TopoOR: A Unified Topological Scene Representation for the Operating Room
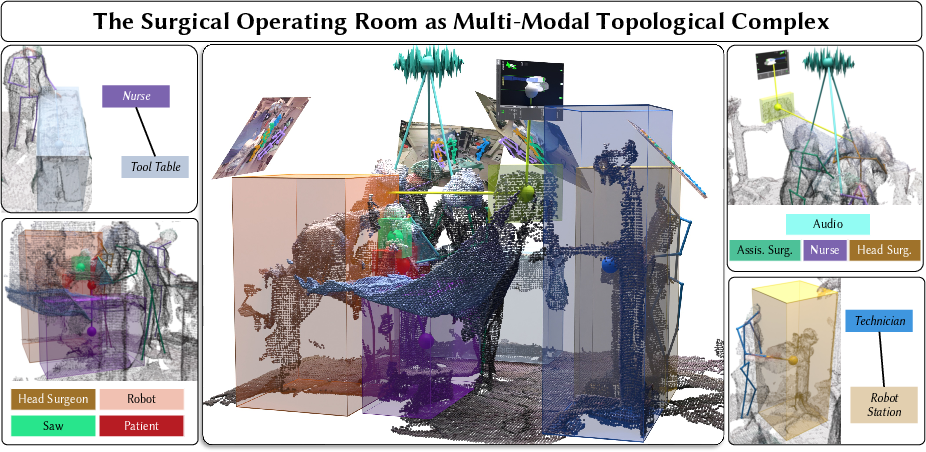
Abstract: Surgical Scene Graphs abstract the complexity of surgical operating rooms (OR) into a structure of entities and their relations, but existing paradigms suffer from strictly dyadic structural limitations. Frameworks that predominantly rely on pairwise message passing or tokenized sequences flatten the manifold geometry inherent to relational structures and lose structure in the process. We introduce TopoOR, a new paradigm that models multimodal operating rooms as a higher-order structure, innately preserving pairwise and group relationships. By lifting interactions between entities into higher-order topological cells, TopoOR natively models complex dynamics and multimodality present in the OR. This topological representation subsumes traditional scene graphs, thereby offering strictly greater expressivity. We also propose a higher-order attention mechanism that explicitly preserves manifold structure and modality-specific features throughout hierarchical relational attention. In this way, we circumvent combining 3D geometry, audio, and robot kinematics into a single joint latent representation, preserving the precise multimodal structure required for safety-critical reasoning, unlike existing methods. Extensive experiments demonstrate that our approach outperforms traditional graph and LLM-based baselines across sterility breach detection, robot phase prediction, and next-action anticipation
Paper Prompts
Sign up for free to create and run prompts on this paper using GPT-5.
Top Community Prompts
Explain it Like I'm 14
What is this paper about?
This paper is about teaching computers to better understand what’s happening inside a surgical operating room (OR). The authors introduce a new way, called TopoOR, to represent all the people, tools, machines, sounds, and movements in the OR—not just as pairs of things that interact, but as groups that work together at the same time. This helps the computer make safer and smarter predictions during surgery.
What questions are the researchers asking?
- Can we model real surgical teamwork (where many things happen together) instead of breaking it into simple pairs like “doctor uses tool”?
- Can keeping different types of information separate but connected (3D positions, video, sound, robot logs) lead to better predictions?
- Does this new representation help with important tasks such as spotting sterility problems, predicting what will happen next, and recognizing what phase a surgical robot is in?
