- The paper introduces a multi-layered framework emphasizing coherence, continuity, adaptation, and agency for longitudinal health management.
- It outlines structured mechanisms for proactive follow-up, context-aware memory, and adaptive decision support integrated with clinical and behavioral care.
- Findings highlight practical challenges in balancing model stability with dynamic adaptation while ensuring user empowerment and safe clinical implementation.
A Longitudinal Health Agent Framework
Introduction
AI-driven health agents, especially those implemented with LLMs, are increasingly employed to support various dimensions of healthcare such as triage, clinical documentation, decision support, patient education, and behavioral health coaching. However, current AI agents predominantly operate as reactive, episodic systems, handling health interactions as isolated events instead of orchestrating coherent, goal-oriented, and accountable health interventions across time. This episodic paradigm stands in contrast to the requirements of longitudinal health management, where chronic condition trajectories, evolving user goals, and accountability for outcomes necessitate persistent, adaptive, and user-centered engagement. The paper proposes a structured framework for longitudinal health agents, addressing functional and relational requirements essential for meaningful engagement and decision support over repeated, evolving interactions (2604.12019).
Multi-Layered Framework for Longitudinal Health Agents
The framework synthesized from clinical continuity principles and personal health informatics models delineates four tightly interdependent layers, each operationalizing key dimensions necessary for effective longitudinal engagement: Coherence, Continuity, Adaptation, and Agency.
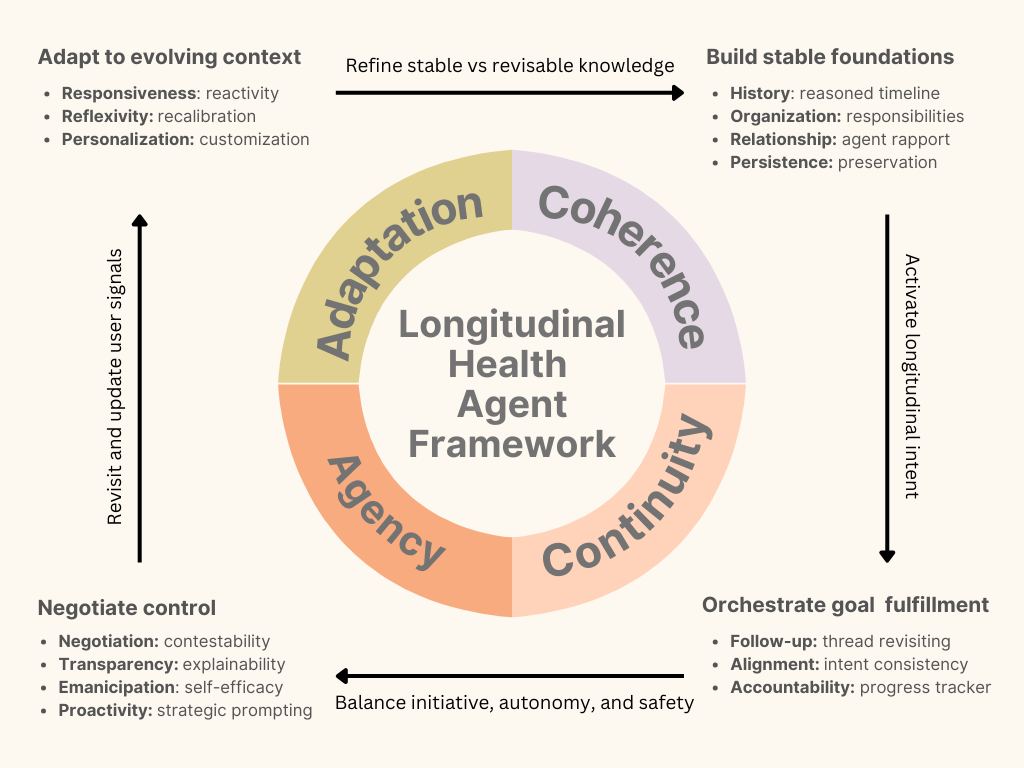
Figure 1: A four-part framework integrating Coherence, Continuity, Adaptation, and Agency to support sustained health engagement over time.
Coherence
The Coherence layer ensures consistent, contextually aware interaction and reasoning across sessions. Rather than relying solely on passive data storage, it emphasizes the active maintenance and structured evolution of interpretive relationships, including hypotheses about triggers, reasoning chains, and explanatory models that connect episodes to outcomes. This goes beyond traditional context embedding, advocating for explicit representation of roles and responsibilities and stable, interpretable memory architectures that preserve meaning but remain amenable to justified revision. Failure to adequately model information stability versus necessary change risks both the ossification of outdated beliefs and fragmentation of an individual’s narrative trajectory.
