- The paper introduces a novel graph-based method to transform longitudinal EHRs into structured, provenance-linked data.
- The methodology leverages hierarchical MEDS and TOA graphs to accurately resolve clinical events and optimize query speed.
- Empirical evaluation shows a 34-fold speedup and 96.4% extraction accuracy, outperforming conventional LLM-based workflows.
VISTA Architect: Database-Oriented Health AI System for Longitudinal Clinical Reasoning
Architectural Overview
VISTA Architect operationalizes a database-oriented approach to health AI by leveraging hierarchical graph databases—specifically, the source-faithful MEDS Graph and the abstraction-driven Timeline Object Architecture (TOA) Graph—for representing and reasoning over longitudinal EHR data. The architecture systematically transforms raw EHR records into persistent, provenance-linked graph structures, facilitating agentic AI interactions that bypass inefficiencies and limitations of repeated raw-text processing inherent in conventional LLM-centric workflows.
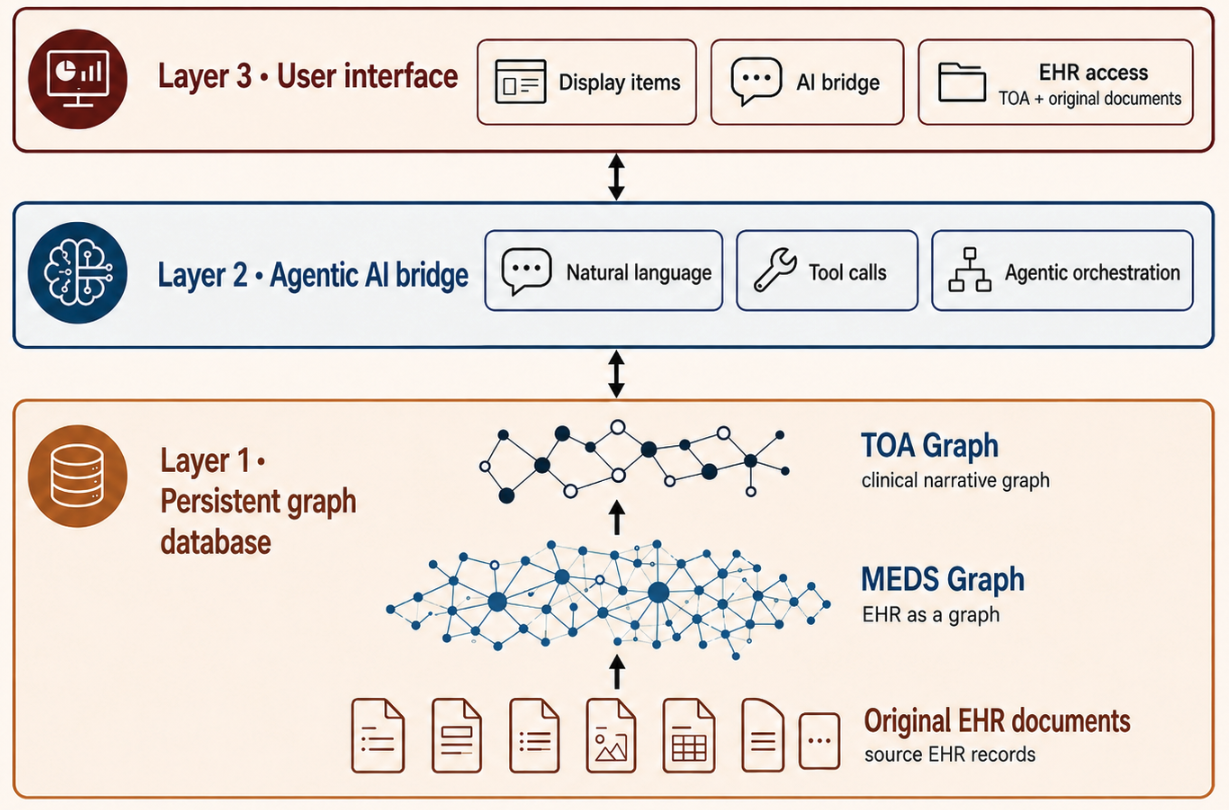
Figure 1: VISTA Architect system design illustrating conversion of source EHRs into graph databases, enabling agentic queries and provenance-linked access via a unified interface.
The MEDS Graph preserves original document granularity, instantiating clinical artifacts such as patient demographics, encounters, notes, measurements, and imaging data as nodes with explicit temporal and visit-level relations as edges. In contrast, the TOA Graph abstracts these into clinically meaningful, temporally resolved events and episodes (diagnosis, treatment lines, post-oncology phases), each linked back to underlying sources for maximal auditability and determinism. This pre-computed abstraction amortizes longitudinal synthesis complexity, optimizing downstream agentic queries for speed and accuracy.
