- The paper reviews how integrating generative LLMs, discriminative vision models, and dental-specific foundation models enhances clinical reasoning and diagnostic performance.
- The paper details adaptation strategies, such as dual-encoder integration and UNet refinement, achieving high segmentation accuracy (Dice ~0.90) in dental imaging.
- The paper emphasizes the need for integrated, auditable AI pipelines to overcome individual model limitations and ensure clinically safe deployment.
Large AI Models in Dental Healthcare: Paradigm Integration, Specialization, and Clinical Implications
Introduction
Oral diseases constitute a substantial global health burden, necessitating robust technological solutions for clinical, diagnostic, and educational challenges in dentistry. The reviewed paper systematically examines the landscape of large-scale AI models in dental healthcare, dissecting how architectural paradigms and the degree of domain specialization influence model performance, integration strategies, and clinical applicability (2606.02914). The analysis spans language-generative models, discriminative vision foundation models, and dental-specific foundation models, mapping methodological progress and their practical interplay.
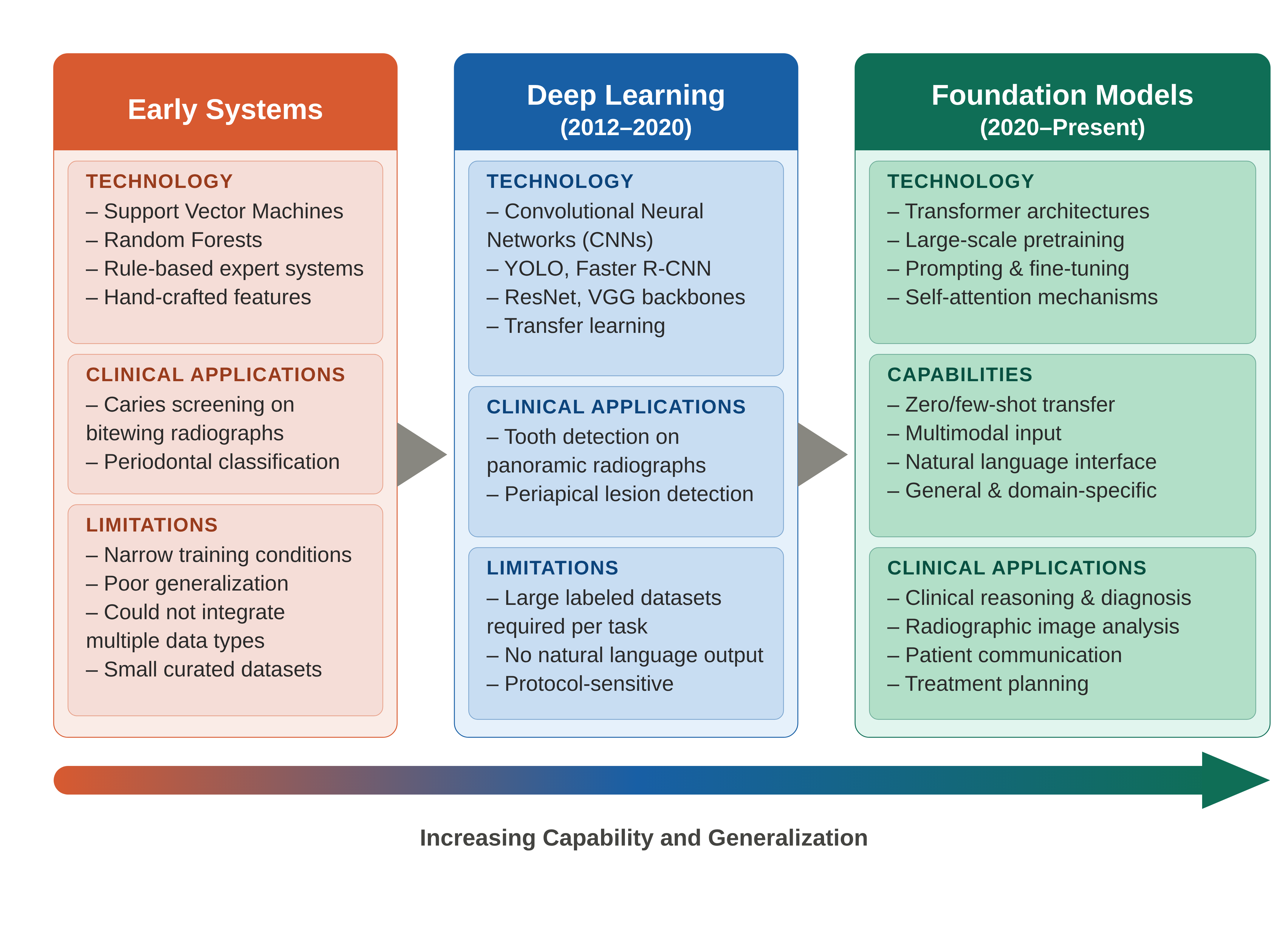
Figure 1: The evolution of AI in dentistry, demonstrating transitions from rule-based and shallow ML systems to multimodal and foundation models with increasing clinical generalization and application diversity.
