- The paper introduces a multidimensional coding framework to evaluate how clinical AI systems handle longitudinal patient data within EHRs.
- The study finds that only 20% of systems maintain persistent patient-state representations, impacting the fidelity of clinical reasoning.
- The research advocates for new benchmarks prioritizing interpretability and trajectory reconstruction to bridge the gap between prediction and clinical reasoning.
Structured Analysis of Longitudinal Reasoning in EHR-Integrated Clinical AI
Introduction
This paper systematically investigates the representation and operationalization of longitudinal patient data within electronic health record (EHR)-integrated clinical AI systems. By developing a comprehensive coding framework and applying it to a curated corpus of 85 publications, the work reveals how contemporary systems process, compress, and structure EHR-derived information with respect to the temporal dynamics of clinical reasoning. It explicitly addresses the disconnect between routine data ingestion and the explicit encoding of evolving patient trajectories central to medical practice.
Methodological Framework
The analysis introduces a multi-dimensional coding framework capturing both the technical and representational axes of EHR-based systems, including (but not limited to): patient representation level, longitudinal fidelity, temporal modeling, cross-encounter reasoning, and information compression. Systems were classified according to whether they supported persistent representations of patient state across encounters, the granularity of their data abstractions, and their fidelity in maintaining original patient trajectories.
Physician perspectives were collected—via structured reflections from practitioners using major EHR platforms—to triangulate technical findings with real-world challenges in information access, trajectory reconstruction, and clinical workflow.
Patterns of Patient Representation
A dominant finding is the stratification of representation strategies in clinical AI. The majority of systems reviewed are population-level or encounter-oriented, with 58.8% annotated as population-level and only 20% maintaining a longitudinal patient state representation. This underlying representational choice directly impacts the preservation of trajectory information essential for longitudinal reasoning.
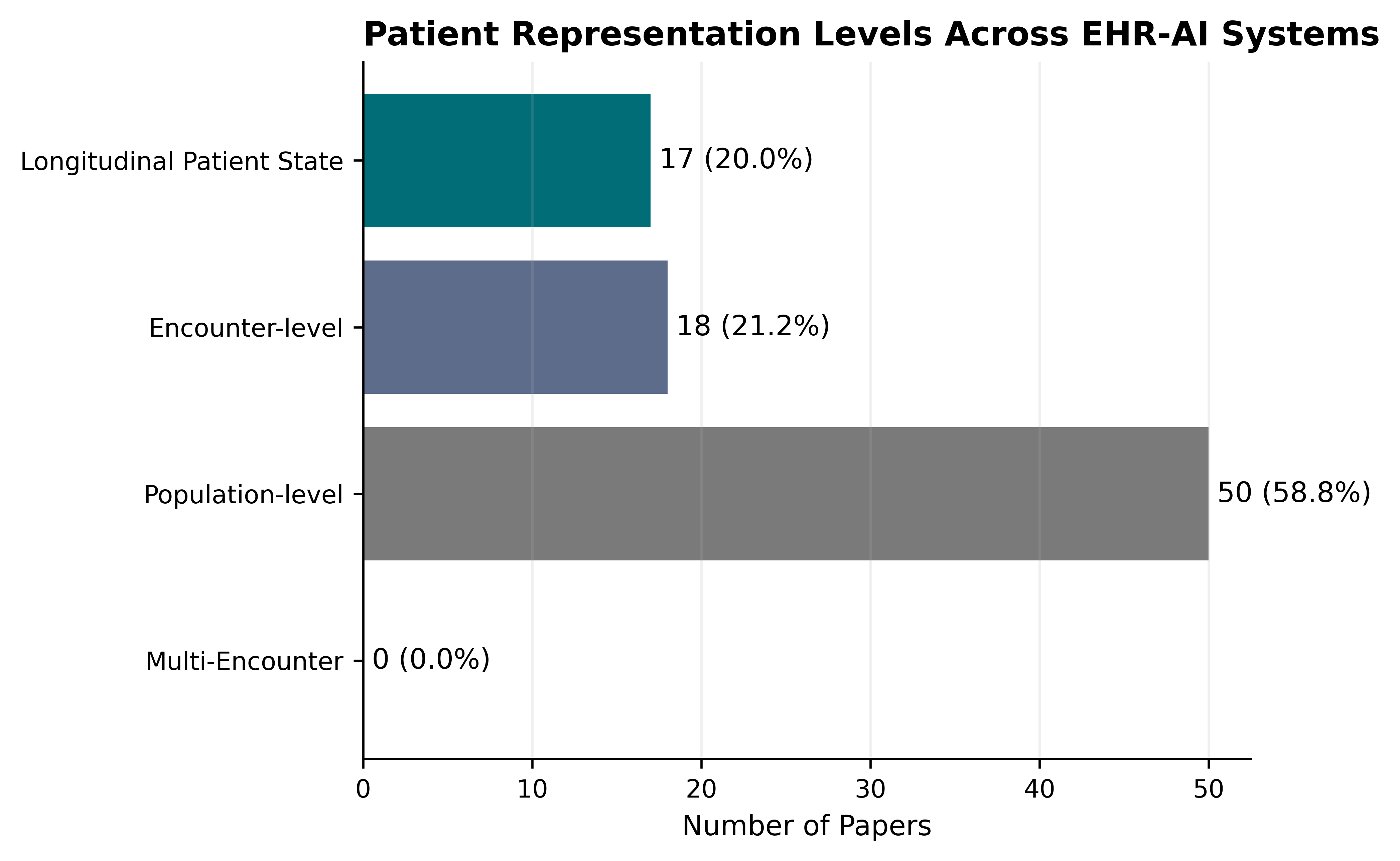
Figure 1: Distribution of system architectures by patient representation level (encounter-level, multi-encounter, longitudinal, or population-level).
