- The paper presents TRIAGE, a framework using dual-chain dialectical reasoning to provide calibrated risk scores and outcome-conditioned clinical explanations from irregular EHR time series.
- It employs a two-stage training pipeline combining supervised fine-tuning and reinforcement learning with group relative policy optimization to enhance calibration and discrimination.
- Empirical results demonstrate that TRIAGE outperforms baselines on metrics like AUROC, AUPRC, and calibration, especially under missing data and low-resource scenarios.
TRIAGE: Dialectical Reasoning for Explainable Risk Prediction on Irregular Medical Time Series with LLMs
Introduction and Motivation
Accurate prediction and effective triage from Electronic Health Records (EHR), structured as irregularly sampled medical time series (ISMTS), necessitate calibrated risk estimation and transparent, clinically meaningful language-based rationales. Mainstream deep learning (DL) solutions for ISMTS deliver state-of-the-art discrimination but lack interpretable reasoning. Attempts to augment deep models with post-hoc explainability offer only attribution-level insights, falling short of clinician-verifiable justification. Recent LLM-based approaches have primarily bifurcated: (1) probability extraction from answer-token distributions (HeLM, EHR-R1), yielding patient-comparable risk with no explanation, and (2) rationale-augmented predictions (KARE, OpenTSLM), yielding opaque or discrete (often non-comparable) risk with ungrounded narrative.
The paper introduces TRIAGE (“Time Series Reasoning by Inspecting Alternative Outcomes for Grounded Risk Estimation”), a unified framework enabling LLMs to generate outcome-conditioned dialectical rationales and well-calibrated, continuous risk scores in a single inference pass. The authors identify a risk polarization pathology in conventional LLM reasoning: when prompted to justify a choice, the model pre-commits to a one-sided narrative, saturating its answer-token probability and destroying cross-patient discrimination. TRIAGE addresses this by structurally separating the rationale into parallel chains, each grounded in evidence for a specific outcome, and reads risk from the logit-level softmax over outcome tokens conditioned on these balanced deliberations.
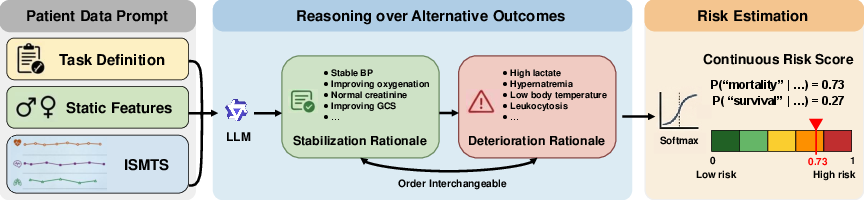
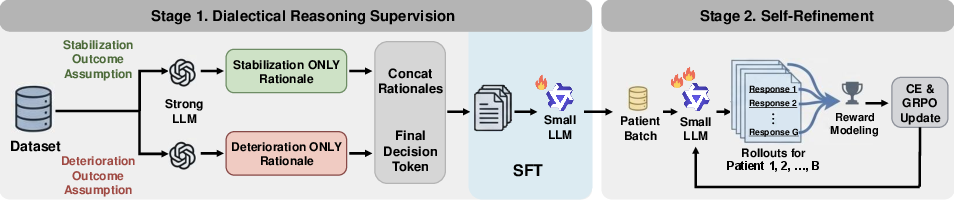
Figure 1: Schematic of TRIAGE: patient information is represented as language; alternative outcomes are explicitly reasoned about in parallel and used to compute calibrated risk.
Method: Dialectical Reasoning and Self-Refinement
Reasoning Procedure:
TRIAGE divides a patient’s ISMTS record into (a) structured language prompts, and (b) dedicated rationale blocks for every candidate outcome (e.g., survival, death). The input prompt includes a programmatic definition, static patient attributes, and serialized observations.
Each outcome (e.g., “survival,” “death”) is allocated an independent rationale—eliciting only evidence consistent with that specific outcome and strictly prohibiting fabricated or contrastive information. This dual-chain format forces the model to enumerate and balance both supporting and refuting clinical observations, removing the confirmation bias that pervades classical reasoning chains.