How did they do it? (Easy-to-understand methods)
Think of the OR like a team sport:
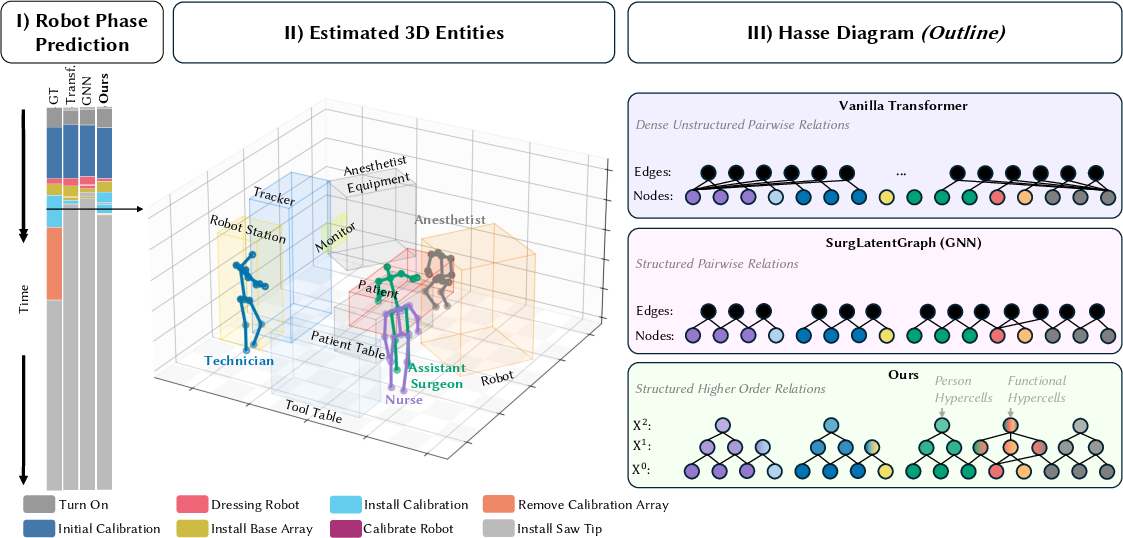
- Old way (scene graphs): Imagine describing a soccer play only as a list of pairwise passes (“A passes to B,” “B passes to C”). You miss the bigger picture, like how the whole team moves together.
- New way (TopoOR): Capture both the individual moves and the group play (e.g., “these four players coordinate to execute a play”). That’s what TopoOR does for surgery.
Here’s how TopoOR builds this “team play” model:
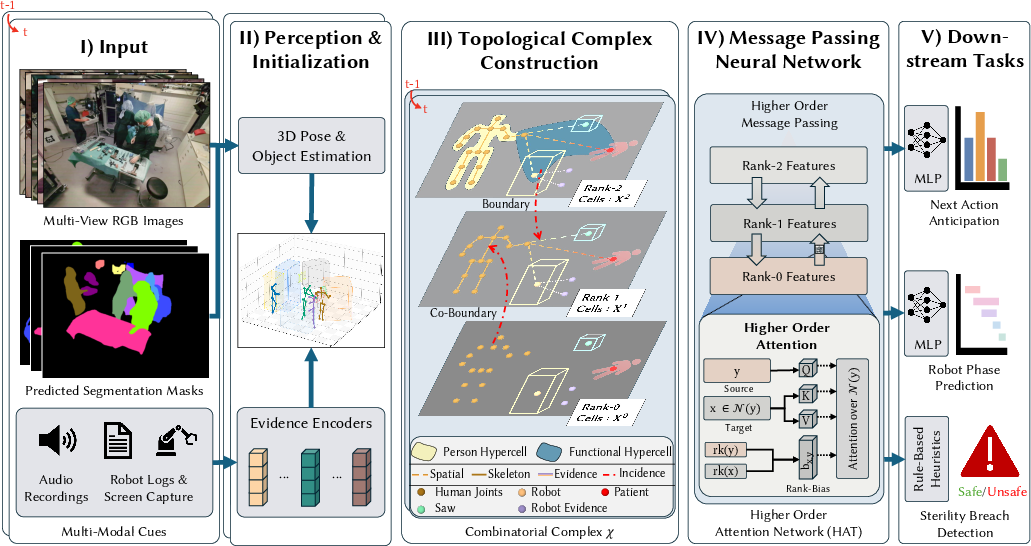
- Three levels of building blocks (like LEGO layers):
- Rank-0 (points): People’s joints, tools, patient, robot parts—each as 3D points or small objects.
