- The paper introduces APRIL-MedSeg, a framework that modularizes 2D segmentation into Encoder, Bottleneck, Skip, and Decoder components for versatile model configuration.
- It leverages a YAML-driven registry supporting 177 encoders, 17 bottlenecks, 45 decoders, and 25 skip connections to simplify experiment management and reproducibility.
- The framework incorporates advanced paradigms such as semi-supervised learning, domain adaptation, knowledge distillation, and text-guided segmentation to enhance clinical applications.
APRIL-MedSeg: Modularizing the Medical Image Segmentation Stack
Motivation and Context
Medical image segmentation is instrumental for clinical diagnosis, treatment planning, and automated analysis. While domain-agnostic vision toolkits and later medical-specific libraries have matured, they exhibit fragmentation across architecture coverage, training paradigms, and support for recent foundation models or configuration-driven experimentation. APRIL-MedSeg (2606.30577) is proposed as a comprehensive modular framework to address these deficits, offering systematic unification and extensibility for 2D medical image segmentation.
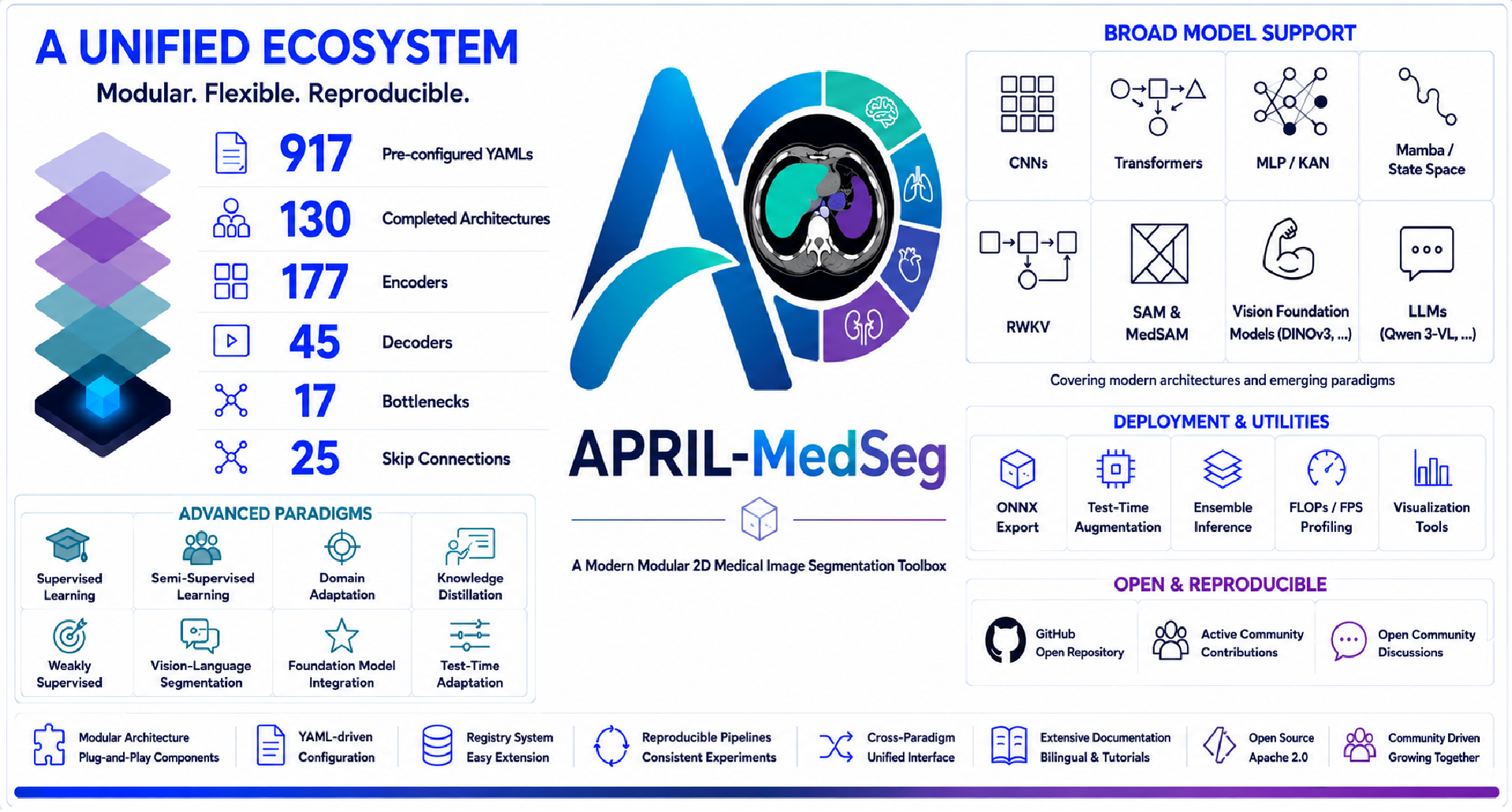
Figure 1: APRIL-MedSeg, a unified modular framework for medical image segmentation that integrates architectures, training paradigms, and deployment pipelines under a configuration-driven system.