Temporal Clinical Structuring and Representation
Central to VISTA Architect is the synthesis of a temporally ordered clinical narrative from fragmented EHR events, leveraging graph-guided LLM extraction. The architecture resolves distributed mentions of events (e.g., diagnosis, molecular testing, treatment initiation) into deduplicated TOA nodes, each annotated with inferred occurrence timestamps rather than documentation artifacts, capturing actual clinical progression independent of inconsistent note chronology.
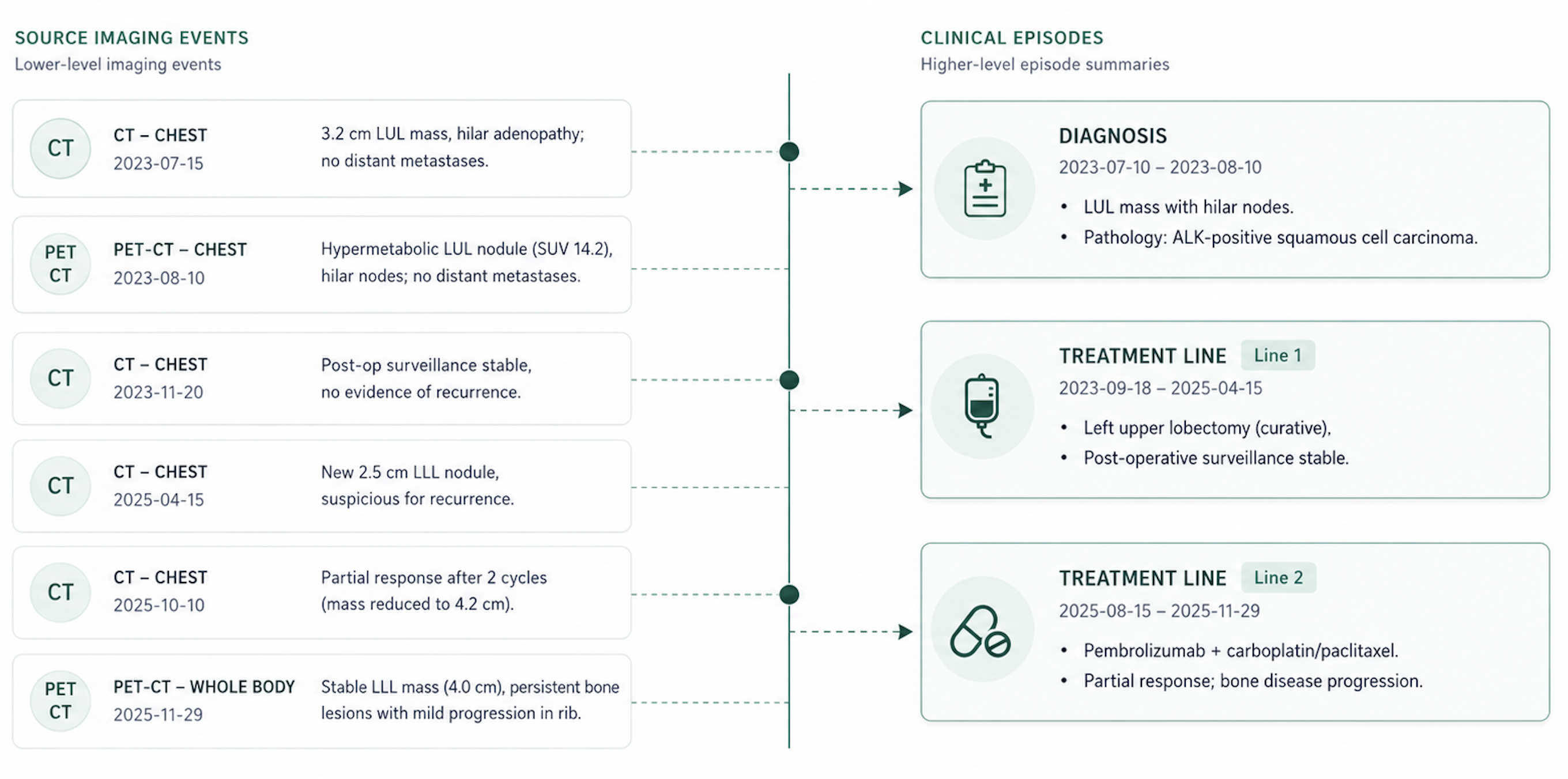
Figure 2: TOA-based timeline organization, mapping granular imaging events from the EHR to episode summaries anchored by anatomical and temporal coherence.