- Rank-1 (links): Connections between points—like bones in a person’s skeleton, or a tool close to a patient.
- Rank-2 (groups): Small “team huddles” that bundle several people or tools acting together (e.g., Surgeon + Robot + Saw + Patient during a specific step).
- Multiple senses, kept separate but connected:
- Vision (RGB images), 3D positions (where things are), robot logs (text-like information), and audio (sounds).
- Instead of squeezing all of this into one blended feature, TopoOR keeps each type in its own form and connects them structurally. That way, the model doesn’t lose important details.
- A smarter “attention” mechanism (Higher-Order Attention Network, HAT):
- Attention is a way for the model to focus on what matters most. HAT passes information up and down the layers:
- Upward: from individuals (rank-0) to interactions or groups (rank-1, rank-2).
- Downward: from group context back to individuals.
- It also treats different layers differently, so the model knows whether it’s looking at a person’s arm or a whole team action.
- Time matters:
- The model connects the same person or object across consecutive moments, so it understands how things change over time (like a mini video clip rather than a single photo).
- Tasks the model learns:
- Next Action Anticipation: What is likely to happen next?
- Robot Phase Prediction: Which step the surgical robot is currently performing.
- Sterility Breach Detection: Spotting when a non-sterile person or object gets too close to a sterile area. (This one is handled with simple 3D distance rules using the model’s structure.)
What did they find?
- Better predictions than older methods:
- Next Action Anticipation: TopoOR scored about 41% (F1), higher than baselines that scored around 35–37%.
- Robot Phase Prediction: TopoOR reached about 73% (F1), clearly better than baselines around 64–65%.
- Sterility Breach Detection: All 3D-aware methods (including TopoOR) achieved about 76% (F1), much better than a text-only method (~55%). Here, the strong 3D structure helps everyone, and TopoOR matches the best.
- Mixing more senses helps:
- Starting with just 3D shapes was weak.
- Adding images made a big jump in accuracy.
- Adding robot logs and audio improved things further.
- Connecting moments over time gave another boost, especially for recognizing robot phases.
- Can still talk “old language”:
- Even when TopoOR is forced to output a traditional, simpler scene-graph format, it does a better job than a vision-LLM designed for that task. This means TopoOR’s richer structure captures more useful information.
- Fast and light enough for real-time:
- TopoOR is much smaller (about 12 million parameters) and faster (around 59 ms per step) than a very LLM baseline (~7 billion parameters; ~194 ms per step). That’s important for real surgeries, where delays are risky.
Why does this matter?
Surgery is complex and fast-moving. Many people and machines work together at once. By modeling group interactions directly—and by respecting the unique nature of different data types (3D movement, sound, text, images)—TopoOR gives computers a clearer, safer understanding of what’s going on. This could help:
- Reduce mistakes (like sterility breaches).
- Support surgeons by predicting what they’ll need next.
- Track surgical robot progress in real time.
- Make computer assistance more dependable and faster during actual operations.
Key takeaways
- Real surgeries often involve groups acting together, not just pairs—TopoOR models that directly.
- It keeps different types of data in their natural forms and connects them structurally instead of blending them into one.
- It outperforms standard graph and language-model approaches on important tasks.
- It runs fast enough to be useful during real procedures.
Knowledge Gaps
Knowledge gaps, limitations, and open questions
Below is a concise, actionable list of what remains missing, uncertain, or unexplored in the paper and its evaluation.
- External validity: Evaluate TopoOR across institutions, specialties (open, laparoscopic, robotic), OR layouts, and camera rigs to quantify cross-domain generalization.
- Dataset dependence: Assess performance and domain shift on datasets beyond MM-OR, including different robot platforms and non-robotic settings.
- Perception error sensitivity: Quantify how inaccuracies in depth back-projection, 3D pose, segmentation, audio localization, and robot-log parsing propagate through the combinatorial complex and affect downstream tasks.