The coding framework reveals that persistent patient-state architectures—those explicitly tracking evolving patient status across encounters—remain the minority. Most systems compress complex longitudinal narratives into static summary features, latent embeddings, or even further into recommendations and alerts, decoupling their outputs from the raw, temporally stratified clinical history.
The results highlight a pervasive trend toward aggressive information compression. More than half the corpus utilized feature aggregation, while latent embeddings and recommendation generators accounted for another substantial fraction. Only 12.9% of systems exhibited high longitudinal fidelity, and a single system was identified as maintaining very high fidelity to longitudinal data structures.
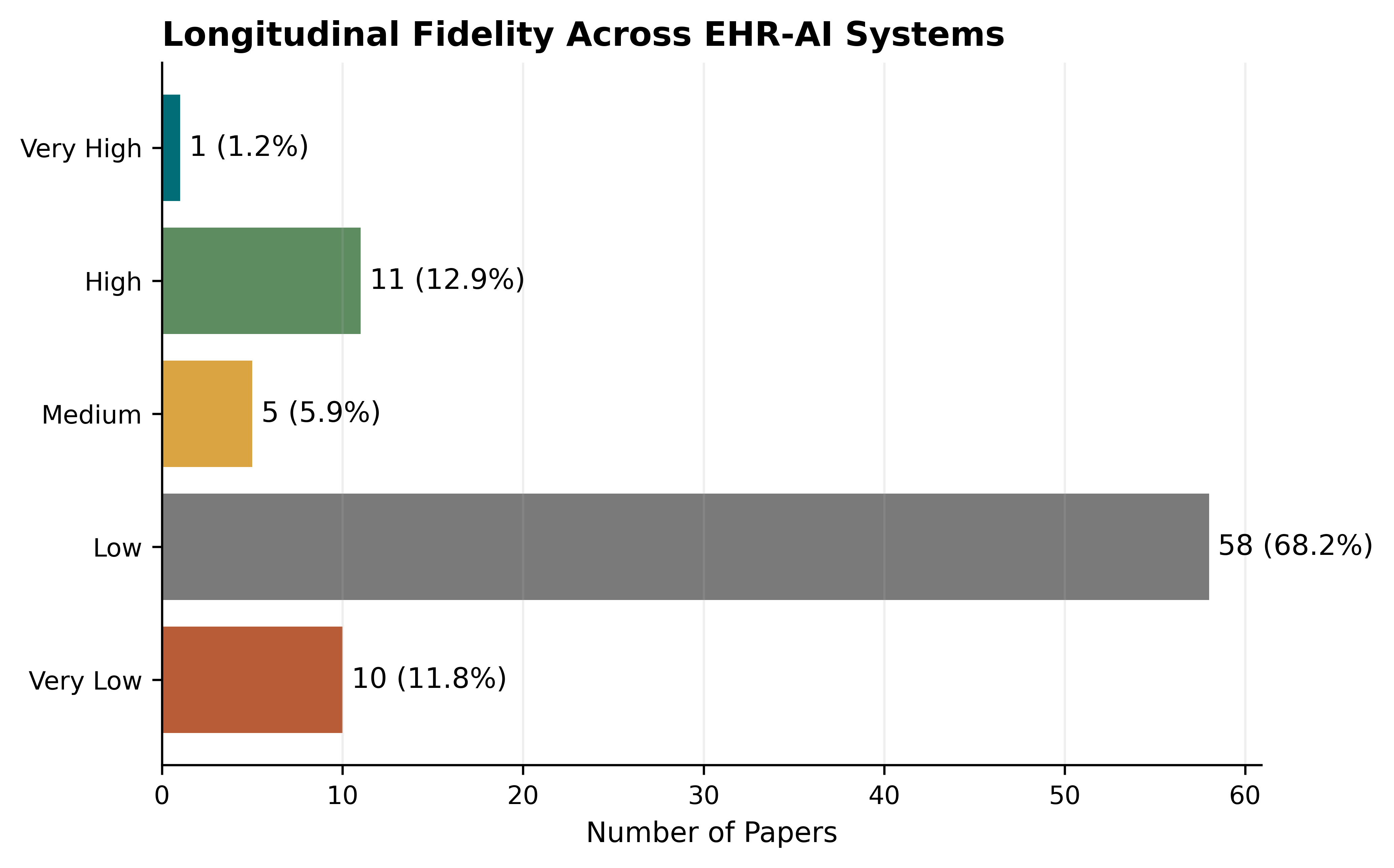
Figure 2: Levels of longitudinal fidelity across the corpus, indicating the degree to which original patient trajectories are preserved versus compressed during modeling.
This pervasive compression is tightly linked to representational architecture. Systems that maintain explicit longitudinal patient-state representations are significantly more likely to retain trajectory fidelity, whereas encounter- and population-level architectures consistently result in low or very low fidelity.
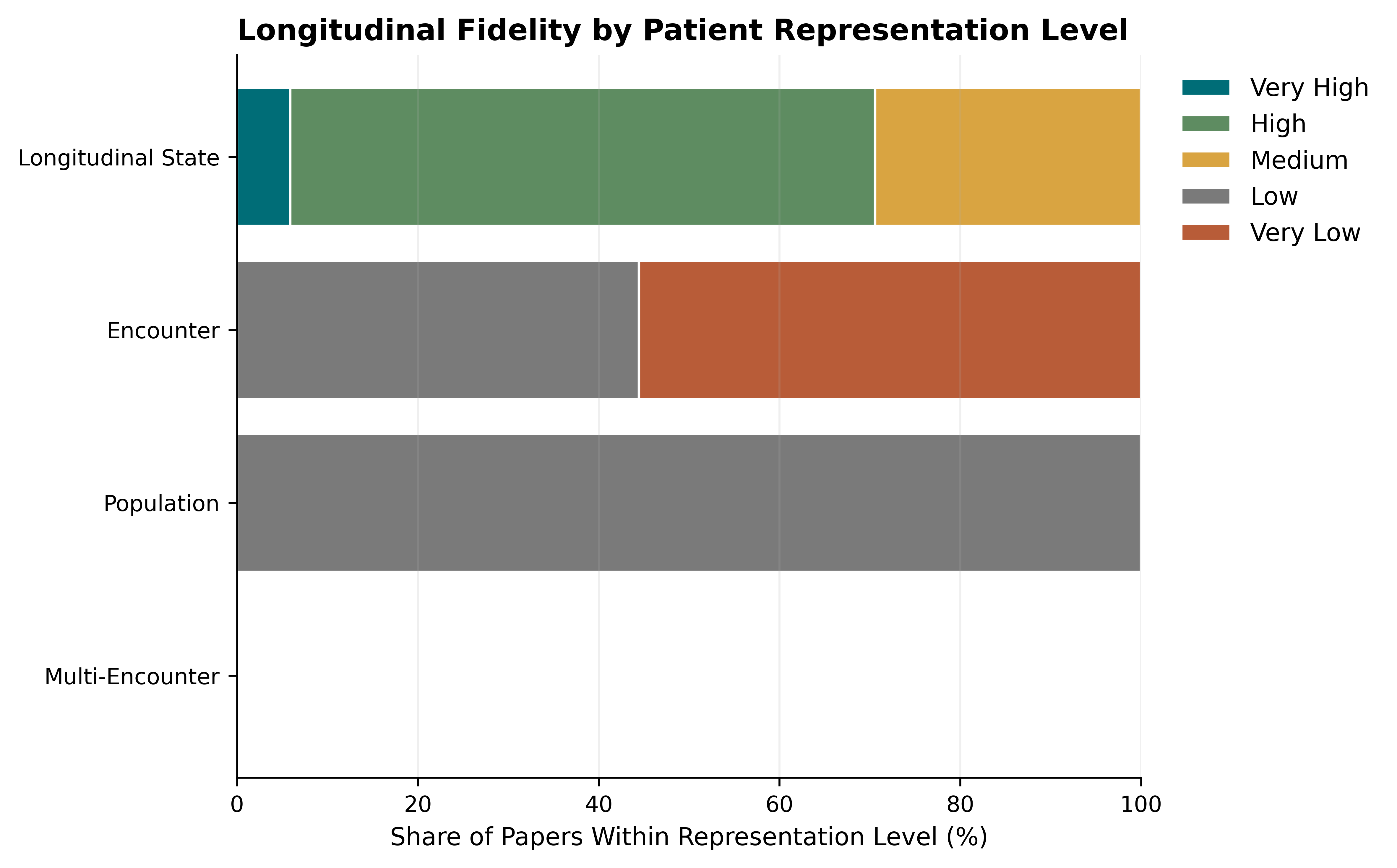
Figure 3: Cross-tabulation of patient representation level with longitudinal fidelity, illustrating the superiority of longitudinal patient-state models.