Episodes in the TOA layer are automatically segmented by domain-specific configuration, grouping events by anchors such as imaging studies or specific encounters within clinically meaningful windows. The episode model supports flexible adaptation to domain requirements, exemplified by thoracic oncology's use of treatment lines and baseline–diagnosis–post-treatment episodic stratification.
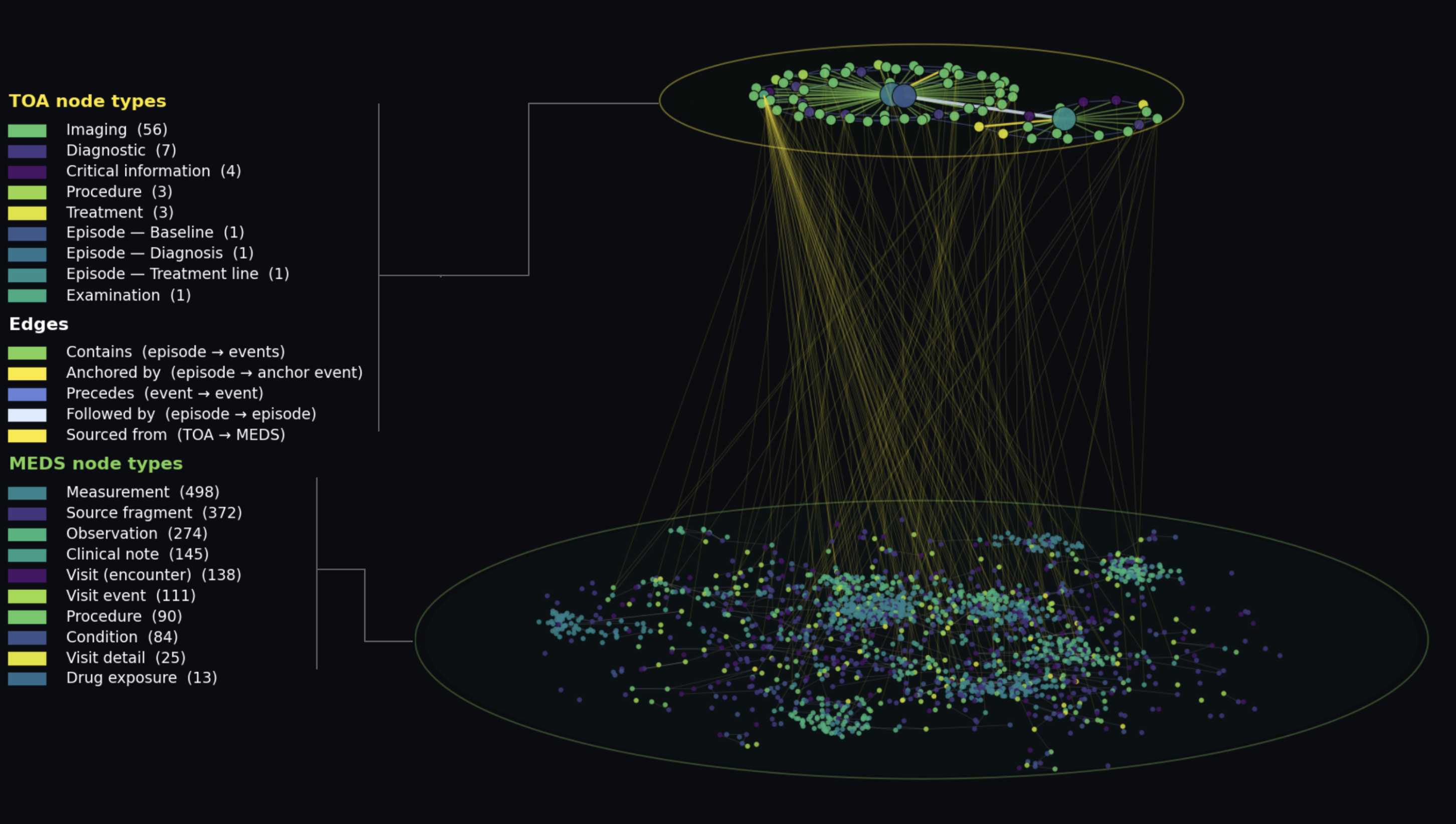
Figure 3: Two-tier graph structure for a representative patient, showing source-level MEDS Graph nodes and abstracted TOA episode and event nodes with explicit provenance and clinical relationships.