- Uncertainty handling: Introduce and evaluate uncertainty-aware features (e.g., probabilistic 3D boxes, pose covariances) and calibrated prediction confidence for safety-critical decisions.
- Learned topology vs hand-crafted priors: Replace fixed spatial thresholds and clinical priors with learned or probabilistic structure discovery for rank-1/2 cells; compare end-to-end structure learning with the current rule-based incidence construction.
- Topology stability over time: Define criteria/hysteresis for creating/dissolving rank-2 cells to prevent flicker; evaluate effects on temporal consistency and task performance.
- Temporal horizon and online operation: Study sensitivity to temporal window size, streaming/online inference vs offline batches, and mechanisms for long-range dependencies.
- Robustness to modality dropouts: Systematically test graceful degradation when one or more modalities are missing, delayed, or corrupted; design failover strategies.
- Synchronization and calibration: Quantify tolerance to inter-sensor time skew and extrinsic/intrinsic calibration errors; explore self-calibration or alignment modules.
- Scalability analysis: Characterize computational/memory scaling with entity count and higher-order cells; develop pruning, sparsification, or budgeted attention to handle crowded ORs.
- Edge deployment: Validate latency and throughput on OR-viable edge hardware (embedded GPUs/CPUs), including worst-case latencies under multi-camera loads and energy/thermal constraints.
- Breadth of baselines: Compare against state-of-the-art higher-order methods (e.g., Hypergraph Transformers, simplicial/cell/sheaf neural networks) to isolate the benefits of HAT on combinatorial complexes.
- HAT design ablations: Analyze the impact of rank-pair bias, message directions (boundary vs co-boundary), number of ranks, head count, and per-rank feature spaces on performance.
- Manifold-awareness: Investigate SE(3)/SO(3)-equivariant operators and manifold-aware attention to better exploit articulated kinematics and rotations within ranks.
- Sterility breach modeling: Move beyond rule-based proximity thresholds to learned, probabilistic sterility zones; validate against diverse clinical protocols and measure intraoperative false-alarm rates.
- Interpretability: Develop tools to attribute decisions to specific cells/interactions and visualize higher-order attention for clinician-in-the-loop validation and trust.
- Safety and OOD detection: Incorporate out-of-distribution detection, failure mode monitoring, and formal/empirical safety bounds for alerts in real-time settings.
- Multi-task interference: Analyze task trade-offs (next-action vs phase) and try dynamic task weighting or decoupled heads to mitigate negative transfer.
- Label granularity and taxonomy: Evaluate sensitivity to changes in action/phase label granularity and how it aligns with rank-2 cell definitions.
- Error analysis: Provide systematic breakdowns of failure cases (occlusions, crowded scenes, fast motions, modality noise) to guide targeted improvements.
- Data efficiency: Measure performance under reduced supervision; explore semi/self-supervised pretraining, weak labels, and active learning to reduce dependence on dataset-provided segmentations.
- Bias and fairness: Audit performance across surgeon demographics, body types, institutions, and acoustic conditions to detect modality- or population-specific biases.
- Causal reasoning: Extend from descriptive higher-order relations to causal models enabling counterfactuals or interventional predictions relevant to safety.
- Task coverage and clinical endpoints: Expand beyond classification to localization of interactions, contact reasoning, trajectory forecasting, and define/measure clinically actionable endpoints (risk mitigation, cognitive load, error prevention).
- Automatic higher-order event discovery: Investigate unsupervised or weakly supervised discovery of polyadic events (rank-2+ cells) without relying on curated clinical priors.
- Modality weighting and fusion: Study adaptive, data-driven weighting of modalities to prevent noisy channels from dominating attention; report modality attribution during failures.
- Reproducibility: Release full code, preprocessing, and topology construction recipes; publish standardized benchmarks and protocols for higher-order OR modeling.
- Privacy and ethics: Address consent, audio/video privacy, and on-device anonymization requirements for real-world OR deployment.
- From representation to action: Explore how TopoOR outputs translate to actionable guidance, UI design for alerts, and integration into closed-loop assistance or robotic control.
