- The paper introduces a model-agnostic orchestration framework with algorithmic impermeability that decouples data ingestion from AI inference.
- It employs a deterministic DAG pipeline and a standardized intermediate payload, ensuring modularity, auditability, and seamless integration with EMR systems.
- Empirical validation shows 100% pipeline reliability, failure safety, and effective multi-protocol support, paving the way for scalable oncology decision support.
The Large Cancer Assistant (LCA): Algorithmic Impermeability and Model-Agnostic Clinical Orchestration in Oncology
Context and Limitations of Multimodal Oncology AI
Prevailing architectures for machine learning in oncology are fundamentally constrained by rigid, monolithic integration of data ingestion, routing, and model inference. Such tight coupling precludes post-hoc adaptation, modularity, or robust interoperability with heterogeneous hospital IT infrastructure. Despite recent progress in multimodal deep learning—spanning multimodal fusion of imaging, omics, and clinical text [GD_Net], and foundation vision-LLMs for oncology [MUSK_Stanford]—existing frameworks are not directly extensible to scalable clinical decision support due to their architectural inflexibility and persistent entanglement of data orchestration and AI inference.
The Large Cancer Assistant (LCA) is introduced as a model-agnostic orchestration system that imposes strict architectural decoupling between data pipelines and downstream black-box AI models. This framework champions the principle of algorithmic impermeability, rigorously preventing any cross-dependence between orchestration logic and specific model implementations or downstream EMR protocols.
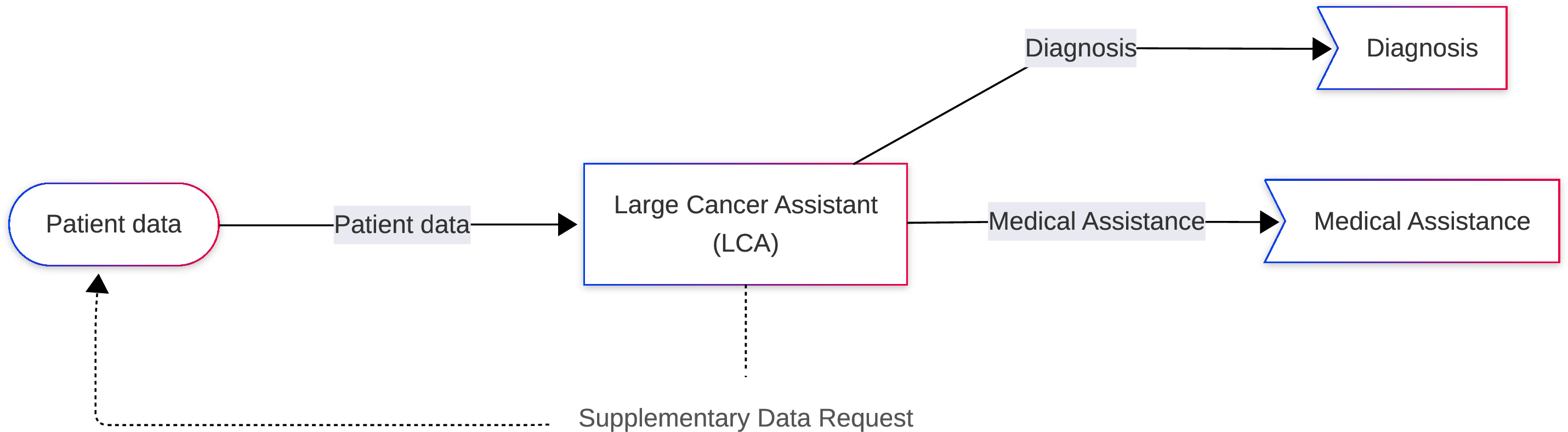
Figure 1: Macroscopic ecosystem of the LCA framework, showing the model-agnostic LCA core with multimodal input and explicit decoupling of all outputs—including a Supplementary Data Request feedback mechanism.
Formal Framework: LCA Architecture and Entry Theory
LCA is mathematically instantiated as a 7-tuple, the critical elements of which are (i) an input space of structured, heterogeneous clinical histories, (ii) a registry of pathology protocols, and (iii) a deterministic, unidirectional orchestration pipeline of modular interpretable units. The formalization revolves around the following modules: Data Preprocessing (DPM), Cancer Switching (CSM), Diagnostic (LCDM), Remedy (LCRM), and a Wordings interface (LCWM). Notably, all orchestration logic, including routing and failure-handling, is declared a priori, independently of learned model parameters.

