- The paper demonstrates that TabPFN outperforms classical models in low-data regimes with higher AUC-ROC and superior calibration.
- It uses LOCO validation and subgroup fairness analysis to reveal significant cross-country heterogeneity in predictive performance.
- The study underscores the need for domain adaptation and context-sensitive modeling in resource-constrained global health settings.
Cross-Country Few-Shot Generalization in Tabular ML and Foundation Models for Childhood Anemia Prediction under Distribution Shift
Study Design and Context
The paper systematically investigates the predictive utility and generalization properties of classical ML models (Logistic Regression, XGBoost, LightGBM) and a transformer-based tabular foundation model (TabPFN v2.6) for childhood Anemia prediction using harmonized Demographic and Health Surveys (DHS) data from 16 countries across Africa, Asia, Latin America, the Caucasus, and the Middle East. The analytic sample comprises 68,856 children aged 6–59 months with altitude-adjusted hemoglobin measurements and standardized predictors spanning child, maternal, household socioeconomic, and geographic domains. Anemia is modeled as a binary outcome using WHO thresholds, and rigorous internal (stratified within-country cross-validation) and external (LOCO, reverse-LOCO) validation protocols are employed. Emphasis is placed on data-scarce regimes, subgroup fairness, model calibration, decision curve analysis, and robust interpretability leveraging SHAP and adapted in-context explanations for TabPFN.
The comparative few-shot learning investigation reveals pronounced advantages for TabPFN in settings with limited within-country labeled data. Below approximately 200 training samples, TabPFN delivers higher AUC-ROC than all classical baselines, with confidence intervals consistently non-overlapping at the lowest data regimes, demonstrating superior discrimination and robustness under strict sample scarcity (Figure 1).
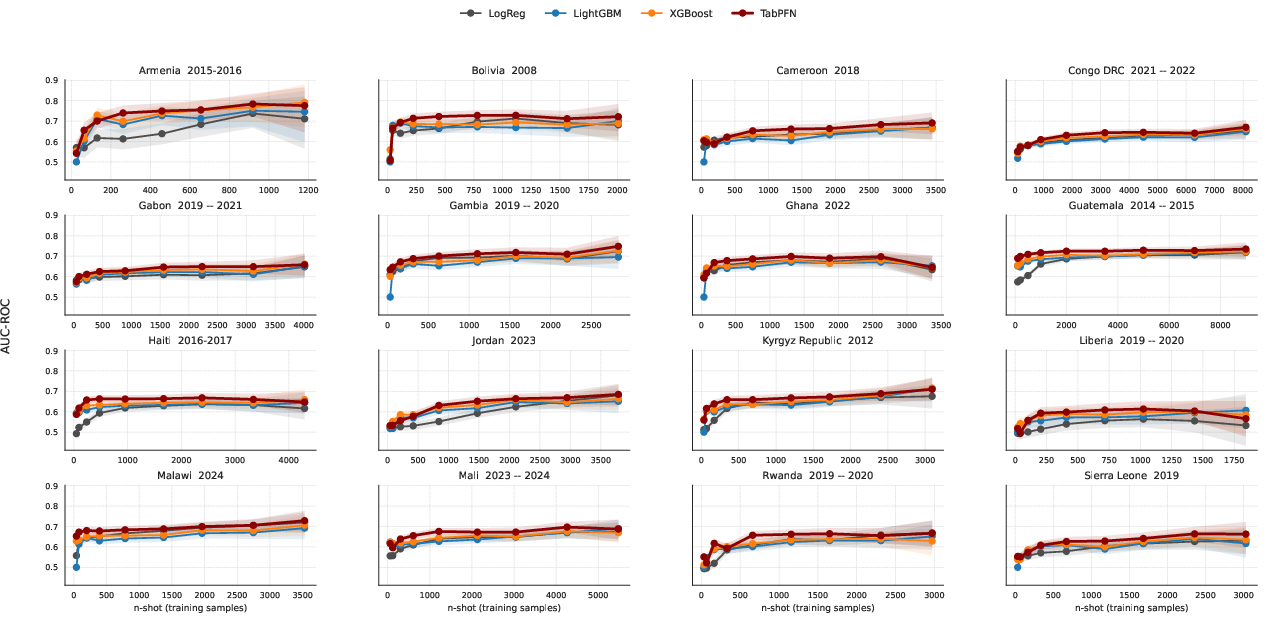
Figure 1: Few-shot AUC-ROC performance across countries and models as a function of within-country support set size.