Classification Framework for Dental AI Models
The taxonomy proposed organizes large dental AI models along two primary axes: architectural paradigm and degree of dental specialization. The former dichotomizes models into language-generative systems (e.g., LLMs, LVLMs) and discriminative vision models (e.g., SAM, CLIP, GroundingDINO); the latter stratifies models by progression from zero-shot, inference-time strategies, through parameter-efficient fine-tuning, up to full domain-specific pretraining.
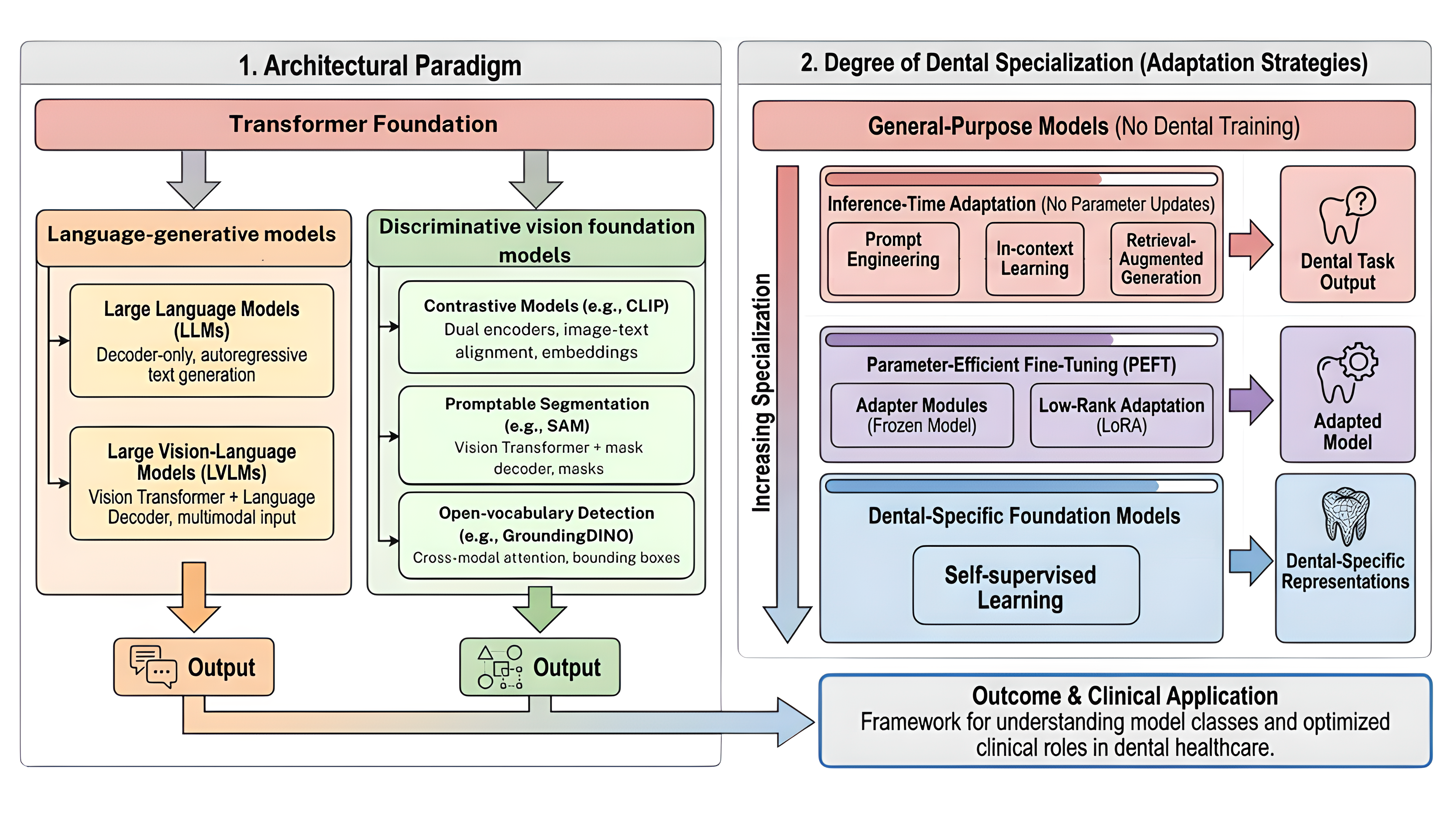
Figure 3: AI model paradigms (left) and adaptation spectrum (right) illustrating how model classes and specialization tiers organize methods and clinical task alignment.