Figure 2: Internal orchestration graph, showing the DAG pipeline sequence and propagation of a shared routing context P^. Explicit logic separation guarantees that AI model swaps leave orchestration invariant.
The Entry Theory component formally decomposes all input signals along two orthogonal axes: (1) a geometric-structural axis (domain, symmetry group, feature type) compatible with geometric deep learning, and (2) a medical axis encoding provenance, usage, and epistemic certainty. The content and context of each entry are algebraically decoupled, supporting principled, lossless translation across arbitrary clinical data sources.
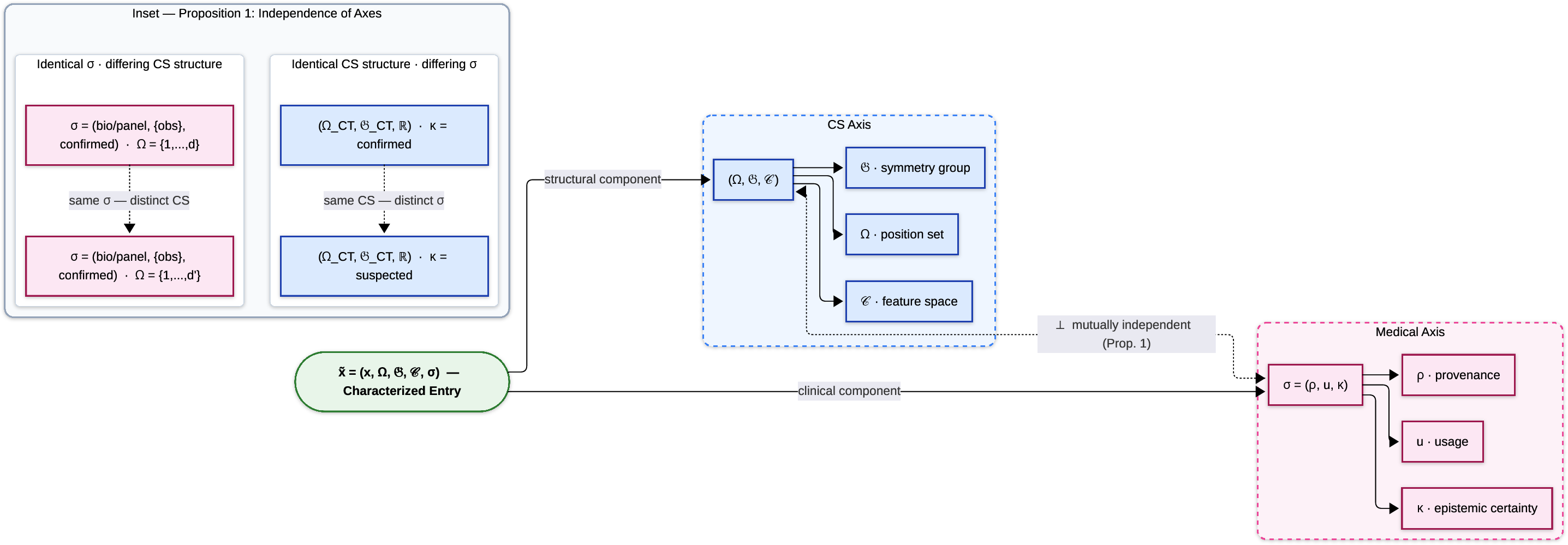
Figure 3: Structure of characterized entries, demonstrating orthogonality of the structural (CS) and medical axes.
Algorithmic Impermeability and Routing Logic
A core contribution is the explicit enforcement of algorithmic impermeability. Formally, all routing projections, module activations, and structural schema decisions are invariant under any model swap (given adherence to the pre-specified interface contract). The practical implication is that clinical AI models can be retrained, updated, or replaced without any need for revalidation upstream of the protocol boundaries—contrasting sharply with all monolithic fusion models. The result is a clinically robust system minimally susceptible to propagation of IT or model changes.
Routing is governed by the Cancer Switching Module, supporting both deterministic (clinician-chosen) and probabilistic (V2, learned and calibrated) protocol identification. The design enables dynamic, cancer-agnostic matching of patient representations to appropriate downstream AI pipelines. Failure at routing or module precondition levels is handled deterministically and always triggers targeted Supplementary Data Requests—never silent or spurious outputs.