Continuity
Continuity extends beyond task reminders and adherence metrics, operationalizing the agent’s responsibility to steward longitudinal health goals and maintain momentum toward evolving user aims. This involves structured mechanisms for proactive follow-up, tracking unresolved concerns, systematically re-engaging with open threads, and maintaining explicit links between immediate actions and broader, shifting objectives. The agent must accommodate incremental progress and non-linear trajectories, rather than binary completion, to robustly support chronic disease self-management and behavioral adaptation.
Adaptation
The Adaptation layer centers on the agent's ability to calibrate its strategies, recommendations, and underlying models in response to sustained evidence of change in user state, context, or preferences. This encompasses not only short-term reactive adjustments but also higher-order, reflexive revision of assumptions and inferred preferences—extending to guideline updates and external contextual shifts. Second-order adaptation is crucial for maintaining alignment with individual trajectories and minimizing residual systematic error arising from static modeling approaches.
Agency
Agency is conceptualized as dynamic, longitudinally calibrated negotiation of initiative, authority, and responsibility among the agent, user, and care stakeholders. Rather than dichotomizing autonomy as a one-off consent property, this framework enables proactive support without erosion of user empowerment, allowing configurable initiative, contestability, the exposure of reasoning and uncertainty, strategic scaffolding for patient independence, and proactive interventions with user-aligned safeguards. The agent’s degree of involvement adapts to user capacity, clinical risk, and shifting goals, supporting empowered self-management alongside risk mitigation.
Representative Use Cases
The framework’s utility is demonstrated through clinical and behavioral use cases including chronic symptom management (endometriosis), post-discharge follow-up for heart failure, and ongoing mental health support for anxiety and depression.
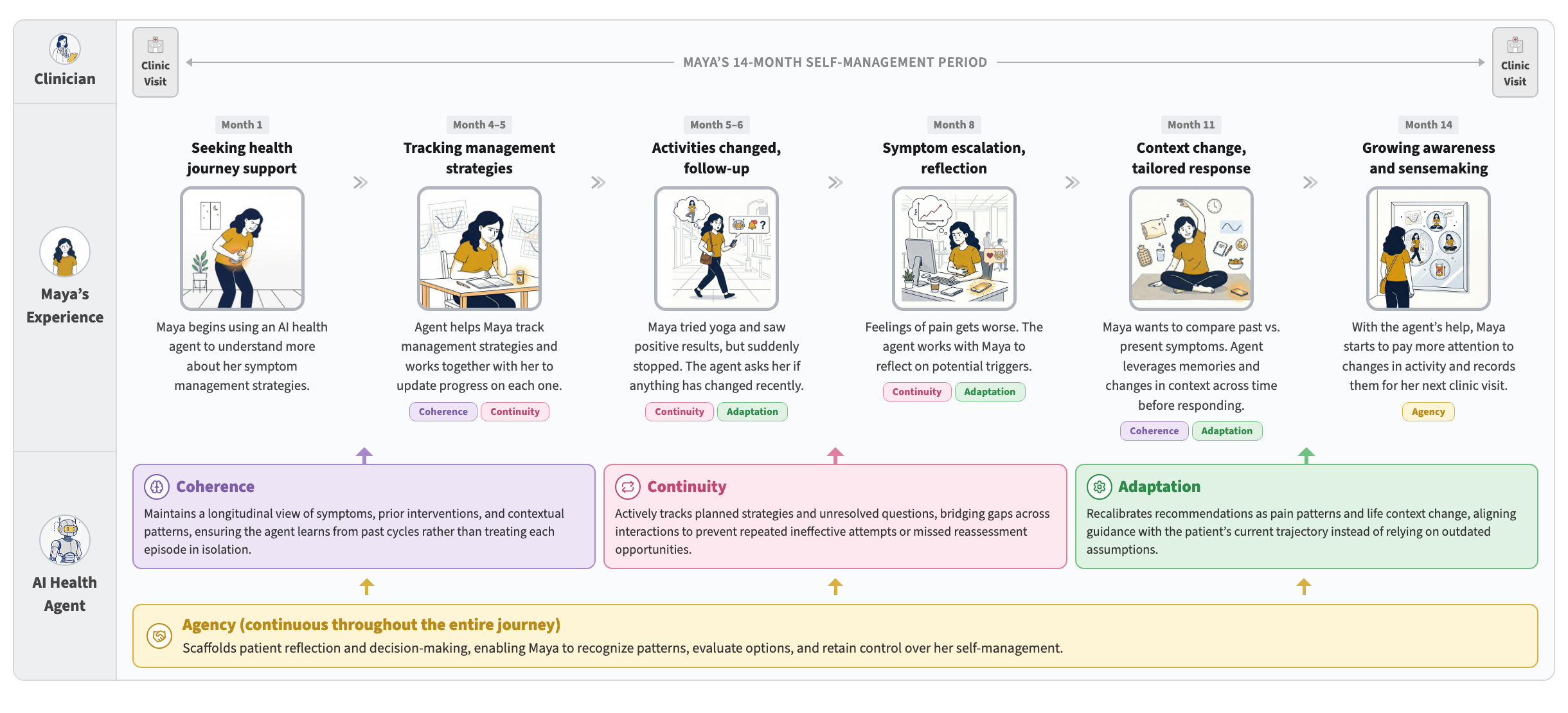
Figure 2: A potential timeline of a longitudinal health agent supporting an individual with endometriosis, integrating coherence, continuity, adaptation, and agency.