Agentic AI Bridge and User Interaction
VISTA Architect exposes its graph-resident artifacts through a unified agentic interface, enabling natural language queries, dashboard population, automated documentation, and graph-guided retrieval with deterministic provenance. By operating over a pre-synthesized clinical context, agents answer most queries directly from the TOA layer, resorting to targeted traversal into raw MEDS Graph nodes only when source-level validation is required. This fundamentally changes retrieval dynamics relative to conventional retrieval-augmented generation (RAG), as clinical navigation is strictly determined by graph structure rather than semantic similarity metrics.
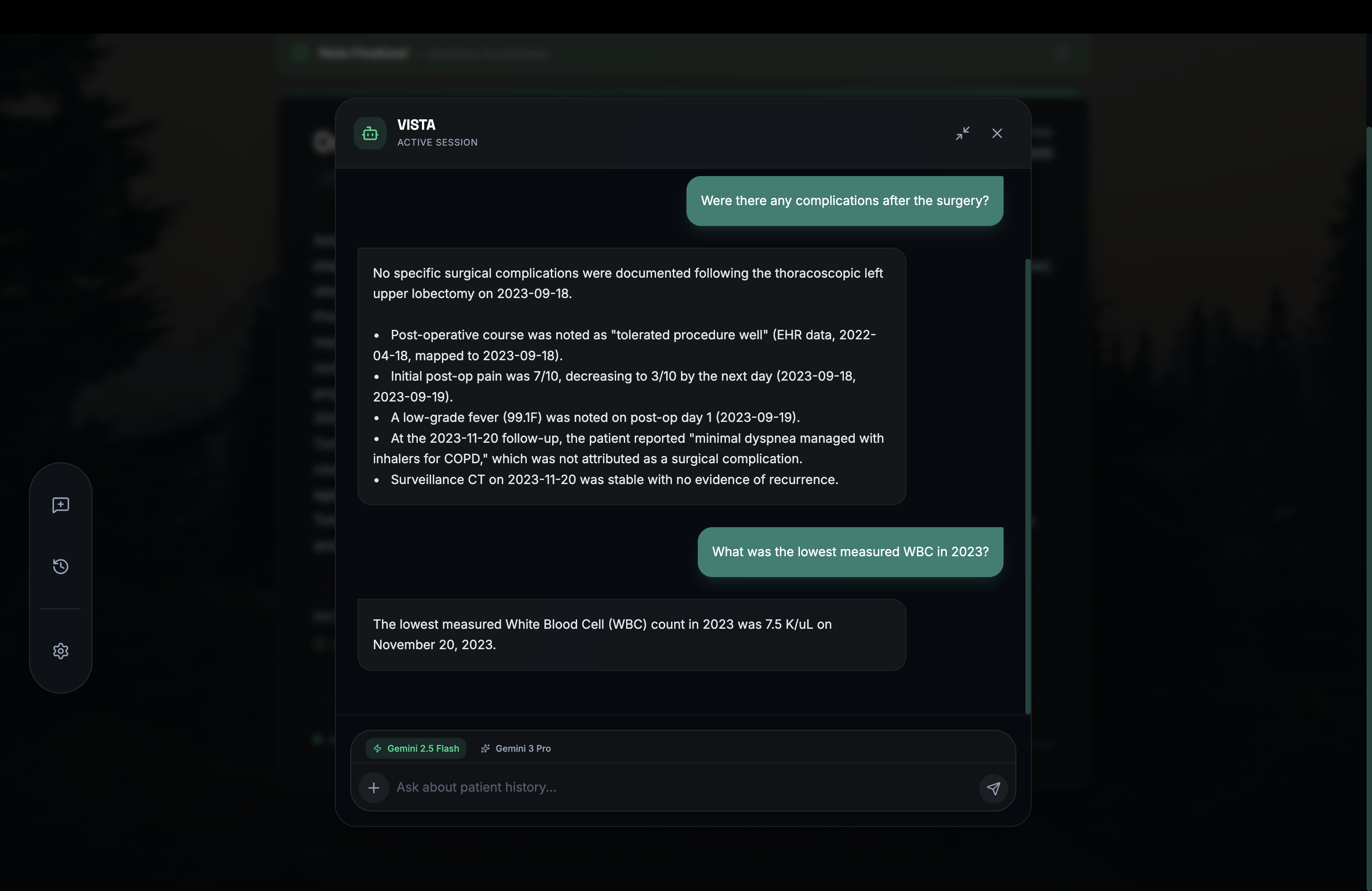
Figure 4: Chat interface leveraging graph-guided agentic retrieval, providing provenance-linked answers from TOA and MEDS layers.
User-facing applications—including patient overviews, clinical timelines, automated tumor board notes, and interactive chats—are rendered directly from graph artifacts, ensuring consistent, explainable outputs for both human and AI interactions.