Rather than direct EMR commit or fused outputs, LCWM emits a strictly defined Standardized Intermediate Payload (SIP) at the orchestration boundary. The SIP provides both a structured bypass of all input and output artifacts and an NLG narrative summary, completely decoupled from healthcare IT specifics. The SIP logs provenance, input references, protocol activation traces, diagnostics/remedy signatures, all module states, and explicit SDRs, but purposely excludes all model identifiers to sustain algorithmic impermeability.
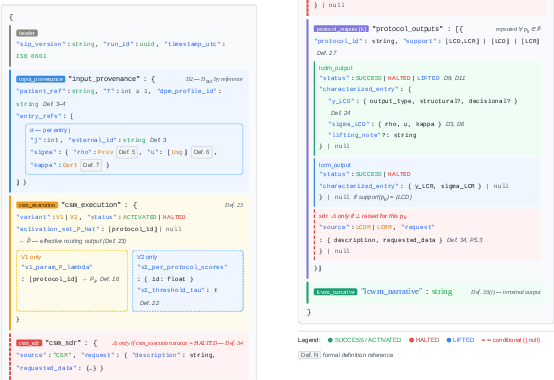
Figure 4: Condensed SIP/SDR schema (annotated pseudo-JSON), showing architectural blocks, protocol outputs, and SDR embedding, jointly ensuring auditability, provenance, and strict decoupling from downstream EMR or FHIR implementations.
This layer provides strong guarantees:
- SIP is the invariant external output for all cases, including failures.
- All input data is referenced but never serialized directly, eliminating latency or redundancy issues.
- Distinct code paths (model failures, routing nulls, or input schema errors) are precisely traceable, supporting full clinical audit and regulatory alignment.
Empirical Validation of Orchestration Guarantees
The proof-of-concept implementation verified the framework under four critical technical scenarios:
- Nominal flow: 100% pipeline completion and SIP schema validity, with orchestration layer latency of ∼0.04 ms (negligible versus typical model inference).
- Algorithmic impermeability: Swapping between distinct stubs with different output schemas yielded invariant routing and SIP structure (100% π-equality), with per-case inference content differences—a direct, strong claim.
- Failure safety: 100% recall in SDR emission for targeted data anomaly injections; construction-time rejection of ill-typed empty histories.
- Multi-protocol support: Parallel activation and full branch independence for multiple protocols, schema validity preserved.

Figure 5: PoC architecture highlighting LCA modules, pipeline independence, synthetic inputs, and reference stubs.
These results, though not asserting clinical model accuracy, explicitly demonstrate the formal properties that underpin LCA's orchestration layer and its divergence from monolithic multimodal approaches.
Practical and Theoretical Implications
The isolation of orchestration logic from model internals and EMR-specific protocols resolves key deployment fragilities for large-scale, multimodal CDSS in oncology. Rapid retraining and deployment of models, unimpeded protocol catalog expansion, and robust human-in-the-loop control at all SDR emission points position LCA as an operational building block for scalable oncology informatics. The SIP boundary enables transparent mapping to FHIR or other standards without upstream regression risk.
The unidirectional DAG structure and dual-variant routing paradigm (V1, V2) further provide an extensible substrate for future development—encompassing autocalibrated triage, adaptive clinical pathway composition, and protocol versioning.
Theoretically, the mutual independence of geometric and semantic axes in Entry Theory and the impermeability formalization together supply a rigorous mathematical substrate for multi-protocol orchestration. This directly supports ongoing requirements for regulatory traceability and static formal verification in clinical AI.
Future Directions
Advancement of LCA's capabilities entails:
- Empirical validation and calibration of the V2 (learned) router across large, multi-pathology cohorts.
- Expansion of SIP translation to strict HL7 FHIR and pipeline abstractions for federated or privacy-preserving infrastructure.
- Incorporation of multimodal feature extraction and protocol decoupling at scale.
Conclusion
The Large Cancer Assistant redefines the system architecture for clinical oncology decision support by enforcing strict, model-agnostic orchestration boundaries. Through algorithmic impermeability, cancer-agnostic pipeline routing, and a rigorous SIP schema, LCA provides a modular, interoperable, and auditable foundation for scalable multimodal CDSS deployment. This approach directly eliminates key obstacles posed by monolithic, tightly integrated AI models, establishing a robust reference for future clinical and engineering translation in AI-driven oncology.
(2607.06531)