Chronic Symptom Management (Endometriosis)
Longitudinal agents can structure and preserve complex hypotheses about symptom dynamics, triggers, and therapeutic trials, tracking unresolved clinical questions and resurfacing them at appropriate intervals. They support the transition from episodic recall to a continuously refined, contextualized personal model, improving the efficiency and safety of self-management, particularly as priorities and context evolve. Strategic calibration of agent proactivity further enables empowerment without overwhelming users during periods of decision fatigue or clinical uncertainty.
Post-Discharge Heart Failure Follow-Up
In acute transitions such as heart failure discharge, agents maintain a live, structured model of the care plan, coordinate between clinical and home settings, and proactively monitor for deviations from recovery milestones. This supports continuity not only in immediate adherence, but also in interpretation of longitudinal trends and feedback to both users and clinical teams. The agent modulates its degree of involvement—including alerting, follow-up, and patient education—according to recovery stage and risk, reducing the likelihood of fragmented or unsafe care.
Ongoing Mental Health Support
For mental health, the agent aggregates and contextualizes longitudinal trends in mood, behavior, and engagement, maintaining presence across sparse or irregular therapeutic encounters. Adaptation enables recalibration of support as emotional states or external context change, while agency-layer mechanisms negotiate autonomy and initiative to avoid both over-direction and abandonment. The result is robust, user-centered mental health stewardship across phases of stability and vulnerability.
Key Implementation Challenges and Open Research Problems
Designing longitudinal health agents entails addressing tensions such as balancing stability (coherence) with necessary model plasticity (adaptation), sustaining long-term engagement (continuity) without reducing autonomy, and orchestrating agent initiative safely (agency). Technical challenges include structured longitudinal representations beyond episodic memory, transparent hypothesis management, explicit encoding of roles and trajectories, and longitudinal calibration of agent control. Integration with EHRs, privacy-preserving mechanisms for consent and data revision, and governance for safety and auditability are also required. Evaluation methods remain an open area; short-term accuracy and adherence are insufficient metrics for measuring longitudinal agent value.
Implications and Future Directions
The framework articulates essential design requirements for the evolution of health AI from reactive, encounter-focused agents to persistent, adaptive, and accountable systems. Practical deployment will require new architectures for multi-agent orchestration, nuanced user modeling, longitudinal metrics for evaluation, and interface designs that support transparency, contestability, and empowerment. Theoretical implications include reframing autonomy, responsibility, and trust as emergent, negotiable concerns that must be explicitly modeled and managed.
As LLM agents mature, sustained coordination across clinical and self-management contexts will necessitate dynamic, evidence-driven realignment of agent roles. Questions regarding oversight, liability, calibration, and user empowerment will necessitate multi-disciplinary collaboration.
Conclusion
This framework provides an authoritative conceptual foundation for longitudinal health agent design, operationalizing coherence, continuity, adaptation, and agency as core layers for persistent, user-centered AI in healthcare. Enabling safe, effective, and adaptive support across the continuum of health trajectories requires not only algorithmic advances but also principled architecture and evaluation incorporating clinical, informatics, and user-centered perspectives. The outlined challenges and open questions form a robust research agenda for the next generation of health agents that move beyond static personalization toward accountable longitudinal stewardship.