As sample sizes increase, TabPFN’s performance converges with gradient-boosted models, but its low-data regime superiority is operationally critical, especially for deployment in resource-constrained surveillance contexts. Logistic regression exhibits the most pronounced sensitivity to sample size, whereas XGBoost and LightGBM recover performance at higher n-shot, reflecting the classical trade-off between model complexity and overfitting in small data scenarios.
Calibration Across Global Populations
Probabilistic calibration analysis demonstrates TabPFN's superiority, with the lowest mean Brier score (0.203) and Expected Calibration Error (ECE = 0.042) across all 16 countries (Figure 2). LightGBM and Logistic Regression display systematic miscalibration, particularly at higher predicted probabilities, while TabPFN exhibits consistent alignment between predicted and observed risk.
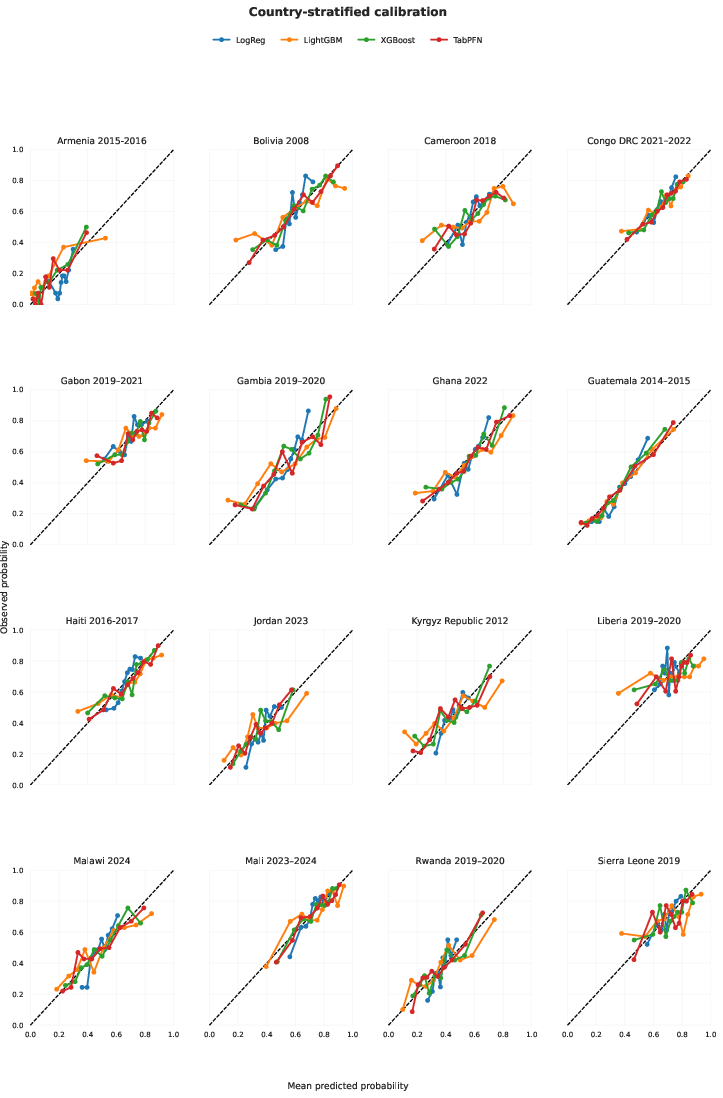
Figure 2: Calibration curves by country and model showing reliability of predicted risk estimates versus empirical Anemia frequency.