Practical Applications
Below is an overview of practical, real-world applications grounded in the paper’s core contributions: a higher-order topological representation of operating rooms (TopoOR) and a Higher-Order Attention Network (HAT) that preserves multimodal/manifold structure for safety-critical reasoning. Applications are grouped by deployment horizon and include sector mapping, potential tools/workflows, and feasibility notes.
Immediate Applications
- OR sterility breach monitoring and alerts (Healthcare; Infection Control)
- Use: Real-time detection of non-sterile entities encroaching on sterile zones using 3D geometry and rule-based thresholds (paper demonstrates zero-shot sterility breach detection).
- Tools/Workflows: “SterileWatch” alert service integrated with OR wall monitors; automatic incident timestamps for audit.
- Assumptions/Dependencies: Multi-camera 3D grounding/calibration; robust pose/segmentation; staff role labels; institutional acceptance to manage false positives.
- Phase-aware supervision dashboards for robotic surgery (Healthcare; Surgical Robotics)
- Use: Live display of detected robot phase (73% F1 in paper) and mismatch alerts between intended and observed phases; safety interlocks (soft stops) before critical transitions.
- Tools/Workflows: “PhaseMonitor” console plugin; ROS middleware adapter for robot logs; alerting policies aligned to clinical workflow.
- Assumptions/Dependencies: Real-time access to robot logs; calibrated cameras; mapping between predicted phases and robot state machine; clinical buy-in.
- Next-action anticipation to streamline teamwork (Healthcare; Perioperative Nursing)
- Use: Predict likely next step to pre-stage instruments/consumables and coordinate team motion, potentially reducing idle time.
- Tools/Workflows: “ActionCue” panel for circulating scrub nurse; automated instrument cart preparation prompts.
- Assumptions/Dependencies: Instrument inventory integration; display ergonomics; handling uncertainty (confidence thresholds).
- Context-aware OR overlays on monitors/AR (Healthcare; Software/Devices)
- Use: Visualize sterile field boundaries, warn on imminent breaches, and depict multi-actor functional cells (e.g., {Surgeon, Robot, Saw, Patient}) for shared situational awareness.
- Tools/Workflows: AR head-mounted display or boom display overlay using TopoOR cells and HAT embeddings.
- Assumptions/Dependencies: Low-latency rendering (<100 ms); stable tracking; clinician usability; infection control for AR hardware.
- Automatic incident logging and compliance reports (Healthcare Administration; Quality & Safety)
- Use: Auto-generate reports for sterility breaches, phase durations, and near-miss events; export to string-based scene graphs for audit.
- Tools/Workflows: “Compliance Auditor” with Scene-to-Graph exporter; searchable logs by event type/time.
- Assumptions/Dependencies: Policy mappings to institutional KPIs; data retention/privacy; time synchronization across devices.
- Rapid annotation and dataset curation (Academia; Industry R&D)
- Use: Semi-automatic labeling of surgical phases and relations by reducing TopoOR to conventional scene graph formats (paper shows improved relation F1 vs. VLM baseline).
- Tools/Workflows: “TopoOR Label Assist” that pre-fills triplets/hyper-relations for human verification.
- Assumptions/Dependencies: Access to multimodal data; annotator UI; calibration metadata.
- OR video search and retrieval by higher-order events (Healthcare Education; Software)
- Use: Query training repositories for episodes where specific multi-actor interactions occur (e.g., collaborative bone resection triads/quads).
- Tools/Workflows: Topological event indexer; natural-language-to-topology query bridge.
- Assumptions/Dependencies: Computed TopoOR indices; metadata storage; permissioned access.
- Team coordination feedback in simulation/debriefing (Medical Education)
- Use: Post-hoc analytics of polyadic coordination (rank-2 cells) to highlight bottlenecks, overlaps, and safety boundary violations.
- Tools/Workflows: “Debrief Coach” with timeline of group-state transitions; comparative heatmaps across sessions.
- Assumptions/Dependencies: Simulation data capture; agreed metrics for team dynamics; facilitator training.