Analysis of 97 studies reveals a concentration of dental-specific pretraining within the vision model family, a reflection of data availability discrepancies: large image datasets are prevalent, whereas extensive dental text corpora remain scarce. The paradigm-specialization interplay thus shapes both the research landscape and practical deployment.
Clinical Reasoning and Diagnosis
LLMs exhibit high accuracy (80-95%) in text-based reasoning and question-answering tasks (e.g., licensing examinations, guideline-based clinical queries) but significant performance attenuation (45-68%) on image-dependent diagnostic tasks, a result replicated across multiple national licensing examinations (Korea, Japan, Taiwan, Turkey, USA). Prompt engineering, in-context learning, and RAG reduce hallucination and enhance answer quality, but cannot bridge the visual reasoning deficit.
Education
LLMs outperform many dental students on standardized text-based assessments, providing effective tools for simulation, case-based learning, and reflective assignments. However, output reliability and temporal consistency are variable, and image-based clinical reasoning remains unresolved.
Patient Communication and Reporting
LLMs provide readable, empathetic, and well-structured responses in patient Q&A and report simplification, with strongest performance on routine, non-complex queries. Standalone LLM output, however, continues to risk hallucination and occasional factual inaccuracy.
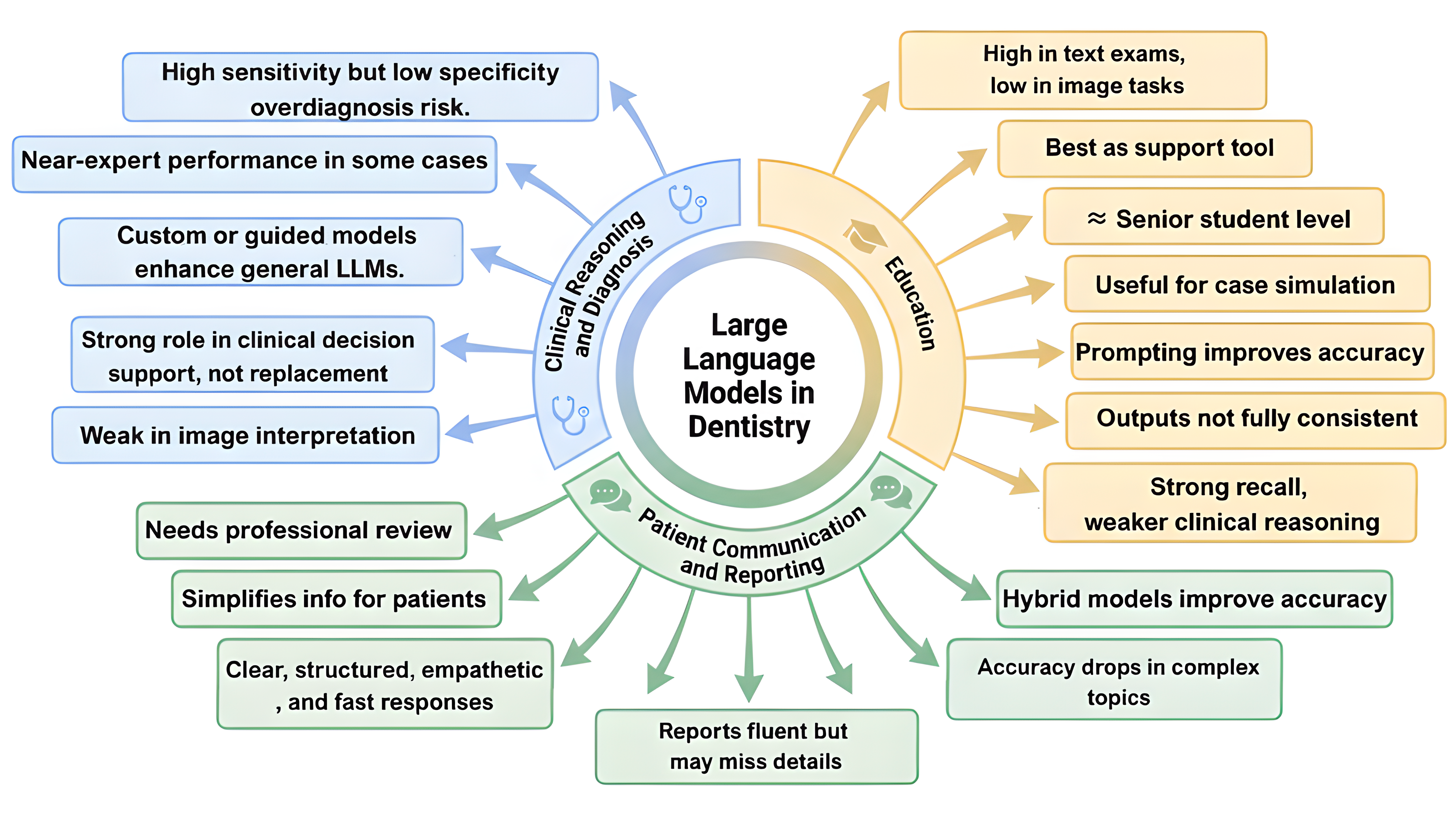
Figure 2: Summarizes major outcome themes for LLM application in clinical, educational, and communication contexts.
Discriminative Vision Foundation Models: Adaptation and Domain Shift
Discriminative vision models (SAM, CLIP, GroundingDINO) require substantive adaptation to dental tasks due to imaging domain shift: complex anatomical overlaps, modality-specific artifacts, and the necessity for high spatial resolution.
Six core adaptation strategies for SAM are reviewed, ranging from adversarial dual-encoder integration, adapter modules, and edge-aware CNN fusion to multi-stage detection-then-segmentation and 3D mesh extension pipelines. The most performant pipelines (Dice ∼0.90) integrate detection models (YOLO) for region localization, followed by SAM, then refined using UNet-based approaches.
Open-vocabulary detection (GroundingDINO) and contrastive alignment (CLIP) enable fine-grained abnormality detection and classification with competitive mAP and F1 scores. Robustness, however, remains contingent on prompt quality, annotation, and the fidelity of adaptation architecture.