Model calibration is essential for decision-making in clinical and public health settings, as it governs the reliability of stratification thresholds and resource allocation.
Discrimination, Cross-Population Generalization, and Distributional Shift
Within-country discrimination is moderate across models, with AUC-ROC values ranging from 0.59–0.76 and substantially greater inter-country than inter-model variation. Highest performance is observed in Armenia and Guatemala, lowest in Liberia and Sierra Leone, indicating heterogeneity determined by population context rather than architectural choices (Figure 3).
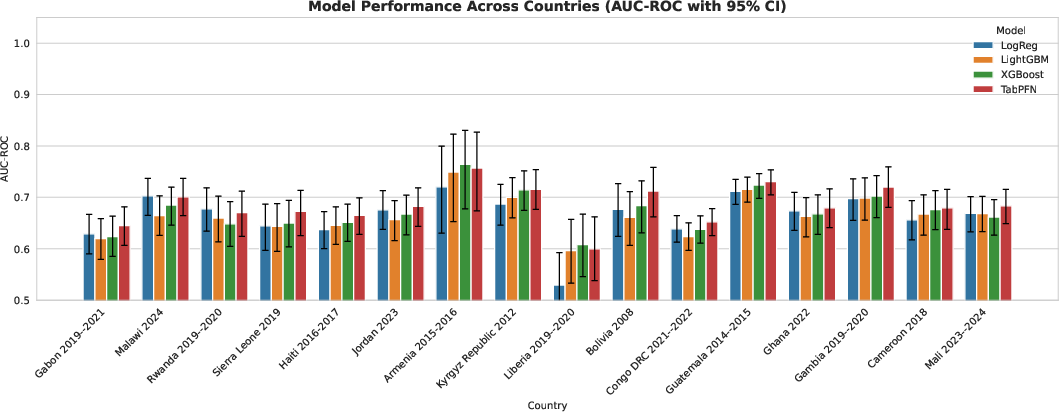
Figure 3: Within-country AUC-ROC with bootstrap confidence intervals for all models across 16 populations.
LOCO validation simulating external generalization performance reveals a consistent AUC-ROC decline (0.58–0.69), predominantly driven by target country identity and distributional shift rather than model selection (Figure 4). Reverse-LOCO analyses elucidate the asymmetric and directional transferability inherent in cross-country knowledge transfer: certain populations (e.g., Ghana, Guatemala, Haiti, Bolivia) serve as robust source domains, while others (Armenia, Liberia) remain difficult to predict regardless of training origin (Figure 5).
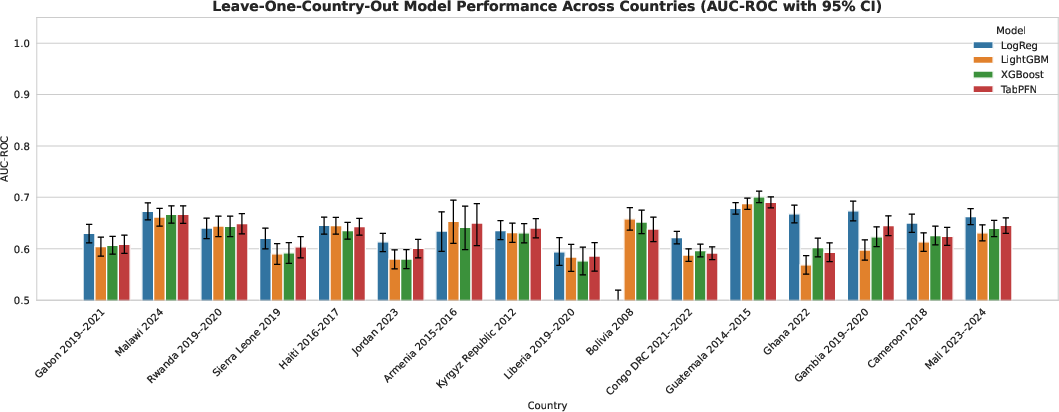
Figure 4: External AUC-ROC under LOCO validation highlights distributional shift across countries.
