- The paper presents a novel ASFOSDA framework that adapts to open-set conditions without reusing source data.
- It leverages decomposed class-aware uncertainty and prototype discrepancy for active sample selection and robust self-training.
- Experiments on CT and MR segmentation show improved DSC scores and efficient use of limited annotated data.
Active Source-Free Open-Set Domain Adaptation for Medical Image Segmentation
Introduction and Problem Statement
This work introduces Active Source-Free Open-Set Domain Adaptation (ASFOSDA) for medical image segmentation, targeting clinically realistic scenarios where domain shift, data privacy, and open-set label space variances are concurrent. Existing domain adaptation approaches in medical image segmentation predominantly assume closed-set conditions (identical label spaces across domains) and require source domain access during adaptation. However, clinical deployment often prohibits source data access due to privacy constraints and must handle new, unseen anatomical classes (open-set condition) in the target domain. ASFOSDA provides a solution by enabling adaptation without revisiting source data, leveraging active sample selection, and explicitly addressing the open-set semantic gap.
Methodological Advances
ASFOSDA employs a two-fold methodological structure encapsulating an active open-set query strategy and a target-refined self-training regimen. The system sequentially identifies and annotates maximally informative target samples—both within known and unknown class regions—crucial for effective knowledge transfer in the open-set, source-free adaptation regime.
Active Open-set Query Strategy
The core of the sample selection is grounded in Class-aware Decomposed Uncertainty (CDU) and Class-agnostic Prototype Discrepancy (CPD):
- CDU integrates class-aware aleatoric (CAU) and epistemic uncertainty (CEU), estimating both intrinsic data ambiguity and model representation variance via test-time augmentation. The uncertainty quantification is conducted independently for classes unknown to the source, enhancing sensitivity to novel anatomical/pathological structures.
- CPD evaluates both cross-domain discrepancy (distance between high-uncertainty “target” samples and low-uncertainty “source-like” samples in embedding space) and self-domain diversity (redundancy reduction among high-uncertainty samples). Low uncertainty samples form anchors representing transferred source knowledge, while high-uncertainty samples—well-separated in semantic space—are prioritized to maximize the acquisition of target-specific features.
These strategies are visualized in the overall pipeline schematic.
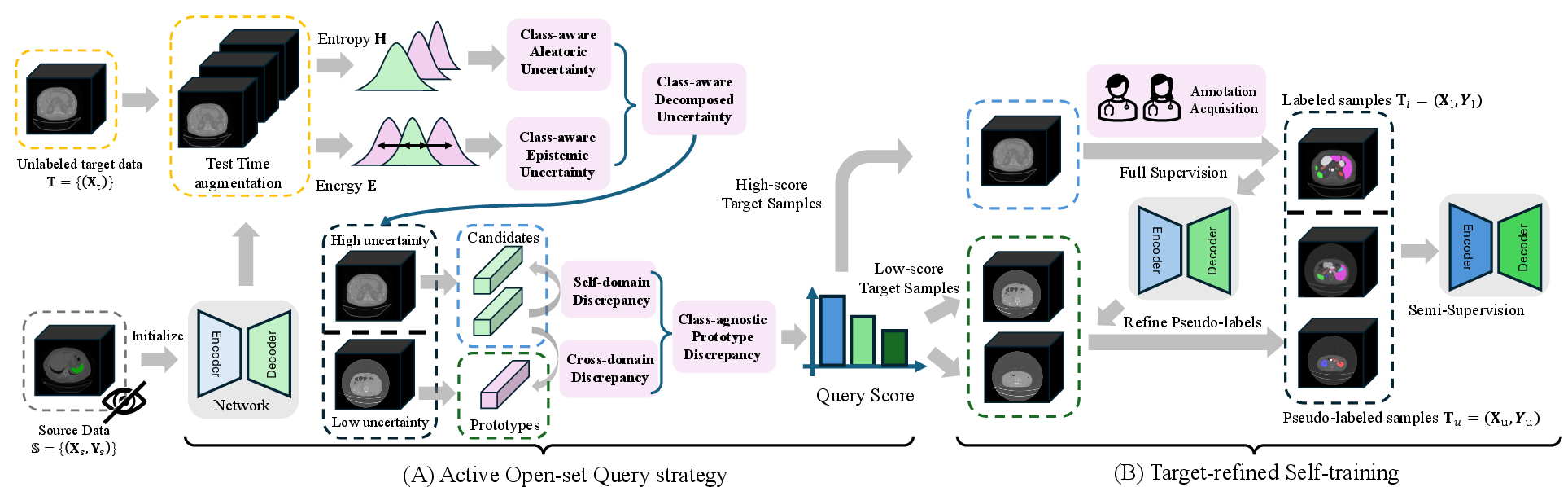
Figure 1: Architecture of ASFOSDA highlighting the open-set active query strategy leveraging decomposed uncertainty and prototype-based discrepancy, followed by semi-supervised adaptation with pseudo-labeled and annotated samples.