- Device and resource utilization analytics (Hospital Operations)
- Use: Aggregate duration and sequence of tool/robot interactions to optimize room turnover and resource planning.
- Tools/Workflows: Utilization dashboards derived from TopoOR functional cells.
- Assumptions/Dependencies: Sufficient coverage of devices by sensors; linkage to scheduling systems.
- Lightweight on-prem deployment for real-time OR perception (Hospital IT; Software)
- Use: Edge deployment with low parameter count (≈12M) and low latency (~59 ms per pass on A40), enabling private, on-site inference.
- Tools/Workflows: Containerized inference service; DICOM/EHR connectors for timestamp alignment.
- Assumptions/Dependencies: GPU-capable edge hardware; secured network; IT governance.
Long-Term Applications
- Closed-loop shared control and autonomy gating (Surgical Robotics)
- Use: Use higher-order scene state to modulate robot autonomy levels, enforce no-go zones, and gate risky maneuvers during critical phases.
- Tools/Workflows: “Phase-Aware Robot Controller” with HAT-derived safety envelopes; ROS2 safety layer.
- Assumptions/Dependencies: Regulatory clearance; formal verification; redundancy/failsafes; broader multi-site validation.
- Proactive risk mitigation and error prevention (Healthcare; Patient Safety)
- Use: Predict unsafe futures (e.g., likely sterile breach or instrument misplacement) and intervene with graded alerts or task re-sequencing.
- Tools/Workflows: “RiskRadar” that fuses next-action anticipation with sterile topology and temporal context.
- Assumptions/Dependencies: Clinically-tuned thresholds; human-factors studies to minimize alarm fatigue; explainability.
- OR digital twin for scheduling and throughput optimization (Operations Research; Hospital Management)
- Use: Simulate team-level polyadic dynamics to optimize case scheduling, staff allocation, and turnover time.
- Tools/Workflows: “OR Digital Twin SDK” seeded by TopoOR/HAT embeddings; what-if simulations.
- Assumptions/Dependencies: Integration with OR management and staffing data; cross-case generalization; change management.
- Automatic intraoperative documentation and coding (Health IT; Revenue Cycle)
- Use: Auto-generate structured logs (phases, events, durations) mapped to CPT/ICD codes and EHR timelines.
- Tools/Workflows: “AutoDoc” that converts TopoOR states to standardized documentation entries.
- Assumptions/Dependencies: Mapping to coding standards; auditing pipelines; privacy and medico-legal governance.
- Standards for multimodal OR data and topological representations (Policy; Standards Bodies)
- Use: Develop open schemas for combinatorial-complex OR models and minimal sensor baselines for safety applications.
- Tools/Workflows: Reference specification (rank definitions, incidence rules, clinical priors), conformance tests.
- Assumptions/Dependencies: Multi-stakeholder consensus (clinicians, vendors, regulators); interoperability mandates.
- Cross-domain safety monitors for multi-actor environments (Industry; Robotics/Manufacturing/Autonomy)
- Use: Apply HAT over combinatorial complexes to factories, labs, and autonomous systems to capture group interactions beyond pairwise graphs.
- Tools/Workflows: “HAT Safety Monitor” for cobots; crowd-vehicle interaction modules for AVs; lab safety in biotech facilities.
- Assumptions/Dependencies: Domain-specific sensors and priors; re-training on new manifolds; environment calibration.
- Personalized skill and team synergy assessment (Medical Education; Credentialing; Insurance)
- Use: Derive polyadic skill metrics (e.g., synchronization with robot and assistant) from rank-2 cell dynamics for longitudinal assessment.
- Tools/Workflows: “SkillScore Polyadic” dashboards; periodic certification support; risk-adjusted premiums.
- Assumptions/Dependencies: Fairness/bias evaluation; informed consent; standard-setting by boards/insurers.
- Predictive AR coaching and decision support (Medical Training; Intraoperative Guidance)
- Use: Real-time overlays with anticipated steps, risk cues, and safe interaction cones for human-robot collaboration.
