.
Ablation: Phase-wise Impact
Ablation studies validate that:
- Memory Anchoring elevates semantic coverage, as evidenced by a >25% relative increase in BERT F1 when compared to baseline LLM prompting.
- Med-ToT navigation yields the most significant jump in diagnostic precision (Primary ACC: 75.40% → 86.70%).
- The Angel-Devil debate, while inducing marginal tradeoffs in raw accuracy, achieves the highest logical consistency (BERT F1: 55.03%), winnowing low-confidence hypotheses.
Stability and Reliability
Temperature sensitivity analysis demonstrates minimal performance variability in both accuracy and semantic metrics across a wide range of sampling stochasticity, indicating strong framework-level determinism.
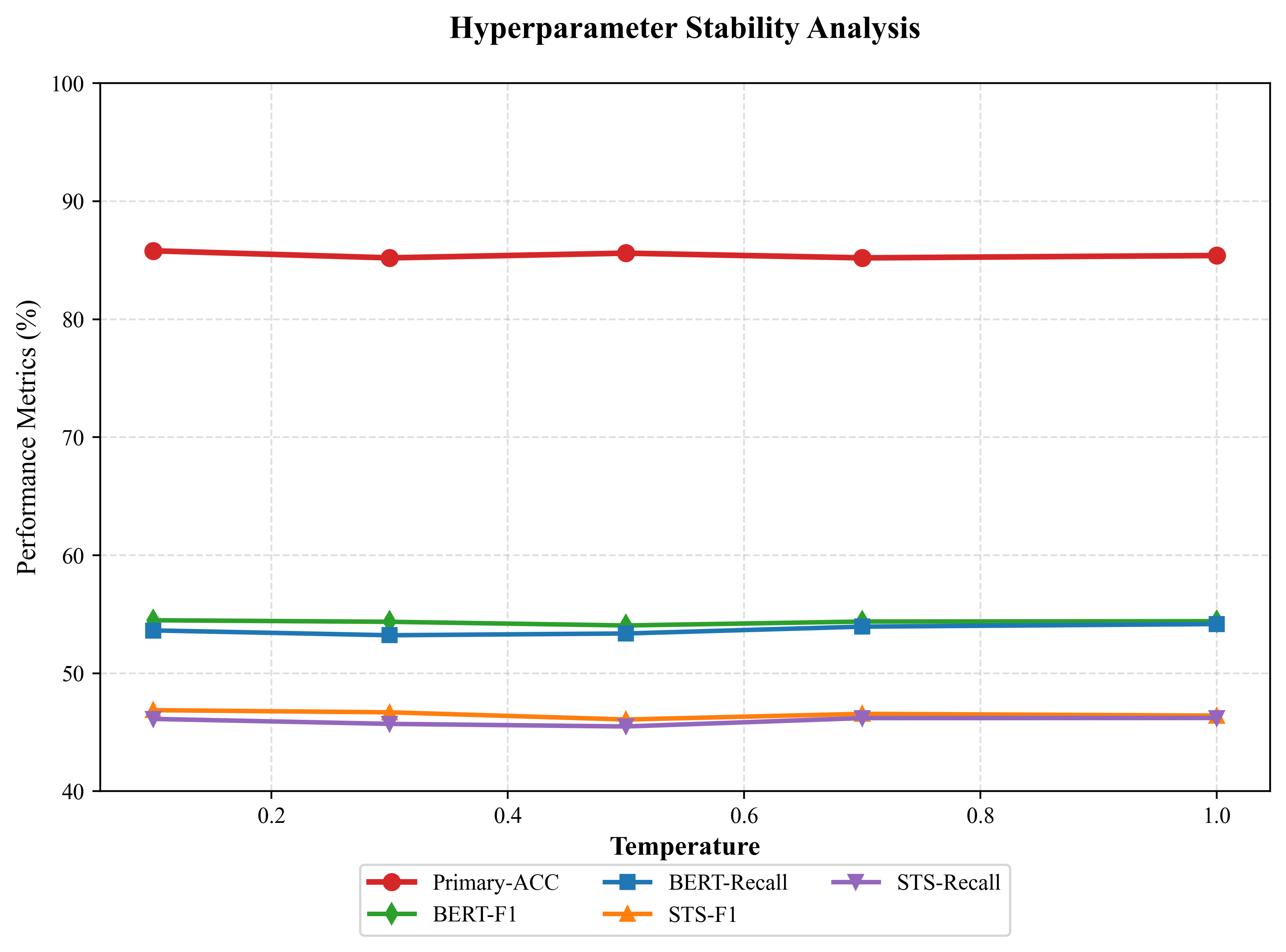
Figure 3: DxChain’s diagnostic accuracy and semantic performance are highly stable to variations in generation temperature.
Implications and Future Directions
The results substantiate bold claims: DxChain breaks the conventionally entrenched precision-recall tradeoff in clinical LLM deployment by structurally mimicking the cognitive workflow of clinicians. The architecture enforces high precision without sacrificing breadth or robustness—especially critical once the system must handle noisy, ambiguous, or multi-morbidity EHR cases.
Key practical implications include:
- Modular and interpretable architectures that allow for phased reasoning and error localization.
- Reduced susceptibility to diagnostic hallucinations and tunnel vision under real-world data noise.
- Model-agnostic deployment potential in clinical AI by decoupling reasoning machinery from underlying LLM backbone.
Theoretically, such cognitive simulation paves the way for agentic clinical AI that does not merely emulate procedure but incorporates true reflective, adversarial, and backtracking strategies. Future research directions include multimodal integration (expanding beyond text to imaging and waveform data), large-scale prospective clinical validation, and extending dialectical arbitration to broader multi-specialty panel debates for rare disease detection and treatment recommendation. The modularity of DxChain also supports incorporation of retrieval-augmented external knowledge and other meta-cognition modules.
Conclusion
DxChain provides a cognitive-aligned, modular blueprint for clinical diagnostic AI, demonstrating that clinically inspired agentic scaffolding can deliver robustness, reliability, and interpretability not achievable with conventional LLM prompting and chain-of-thought reasoning alone. The synergy of panoramic profiling, dynamic cognitive navigation, and selective adversarial verification constitutes a compelling path forward for building clinically trustworthy, accountable medical AI agents.