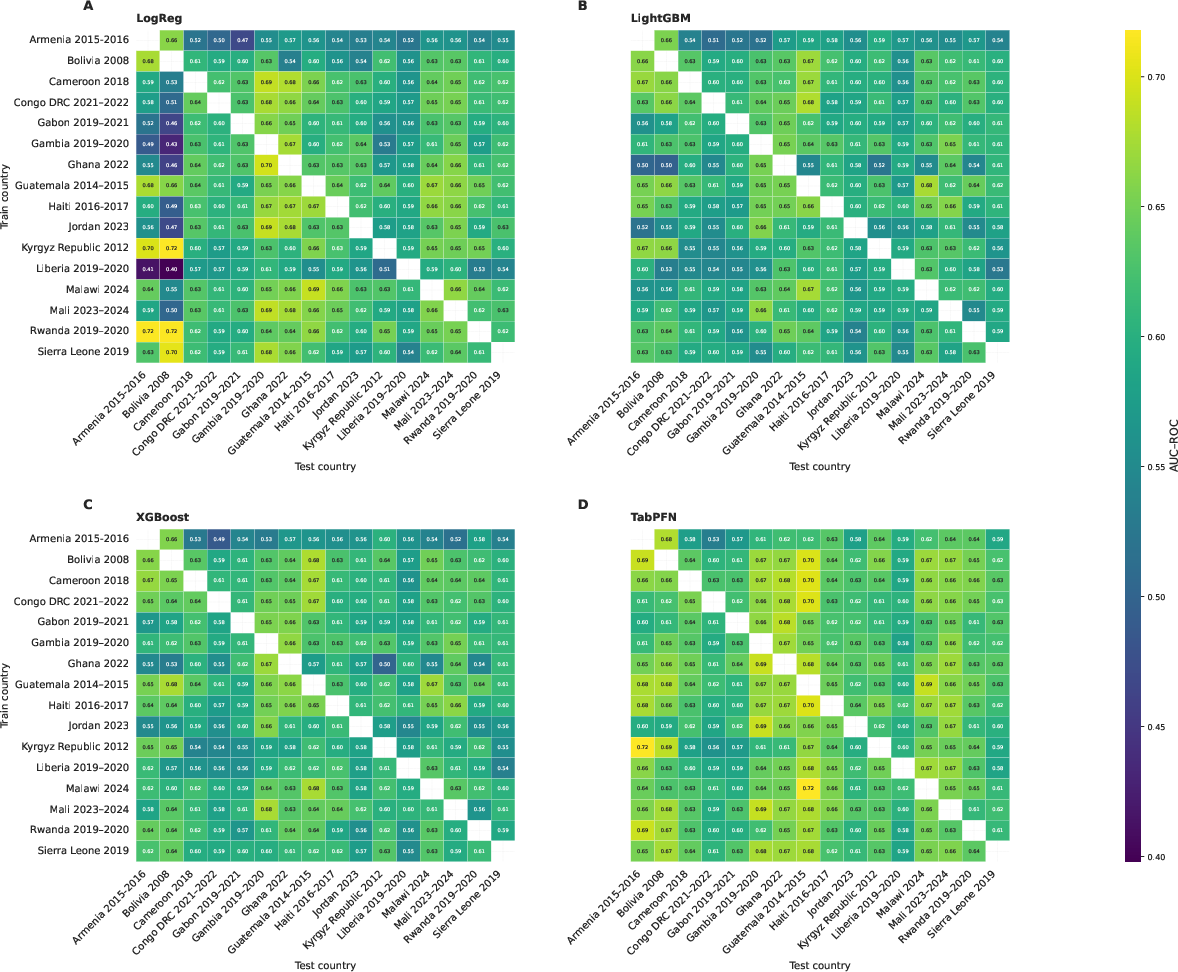
Figure 5: Reverse LOCO cross-country AUC-ROC visualized over all train-test pairs quantifies the asymmetric nature of transferability.