- Tools/Workflows: “AR Coach” integrated with microscopes or headsets; adaptive cueing based on HAT confidence.
- Assumptions/Dependencies: User acceptance; low-latency compute; robust tracking; regulatory approval for live guidance.
- Privacy-preserving on-device topological reasoning and federated updates (Policy; Software)
- Use: Keep raw video/audio on-prem while sharing only topological summaries/gradients to train global models.
- Tools/Workflows: Federated TDL pipelines; PII minimization by operating on combinatorial structures.
- Assumptions/Dependencies: Edge compute capacity; secure aggregation; legal frameworks for federated learning.
- Multi-hospital benchmarking tied to clinically meaningful outcomes (Academia/Consortia)
- Use: Evaluate models on metrics like near-miss prevention, team cognitive load, and intraoperative risk reduction (not just F1).
- Tools/Workflows: Shared evaluation protocols; prospective trials; outcome-linked leaderboards.
- Assumptions/Dependencies: IRB approvals; data-sharing agreements; standardized instrumentation.
- Liability, claims, and forensic reconstruction (Insurance; Legal)
- Use: Use tamper-evident topological event logs to reconstruct multi-actor sequences post-incident for fair adjudication.
- Tools/Workflows: Secure logging with cryptographic timestamps; standardized export for legal review.
- Assumptions/Dependencies: Legal admissibility; chain-of-custody processes; privacy protections.
Notes on general feasibility across applications:
- Sensor stack: Requires reliable multi-view video, depth estimation, audio capture, and access to robot logs; performance degrades with heavy occlusion or poor calibration.
- Model robustness: Generalization beyond MM-OR needs diverse data, domain adaptation, and calibration to different room layouts and surgical specialties.
- Human factors: Interfaces must minimize cognitive load and alarm fatigue; explainability of higher-order states is key for trust.
- Governance: Privacy, consent, and cybersecurity are central; deployment must align with regulatory requirements for clinical software and robotics.
Glossary
- Algebraic topology: A branch of mathematics using algebraic tools to study topological structures and relationships. "we propose a generalized framework for surgical reasoning rooted in algebraic topology"
- Attention gating: An attention-based mechanism to select or modulate feature contributions during fusion. "via attention gating."
- Auxiliary evidence nodes: Additional nodes representing non-physical data sources (e.g., audio, logs) linked to entities to inject modality-specific evidence. "We also establish auxiliary evidence nodes to integrate additional modalities"
- Back-projection: Reconstructing 3D information by projecting 2D observations back into 3D space using camera geometry. "we back-project the 2D segmentations into a unified 3D space"
- Boundary cells: Lower-rank cells incident to a higher-rank cell that contribute constituent information upward in a complex. "Information in HAT flows primarily along the incidence structure of : boundary cells () propagate entity-level features upward, while co-boundary cells () distribute aggregated group context downward."
- Boundary neighborhood: The set of lower-rank cells on the boundary of a cell in a combinatorial complex. "we define its boundary neighborhood "
- Cell complexes: Topological structures built from cells (points, edges, faces, etc.) capturing hierarchical relationships. "combining features of cell complexes (hierarchy among relationships) and hypergraphs (arbitrary set-type relations)"
- Clinical priors: Domain-informed assumptions or rules derived from clinical knowledge used to constrain or guide model construction. "by using spatial thresholding and imposing clinical priors."
- Co-boundary cells: Higher-rank cells that a given cell belongs to, providing group context downward. "Information in HAT flows primarily along the incidence structure of : boundary cells () propagate entity-level features upward, while co-boundary cells () distribute aggregated group context downward."
- Co-boundary neighborhood: The set of higher-rank cells that contain a given cell within a combinatorial complex. "and its co-boundary neighborhood ."
- Combinatorial complex (CC): A generalized topological structure composed of cells with a rank function and face relations, unifying graphs, cell complexes, and hypergraphs. "A combinatorial complex (CC) consists of a finite set of cells and a rank function "
- Dyadic: Involving exactly two elements or entities; pairwise. "strictly dyadic structural limitations."