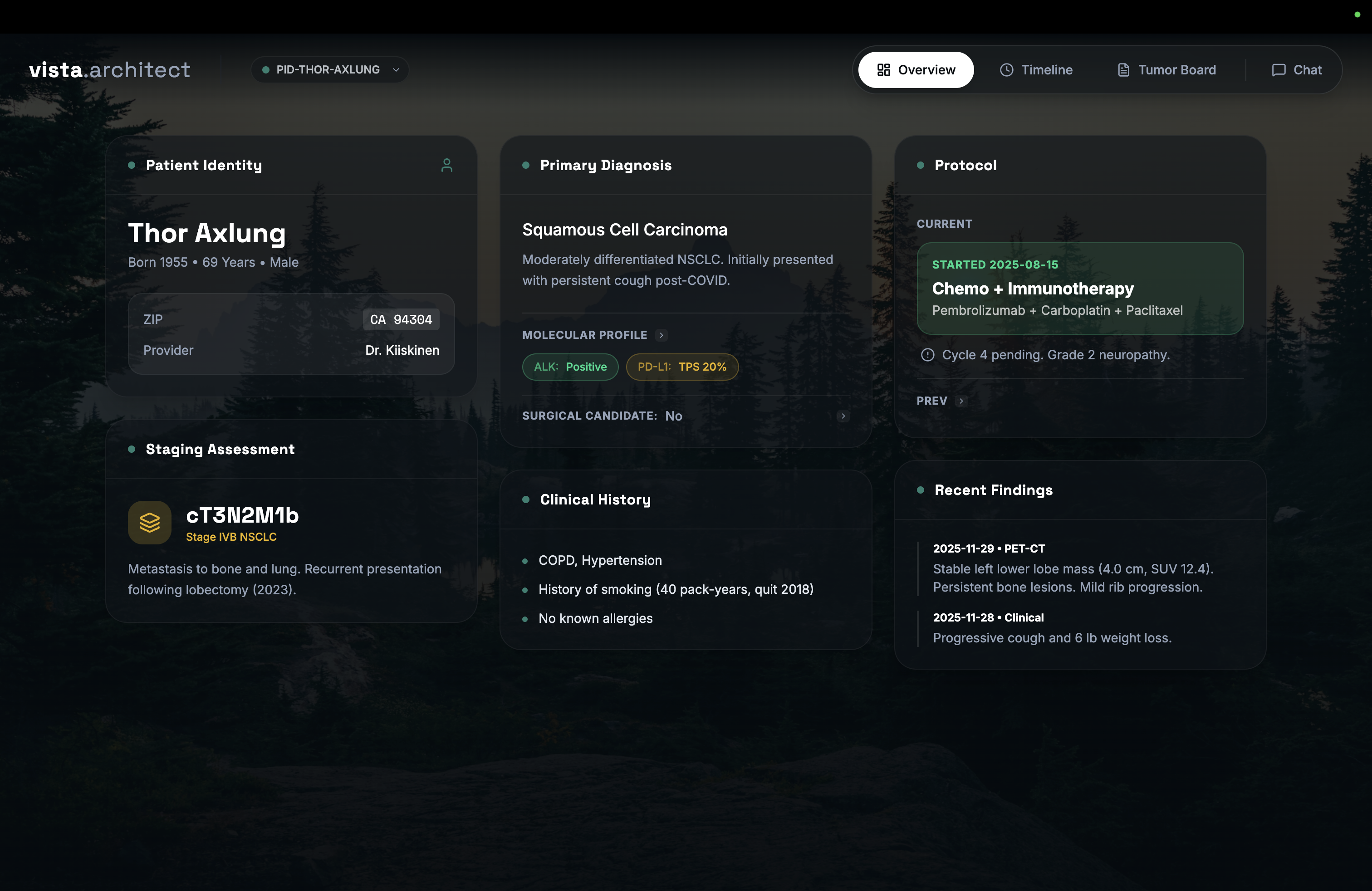
Figure 5: System-generated patient Overview from graph-resident artifacts, displaying key clinical fields and current findings.