These findings underscore the limitations of naive data pooling and the necessity for explicit modeling of cross-population heterogeneity and epidemiological signal directionality.
Subgroup Fairness, Clinical Utility, and Feature Interpretability
Subgroup analysis confirms the absence of systematic bias across demographic strata within-country: child age, maternal education, residence, sex, and wealth quintile demonstrate broadly similar AUC-ROC across all models, though largest absolute variation occurs in country context and specific subgroup (Figure 6).
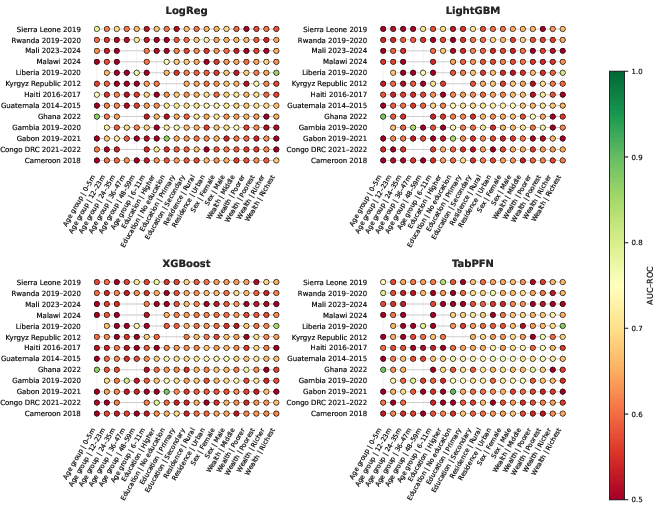
Figure 6: Subgroup AUC-ROC performance (leave-one-country-out) across models, with no consistent bias toward specific demographic strata.
Decision curve analyses demonstrate all models outperforming treat-none and treat-all reference strategies, with inter-model net benefit differences narrow and clinical utility governed largely by prevalence and context (Figure 7).
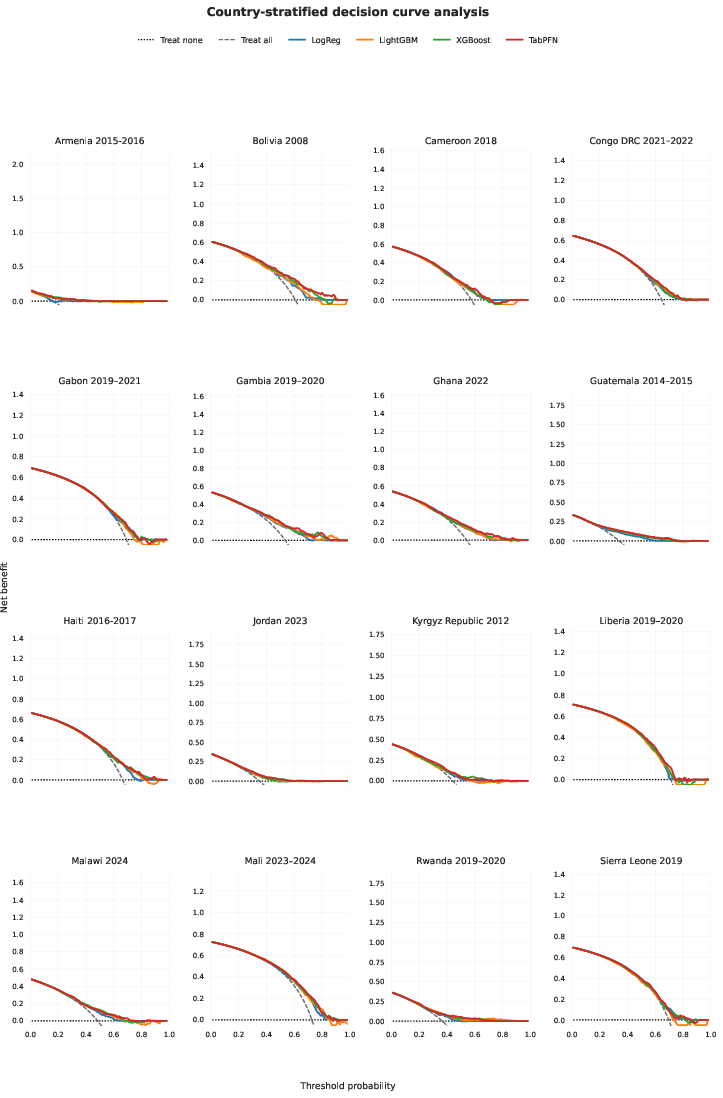
Figure 7: Net benefit versus threshold probability for anemia prediction, with all models providing positive clinical utility across countries.