- Face relation: A partial order indicating when one cell lies on the boundary (is a face) of another. "partial ordering denoting the face relation"
- Graph Attention Networks (GAT): Neural networks that apply attention mechanisms over graph neighborhoods. "which generalizes GAT \cite{velivckovic2017graph} from graph neighborhoods to the incidence structure of combinatorial complexes"
- Higher-Order Attention Network (HAT): An attention architecture that operates over the incidence structure of combinatorial complexes, enabling message passing across cells of different ranks. "we introduce Higher-Order Attention Networks (HAT)"
- Higher-order structure: A representation that models relationships among groups of multiple entities (beyond pairs). "models multimodal operating rooms as a higher-order structure"
- Hypercells: Informal term for higher-rank cells aggregating multi-entity interactions within the complex. "within our rank-2 hypercells."
- Hypergraphs: Generalized graphs where edges (hyperedges) can connect any number of nodes. "hypergraphs (arbitrary set-type relations)"
- Incidence neighborhood: The union of a cell’s boundary and co-boundary neighborhoods in a complex. "The full incidence neighborhood is their union:"
- Incidence structure: The relational organization describing which cells are incident (on the boundary or co-boundary) to which others. "flows primarily along the incidence structure of "
- Kinematic tree: A tree-structured model of articulated joints and their connections used to represent motion. "predefined human kinematic trees"
- Macro F1-Score: The unweighted mean of class-wise F1-scores, treating all classes equally. "measured in Macro F1-Score."
- Manifold geometry: The geometric structure of data lying on curved spaces rather than in flat Euclidean space. "flatten the manifold geometry inherent to relational structures"
- Non-Euclidean (data): Data that reside on spaces not well-modeled by flat Euclidean geometry (e.g., manifolds, groups). "inherently non-Euclidean data"
- Partial ordering: A binary relation that is reflexive, antisymmetric, and transitive, used here to encode face relations among cells. "The CC is endowed with a partial ordering denoting the face relation,"
- Polyadic: Involving more than two entities simultaneously. "surgical procedures are irreducibly polyadic."
- Rank embeddings: Learnable vectors associated with cell ranks to modulate attention across different ranks. "where are learnable rank embeddings"
- Rank function: A mapping assigning an integer dimension (rank) to each cell in the complex. "a rank function "
- Rank-pair bias: Attention bias term conditioned on the ranks of the source and target cells to preserve structural heterogeneity. "The rank-pair bias modulates information flow based on the topological relationship between source and target cells."
- Rank-2 cells: Two-dimensional cells in the complex used to aggregate higher-order (group) interactions. "Rank-2 Cells () for Higher-Order Behavior."
- SE(3): The Lie group of 3D rigid-body motions (rotations and translations). "including articulated 3D human motion in "
- Semantic bottleneck: A compression in representation (e.g., via tokenization) that discards geometric/topological information. "tokenizing forces this inherently non-Euclidean data through a semantic bottleneck"
- Spatio-temporal complex: A combinatorial complex extended over time by linking entities across frames. "we combine consecutive frames into a spatio-temporal complex"
- Surgical scene graphs (SSGs): Graphical representations encoding entities (people, tools) and their relations within surgical environments. "Surgical scene graphs (SSGs) were later conceived to formally structure the complexity of the entire operating theater"
- Topological cells: Basic elements (of various ranks) in a topological complex representing entities and relations. "lifting interactions between entities into higher-order topological cells"
- Topological deep learning (TDL): Deep learning methods operating on topological structures like complexes and hypergraphs. "using the topological deep learning (TDL) framework"
- Vision-LLM (VLM): Models that jointly process visual and textual data in a shared representation space. "VLM-based approaches attempt to sidestep explicit graph construction"
- Zero-shot: Performing a task without task-specific training examples by leveraging generalized representations or rules. "enabling zero-shot, rule-based sterility breach detection."
Collections
Sign up for free to add this paper to one or more collections.