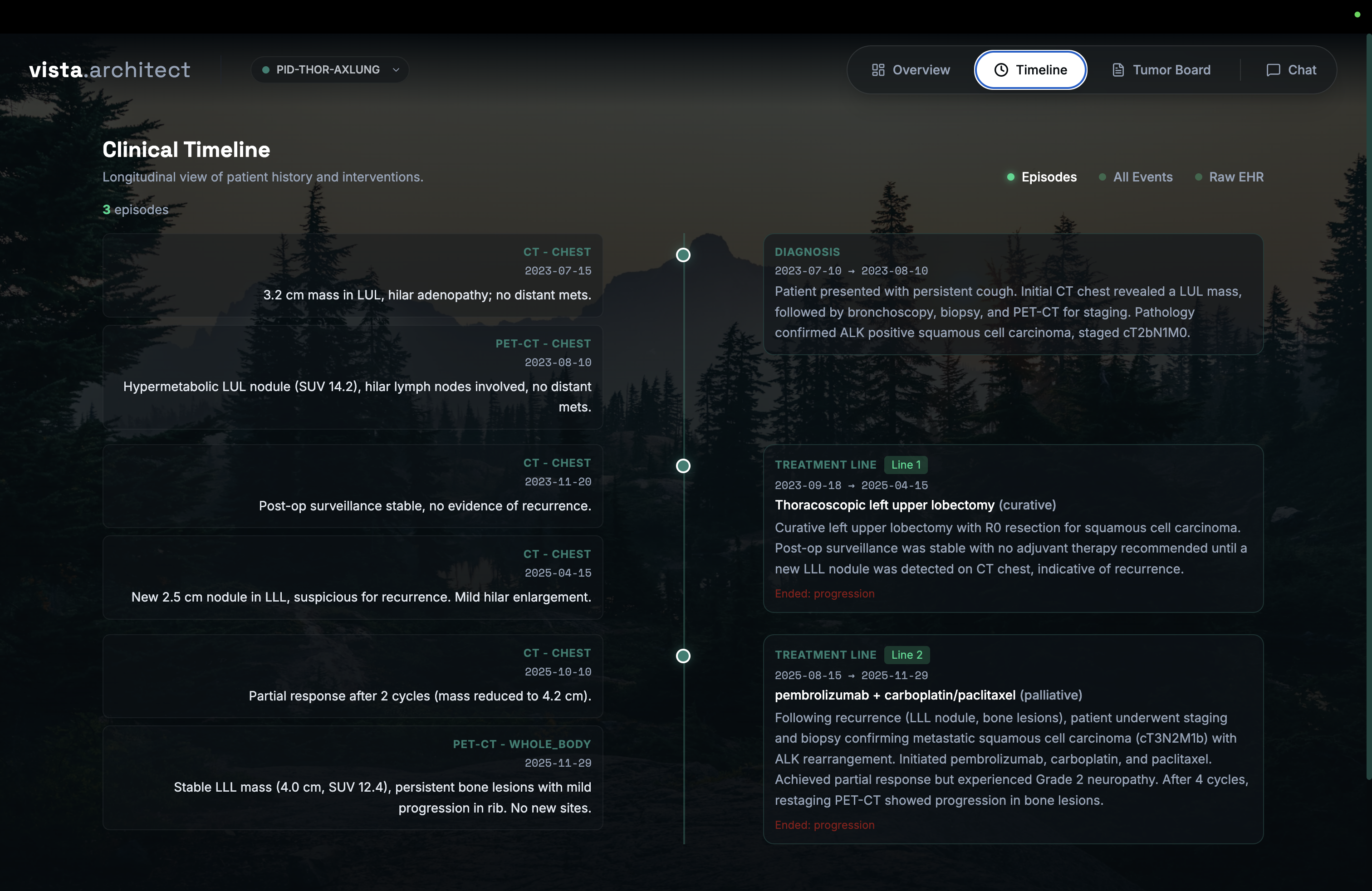
Figure 6: Clinical Timeline view organizing longitudinal episodes and corresponding granular events, with toggles for provenance and full event logs.