Target-refined Self-training
ASFOSDA circumvents the well-established pitfalls of noisy pseudo-labels by introducing a two-stage semi-supervised fine-tuning process:
- The model, initialized from the source domain, is first updated using actively selected and manually annotated target samples.
- The refined model then generates pseudo-labels on the undecided pool, increasing their reliability. Final adaptation amalgamates true and pseudo-labels via a joint loss.
This approach capitalizes on labeled data efficiency and enhances generalization under substantial class divergence and distributional shift.
Experimental Design and Quantitative Analysis
ASFOSDA was evaluated on multi-organ volumetric segmentation tasks involving pronounced open-set transformations (e.g., transitioning from datasets with 1 to 14 organ classes) in both CT and MR domains. The main evaluation networks were 3D U-Net and Swin UNETR architectures, with performance reported using Dice Similarity Coefficient (DSC) and 95% Hausdorff Distance (95HD).
ASFOSDA is benchmarked against a broad suite of source-free DA (SFDA) and active source-free DA (ASFDA) baselines, including prominent selection heuristics—entropy, least confidence, core-set, etc.
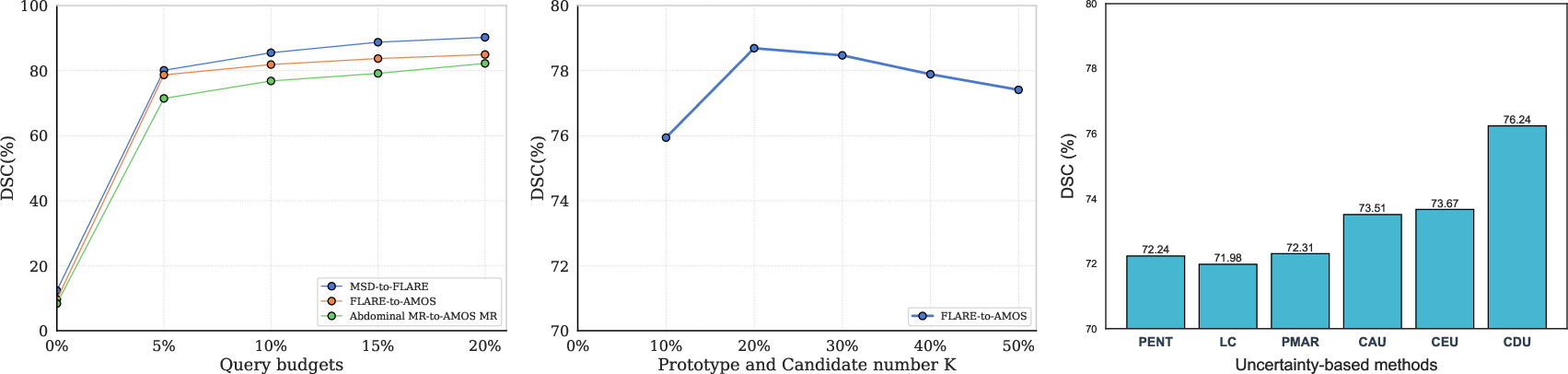
ASFOSDA achieved the following strong numerical results:
- MSD Spleen→FLARE (U-Net): DSC 80.11% ± 8.01, 95HD 5.20mm ± 6.22 (with 5% annotation budget), up to 84% of the fully supervised upper bound.
- FLARE→AMOS CT (U-Net): DSC 78.69% ± 8.87, 95HD 5.75mm ± 6.38, reaching 85.31% of the oracle.
- Abdominal MR→AMOS MR (U-Net): DSC 71.46% ± 8.42, 95HD 8.78mm ± 9.82, representing ~82% of the oracle.
Consistent improvements over all SFDA/ASFDA baselines were observed across networks and domains, with statistical significance (p<0.01 Mann-Whitney U test).

Figure 2: Qualitative segmentation demonstrating improved accuracy of ASFOSDA over SFDA and prior ASFDA approaches in adapting to AMOS CT and MR datasets.
Ablation and Component Analysis
A series of ablation experiments establish the importance of each ASFOSDA component:
Implications and Future Directions
ASFOSDA's capacity to achieve high adaptation accuracy with minimal labeled data, while accommodating unknown classes and adhering to strict data privacy, positions it as a practical framework for real-world deployment of medical segmentation models in federated or privacy-restricted environments. The explicit modeling of open-set semantics and the dual-decomposed uncertainty formulation mark important conceptual advancements for adaptive medical imaging systems.
Potential future developments include extending the approach to multi-modal imaging, integrating with larger-scale vision foundation models, and generalizing the decomposed uncertainty principles to other tasks involving distributional/semantic gaps (e.g., rare disease phenotyping, continual medical learning settings). Efficient uncertainty calibration and dynamic adaptation budget optimization remain open topics for further investigation.
Conclusion
ASFOSDA addresses the critical confluence of open-set domain adaptation, source-free deployment, and annotation efficiency in medical segmentation. Through decomposed class-aware uncertainty, prototype-based sample diversity, and robust semi-supervised adaptation, it quantitatively surpasses established baselines under realistic clinical conditions and sets a precedent for the next generation of adaptive, privacy-conscious medical AI systems.