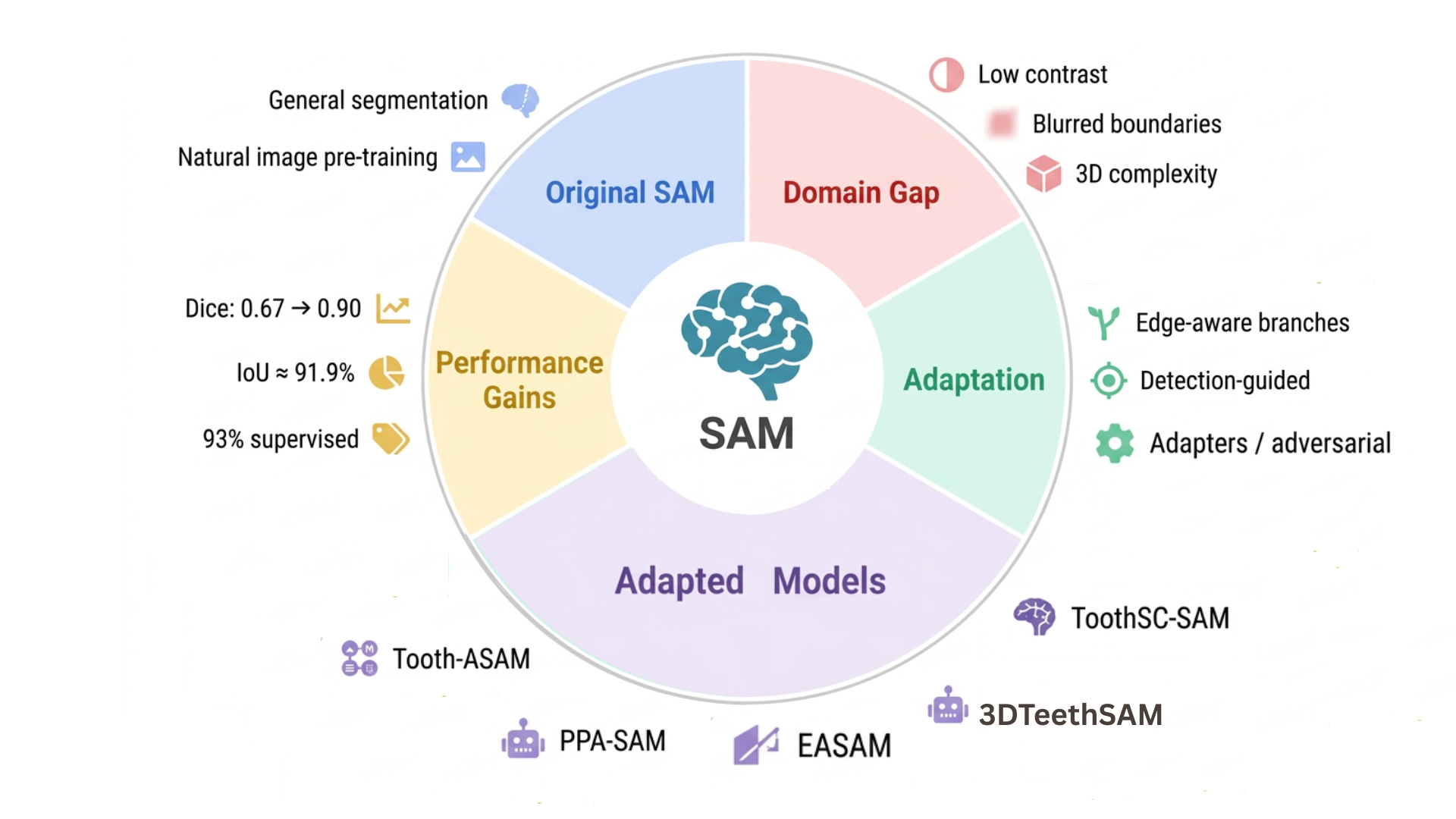
Figure 4: Overview of major SAM adaptation strategies for tooth and anatomical segmentation across dental imaging domains.
Dental-Specific Foundation Models: Full Specialization and Multimodal Integration
Pretrained-From-Scratch Models
DentVFM, trained via self-supervised objectives on 1.6M multimodal dental images, demonstrates label efficiency, robust cross-modality generalization, and, on select tasks, performance exceeding that of experienced dentists. This approach enables effective model scaling in data-dense vision tasks.
Heavily Fine-Tuned Multimodal Systems
Models such as DentVLM, OralGPT, and OralGPT-Omni combine large-scale instruction tuning with chain-of-thought datasets, reinforcement learning for clinical reasoning, and structurally agentic pipelines emulating iterative clinician workflows. DentVLM, for example, outperformed junior dentists on $21/36$ tasks and senior dentists on $12/36$—with diagnostic time reductions of 15-22%. OralGPT-Omni's explicit reasoning traces yield substantial gains over proprietary and generic VLMs.
Structured Pipelines and Agentic Architectures
Integration of deterministic knowledge-guided systems (ArchMap), validation agents for input QA (GumAgent), and retrieval-augmented LLMs (e.g., PerioGPT) illustrate the migration to structured, auditable, and multimodal pipelines, mitigating model-specific limitations.
Complementarity, Limitations, and Integration Imperative
A central, empirically validated conclusion is that model categories are complementary, not competing:
- LLMs: High performance in text reasoning, education, report generation.