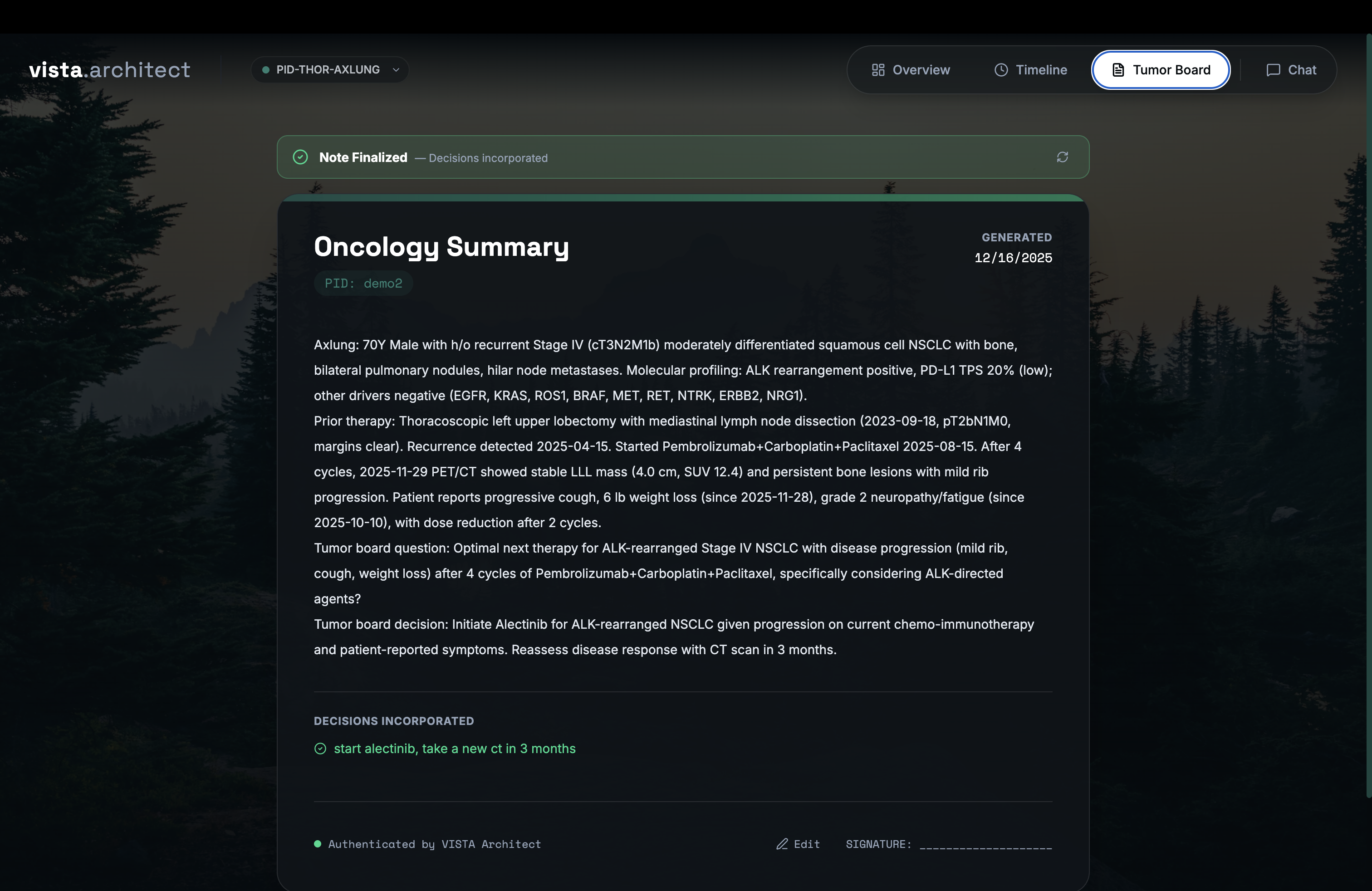
Figure 7: Automated pre-tumor-board summary note generation from the clinical graph, consolidating full patient history and tumor board decisions.
Empirical Evaluation and Benchmarking
In a rigorous cohort analysis spanning 1,180 thoracic oncology patients and 17,700 clinical variable evaluations, VISTA Architect demonstrated superior extraction accuracy (96.4%, mean 9.75/10), outperforming LLM-driven RAG baselines (66.7–66.9%, mean 7.6–7.7/10) and recent agentic multi-agent orchestration benchmarks. Accuracy remained robust for all clinical variable categories, with Date of Birth and Sex serving as positive controls achieving perfect scores; time-varying and collection variables (e.g., Previous Surgery, Metastasis, Radiation Therapy) exhibited high reliability predicated on temporal resolution and document synthesis, unlike RAG's substantial drop-off in these domains.