Modular Design and Architecture Abstraction
APRIL-MedSeg formalizes almost all 2D segmentation networks as compositions of four interchangeable modules: Encoder, Bottleneck, Skip Connection, and Decoder. Each is independently implemented and orchestrated through a Python registry/configuration paradigm, enabling factorial combinatorial mixing (177×45×25×17 possible instantiations), and declarative experiment management via YAML.
- Encoder Registry: 177 entries, including 39 foundation models spanning 9 modalities, exposing any model from the timm library with dynamic wrappers. Supports classic CNNs (UNet, DenseNet), ViTs and hybrids (TransUNet, SwinUNet), SSMs/Mamba, RWKV, KAN/MLP, and medical/vision-language pretrains.
- Bottleneck Registry: 17 modules, from vanilla to spatial-/channel-attentive, MoE, and LLM-augmented representations.
- Decoder Registry: 45 implementations, across basic upsampling, MLP-based, transformer-based, hierarchical pyramid, and attention-based strategies.
- Skip Connections: 25 designs including basic copy, spatial/channel/transformer/mamba-based attention, CNN fusions, and adaptive/mixture gating.
The registry ensures FAIR model composition, weight management, and explicit support for hundreds of backbones and plug-ins. Comprehensive YAML inheritance significantly reduces configuration duplication and facilitates reproducible research.
Modern Paradigms: Beyond Supervised Learning
APRIL-MedSeg differentiates itself by unifying advanced learning paradigms critical for data-constrained and deployment-centric medical imaging:
- Semi-supervised & Weakly-supervised Segmentation: 40+ approaches, leveraging consistency (Mean Teacher, Pi-Model, UniMatch), pseudo-labeling (FixMatch, SoftMatch), co-training (CCT, Deep Co-Training), as well as non-dense annotation regimes (bounding box, scribble, image-level, point) including BoxInst, CAM, and SEAM.
- Domain Adaptation: 18 methods (DANN, AdvEnt, FDA, MIC, DAFormer), addressing cross-hospital and cross-modal generalization.
- Knowledge Distillation: 27 techniques encompassing feature/logit/relation-level supervision, plus medical-specific anatomical and boundary-aware variants.
- Text-guided Segmentation: 12 trainable VLMs (CRIS, LViT, BiomedParse, etc.) and a zero-shot pipeline combining MLLMs with SAM-style promptable segmentation.
All strategies are supported with 81 loss functions and automatic deep supervision in a zero-code manner, maximizing experimental flexibility and reproducibility.
Foundation Model Integration
A distinct strength is the tight integration of foundation models as feature encoders. This covers generic vision and medical-specific models (e.g., DINO[v2/v3], CLIP, BiomedCLIP, MedSAM, Qwen-VL, Rad-DINO, MedGemma), covering radiology, pathology, dermatology, endoscopy, ophthalmology, ultrasound, and more. Multi-block feature extraction via unified DPT heads ensures architectural consistency for downstream decoders. Fine-tuning strategies support full/frozen/partial updating, suiting varying dataset sizes and deployment constraints.
Data, Augmentation, and Deployment
APRIL-MedSeg provides unified interface wrappers for 26 datasets spanning 8 medical imaging modalities, with support for binary, multi-class, domain adaptation, semi-supervised, and VLM text-image pair tasks. Its augmentation suite includes geometric, pixel-level, masking, and sample-level techniques, all YAML-configurable for stochasticity control or reproducibility.
Deployment features include ONNX export, FLOPs and FPS profiling, test-time augmentation (multi-scale/flip), and ensembling, all configurable from YAML, facilitating clinic-ready inference without workflow scripting.
Ecosystem, Documentation, and Usership
Full code and pretrained weights are available under Apache 2.0. Documentation is bilingual and spans modular concepts, configuration-driven workflows, foundation model modification, advanced paradigm integration, and deployment. Tutorials cater to rapid onboarding for both clinical practitioners and research students, with scenarios detailed for architecture R&D, paradigm benchmarking, and clinical prototyping.
The userbase includes low-level algorithm designers, training paradigm researchers, clinicians seeking out-of-the-box workflows, and educators aiming for progressive theory/practice coverage.
Implications and Future Developments
APRIL-MedSeg positions itself as a bridge between evolving deep learning methodologies and real clinical constraints. By formalizing the architecture/paradigm/configuration/deployment pipeline, it enables systematic, reproducible, and cross-comparable empirical studies—addressing stagnation in the architecture expansion and paradigm coverage observed in legacy medical vision toolkits.
While current focus is on 2D segmentation, the extensible registry/config ecosystem lays a foundation for 3D/volumetric and video tasks. The inclusion of text-guided and foundation model pipelines anticipates the growing uptake of zero-shot and open-vocabulary clinical AI systems. Its modularity reduces engineering barriers to introducing next-generation efficient models (Mamba/SSM, prompt-driven VLMs), as well as new compositional training paradigms, making the platform suitable for future AI R&D cycles where rapid model turnover and thorough benchmarking are required.
Conclusion
APRIL-MedSeg (2606.30577) establishes a general-purpose, highly modular framework that unites modern architectures, efficient training paradigms, foundation model adaptation, and deployment utilities for 2D medical image segmentation. Its systematic abstraction and zero-code configurability address reproducibility, flexibility, and efficiency requirements for both research and clinical translation, and create a scalable testbed for developing the next generation of medical vision AI systems.