Risk estimation occurs by capturing the model’s softmax probability over the answer tokens following the two rationales. Since there is no final summary or committed verdict, the resulting probability preserves fine-grained uncertainty and supports cross-patient comparison.
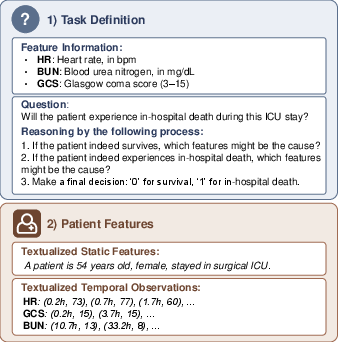
Figure 2: Example of input prompt format—with task definition and structured patient feature blocks—used to facilitate dialectical reasoning.
Training Pipeline:
- Dialectical Reasoning Supervision (SFT): Using a strong LLM (e.g., GPT-5.1 or Kimi K2) to synthesize outcome-conditioned rationales, the framework fine-tunes a more compact LLM (e.g., Qwen3-4B-Base) on these traces, including order augmentation to avoid positional bias.
- Self-Refinement (RL with Group Relative Policy Optimization, GRPO): To correct exposure bias and enhance calibration, the model is further aligned by RL, rewarding discrimination via batch-level, cross-patient separation of log-odds. The loss comprises GRPO on rationales and cross-entropy on the decision token. Batch-level rewards foster patient-comparability in risk and regularize calibration, outperforming sample-level RL objectives.
Empirical Evaluation
Benchmarks and Setups:
Experiments are conducted on three representative, class-imbalanced ISMTS datasets—P12 and MIMIC-III (in-hospital mortality), and P19 (early sepsis). Metrics include AUROC, AUPRC (with AUPRC primary for severe imbalance), Expected Calibration Error (ECE), and Brier score.
Main Results:
TRIAGE, after SFT and RL, achieves the highest or near-highest discrimination and calibration on all datasets. Compared to strong baselines (e.g., GRU-D, KEDGN), TRIAGE reduces calibration error by 81% and provides mean AUPRC improvements of 3.3%. It is also robust under missing variable conditions, outperforming or matching competitors as up to 50% of variables are masked.
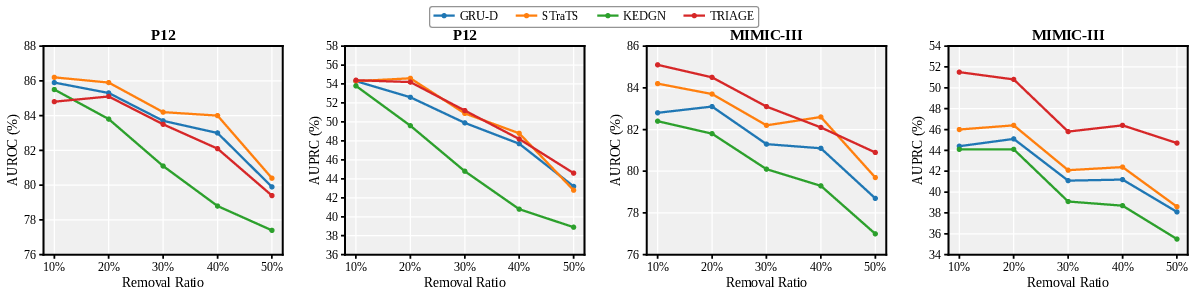
Figure 3: TRIAGE versus ISMTS baselines under leave-variables-out scenario, highlighting superior robustness as variable removal increases.
The ablation study underscores the criticality of dialectical structure: one-sided rationale supervision causes risk collapse, even with prompt sampling, and underperforms answer-only SFT in discrimination. The batch-level reward in RL produces stronger risk calibration and separation compared to classical sample-level rewards.
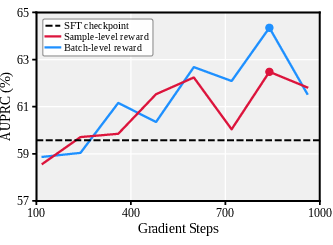
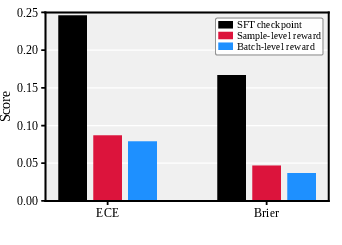
Figure 4: Calibration results for competing models, with lower ECE indicative of better-calibrated probabilistic risk estimates.