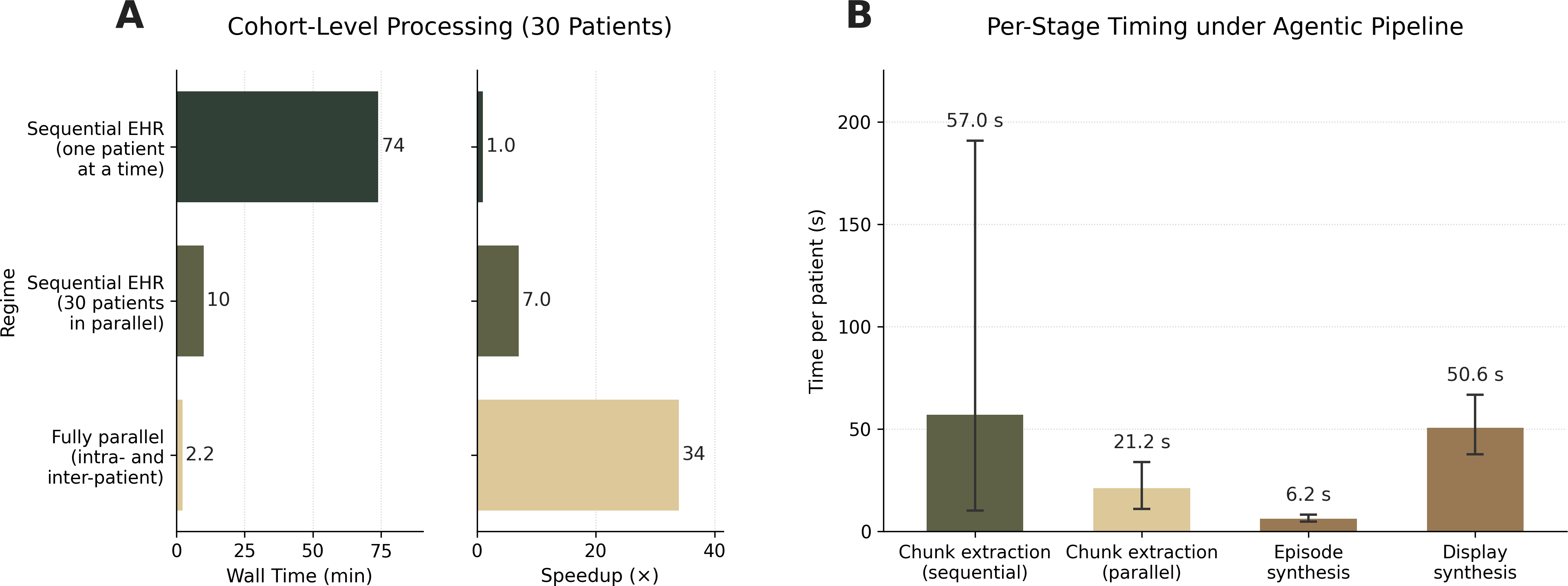
Figure 8: MEDS Graph construction performance displaying linear scaling for build time and peak memory with increasing patient record size; all graphs constructed in under one second and 20 MB.
The pre-computation paradigm enabled dramatic improvements in system throughput and latency, achieving a 34-fold speedup in agentic build times for a 30-patient cohort (2.2 minutes), compared to sequential LLM workflows, with deterministic graph traversal operations executing in sub-millisecond times.
Graph-Guided Cohort Retrieval and Clinical Utility
VISTA Architect supports direct cohort-wide patient retrieval without secondary EHR processing, exemplifying its utility in precision oncology settings. The patient similarity module leverages pre-computed graph artifacts—driver mutation profiles, treatment trajectories, narrative summaries—to surface clinically relevant comparator cases in milliseconds, facilitating real-time contextual evidence accrual during tumor board deliberation. Weighted multi-component retrieval enables configurable scoring across biological, trajectory, and narrative facets, with the LLM only invoked for final clinical judgment.
Implications, Scalability, and Future Directions
VISTA Architect elucidates a pre-computation regime for health AI: structured, temporally-aware graph construction transforms the information extraction and retrieval landscape from costly per-query searches into deterministic, provenance-tracked traversals. Decoupling expensive LLM synthesis from recurrent querying enables high accuracy, scalability, and temporal fidelity in complex clinical domains. The architecture’s modularity and configuration flexibility make it extensible to other specialties and document-centric high-stakes domains, though empirical validation outside thoracic oncology remains an open area.
From a systems perspective, this approach addresses the context-length bottleneck and semantic fragmentation inherent in longitudinal EHRs, while aligning retrieval and abstraction strictly to clinical structures rather than lexical or semantic similarity. The persistent graph representation supports agentic orchestration, reproducible dashboards, cross-patient analytics, and automated clinical documentation from a single substrate, enhancing both efficiency and reliability.
Future work will interrogate architecture generalizability across institutions, languages, and multimodal sources, as well as expand ablation analyses for each layer’s contribution, explicit temporal normalization validation, expanded clinician adjudication, and optimized RAG baselines including dense embedding and long-context models. Integration with population-scale graph stores (e.g., Neo4j) and multimodal asset linking (imaging, genomics) is anticipated.
Conclusion
VISTA Architect demonstrates that amortized graph-based abstraction of longitudinal EHRs, coupled with agentic AI interfaces, substantially advances clinical information extraction, retrieval, and decision-support, particularly in multidisciplinary oncology settings. By precomputing structured, temporally resolved, provenance-linked patient narratives, the system achieves deterministic, high-fidelity reasoning that substantially exceeds conventional LLM- or RAG-based workflows in both accuracy and speed. The architectural principles delineated herein have broad implications for health AI deployments requiring longitudinal context, reliability, and scalable agentic querying (2606.22692).