- Vision Models: Superior in anatomical segmentation, disease detection, localization.
- Dental-Specific Models: State-of-the-art on complex, multimodal, and hybrid tasks.
The most effective clinical systems are integrated pipelines combining these model types, rather than relying on monolithic models.
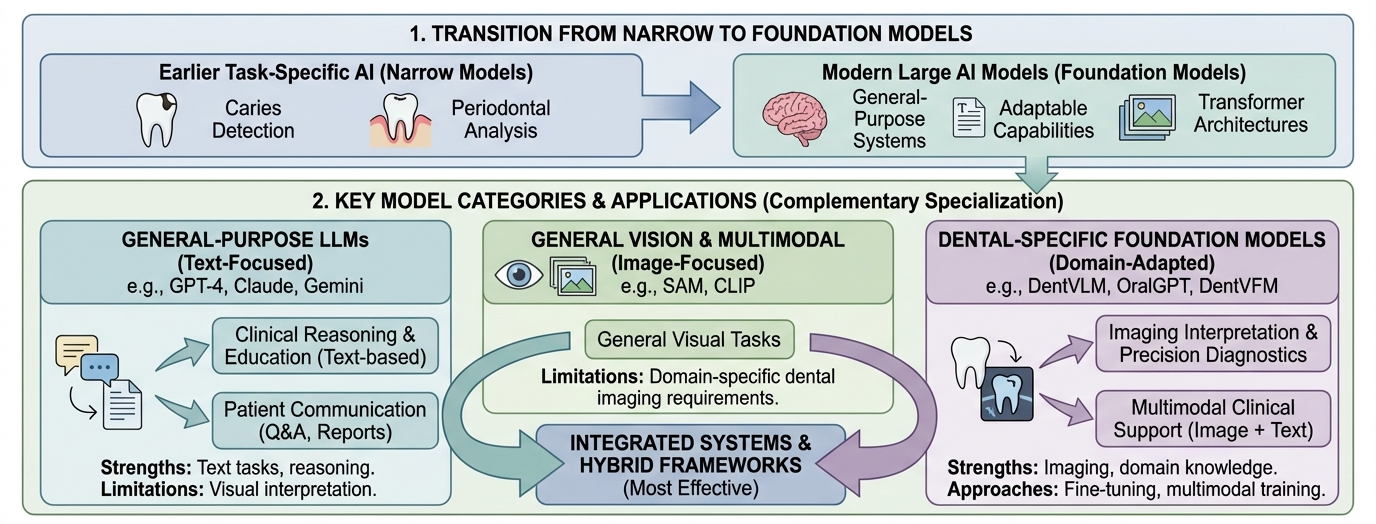
Figure 5: Transition schema illustrating narrow, single-task models giving way to multimodal, integrated foundation model ecosystems in dental healthcare.
Practical and Theoretical Implications
Key Clinical Implications
- Domain shift and data asymmetry necessitate dedicated adaptation strategies—generative models cannot fully replace vision pipelines for image analysis.
- Integrated, auditable systems offer superior clinician support and a clearer regulatory pathway, aligning with both FDA SaMD and EU AI Act standards.
- Data curation and benchmarking remain foundational infrastructure gaps; absence of shared, diverse annotated datasets and evaluation frameworks impedes cross-study and cross-model comparison.
Future Directions
- Agentic clinical reasoning architectures are poised to advance multimodal, stepwise diagnostic support.
- Label-efficient semi/self-supervised pretraining is crucial for sustainable model deployment in data-poor subspecialties.
- Knowledge-guided deterministic inference addresses explainability and control, essential for regulatory compliance and clinical trust.
Conclusion
The unified framework and systematic evaluation provided demonstrate that optimal dental AI deployment requires strategically integrated systems harnessing strengths from generative, vision, and domain-specialized models. Individual model optimization, absent robust integration and benchmarking infrastructure, is insufficient for clinically safe and generalizable deployment. Advances in agentic reasoning, annotation efficiency, and knowledge guidance represent promising directions, but their translational impact will be governed by progress in regulatory clarity, dataset development, and rigorous clinical validation. Until hallucination, annotation scarcity, and benchmarking heterogeneity are addressed, such systems must serve as supervised, assistive tools, augmenting—not supplanting—clinical expertise.