Analysis of Explainability and Clinical Reasoning Quality
TRIAGE’s parallel, outcome-conditioned rationales provide directly interpretable, patient-specific justifications. LLM-as-a-judge (IDEA) evaluation shows that TRIAGE explanations are consistently superior (total score +1.27, interpretive summary +0.9) to post-hoc XAI-based explanations from the strongest baselines.
In qualitative analysis, baseline model attributions frequently hallucinate, conflate, or misinterpret prognostically salient features (e.g., treating GCS=15 as death evidence, misattributing improvement signals). In contrast, TRIAGE’s rationales are temporally aware, feature-precise, and consistent with established clinical knowledge, with minimal hallucination rates (<2%).
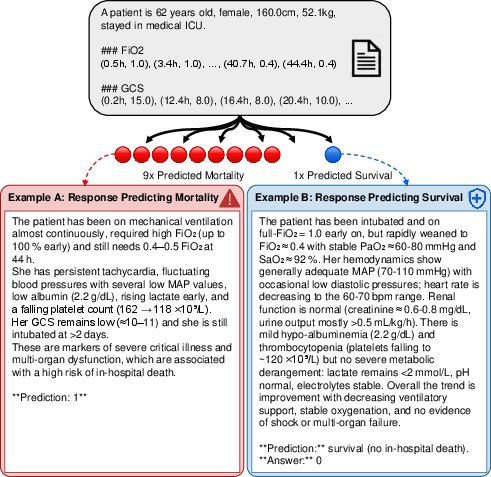
Figure 5: Sample reasoning traces from a conventional LLM—both show one-sided confirmation bias and collapse the risk score to the committed outcome.
Low-Resource Regimes and Backbone Robustness
By leveraging knowledge encoded in foundation models, TRIAGE delivers pronounced advantages under low-resource (1–10% supervision) training, outperforming GRU-D by up to 11% AUPRC with minimal labeled data. Performance gains persist across multiple open LLM architectures (Qwen3-1.7B, 4B, 8B; Llama3.2-3B), confirming method generality.
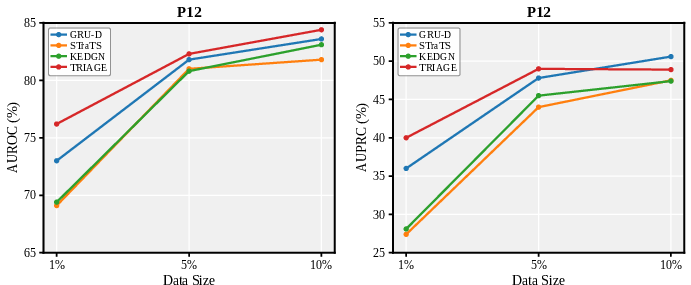
Figure 6: Performance under low-resource training—TRIAGE maintains larger improvement margins at 1% and 5% labeled data.
Broader Implications and Future Directions
TRIAGE demonstrates that structural prompt engineering and outcome-conditioned reasoning significantly mitigate pathologies inherent in standard LLM-based clinical predictions—specifically, overconfident, non-comparable risk estimates and non-grounded explanations. The dialectical format enforces a balanced, multi-hypothesis reasoning protocol, resulting in (1) improved continuous risk calibration; (2) more clinically transparent and actionable explanations; (3) robustness against missingness; and (4) enhanced sample efficiency.
The primary constraints are computational overhead and the restriction to binary settings; future research may extend the framework to multi-class/multi-label tasks, incorporate expert-in-the-loop rationale evaluation, and optimize for low-latency deployment.
Conclusion
TRIAGE sets a new paradigm for LLM-based ISMTS risk prediction, in which LLMs deliver both well-calibrated, patient-comparable risk scores and dialectically structured, clinically meaningful explanations. The method’s dual-stage alignment protocol and balanced rationale generation enable it to systematically outperform specialist deep learning models and generic LLM baselines, advancing the practical deployment of trustworthy, explainable AI for real-world clinical decision support.