Thus, even as EHR data retains longitudinal structure, it is predominantly utilized in ways that decouple the AI's reasoning substrate from the very temporality it is supposed to model. This design choice curtails the capacity for systems to support clinical reasoning tasks such as trajectory tracking, absence-based inference, and interpretation of diagnostic evolution.
Alignment with Clinical Needs: Physician Reflections
Physician accounts reinforce the technical conclusions. Despite advances in EHR design and usability, clinical narratives recounted substantial friction in reconstructing longitudinal patient context. Recurring themes included:
- Difficulty synthesizing information scattered across documentation, results, and encounters
- Absence of explicit support for identifying evolution in diagnoses or reasoning chains
- Tension between compliance-driven documentation structures and clinically salient storytelling
- High cognitive and time costs associated with “manual” longitudinal synthesis
Existing EHRs and the bulk of contemporary AI support tools are described as repositories or “passive” systems that require clinicians to reconstruct evolving contexts, rather than agents that externalize, summarize, and make explicit the patient state trajectory.
Practical and Theoretical Implications
The findings suggest that the prevailing focus on predictive accuracy in EHR-based AI is insufficient for clinical adoption paradigms prioritizing interpretability, trajectory reconstruction, and reasoning support. The disjunction between data access and reasoning-aligned representation is not just a technical issue—it is a primary determinant of the system's fit for use in real-world longitudinal clinical workflows.
Key implications include:
- Systems optimized strictly for prediction (e.g., outcome forecasting, disease onset risk) usually compress away reversible “evidence paths” and the narrative context clinicians need for interpretability and actionability.
- Representational fidelity—explicit modeling of evolving patient state—should be prioritized in both system design and evaluation, particularly for high-impact domains such as longitudinal management, complex differential diagnosis, and cross-specialty handoffs.
- There is an urgent need for new benchmarks in clinical AI that go beyond predictive metrics and focus on trajectory reconstruction, temporal evidence traceability, and the ability of AI outputs to externalize reasoning chains.
Directions for Future Development
A shift toward architectures maintaining explicit, modifiable, and inspectable patient-state representations is required. This includes models capable of:
- Encoding not only observed events but also reasoning over absences, trends, changing hypotheses, and uncertainty
- Supporting clinical tasks that inherently require temporal continuity (e.g., therapy response monitoring, cross-encounter synthesis)
- Maintaining explicit links between compressed AI outputs and the full informational substrate from which they are derived
Evaluation strategies must shift toward clinician-centered and trajectory-aware metrics, moving beyond outcome-centric or static benchmarks.
Conclusion
The study substantiates that the technical state-of-the-art in EHR-integrated clinical AI predominantly prioritizes prediction tasks at the expense of reasoning-relevant longitudinal representation. Access to EHR data is routinely conflated with the preservation of temporality and interpretive context. Clinically meaningful trajectory modeling—supported by persistent, high-fidelity patient-state representations—is comparatively rare. Both technical and end-user evidence support prioritizing representational fidelity and temporal reasoning capacities as cardinal objectives for the next generation of EHR-integrated AI, with direct implications for clinical interpretability, workflow integration, and the ultimate efficacy of AI-enabled care delivery.