Global SHAP importance rankings confirm child age as the dominant predictor, followed by altitude, height-for-age and weight-for-age z-scores, wealth index, and maternal education across all models (Figure 8). TabPFN feature attributions are consistent with classical approaches, reinforcing epidemiological validity; detailed country-level importance reveals altitude and anthropometric z-score effects are contextually determined by geography and sample heterogeneity (Figure 9).
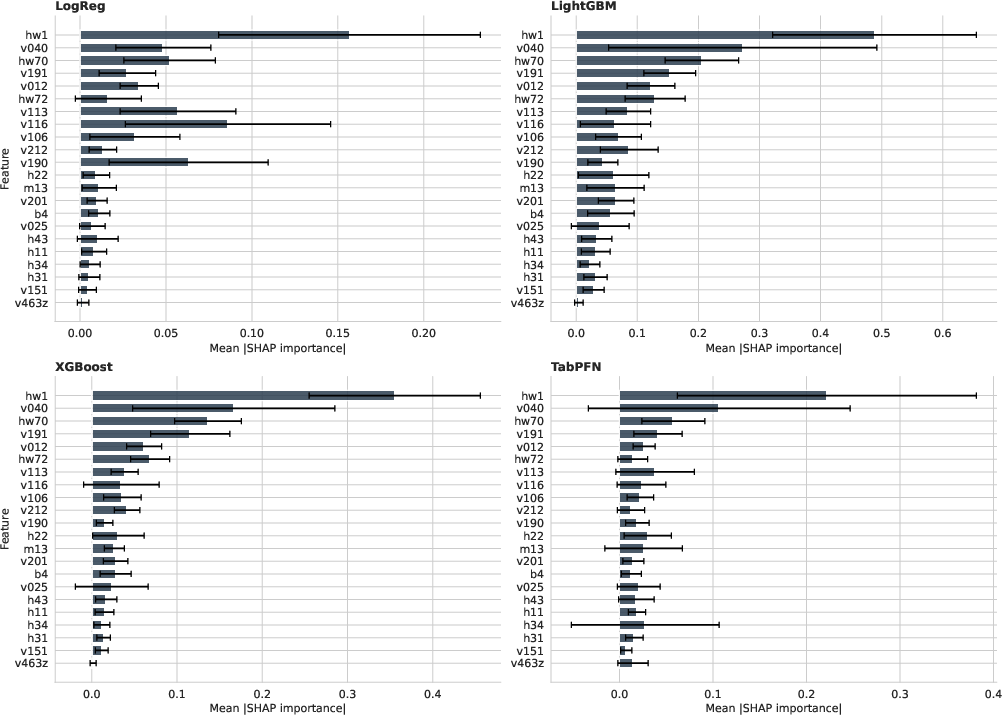
Figure 8: Aggregated SHAP feature importance with error bars for all models identifying consistent predictor hierarchies.
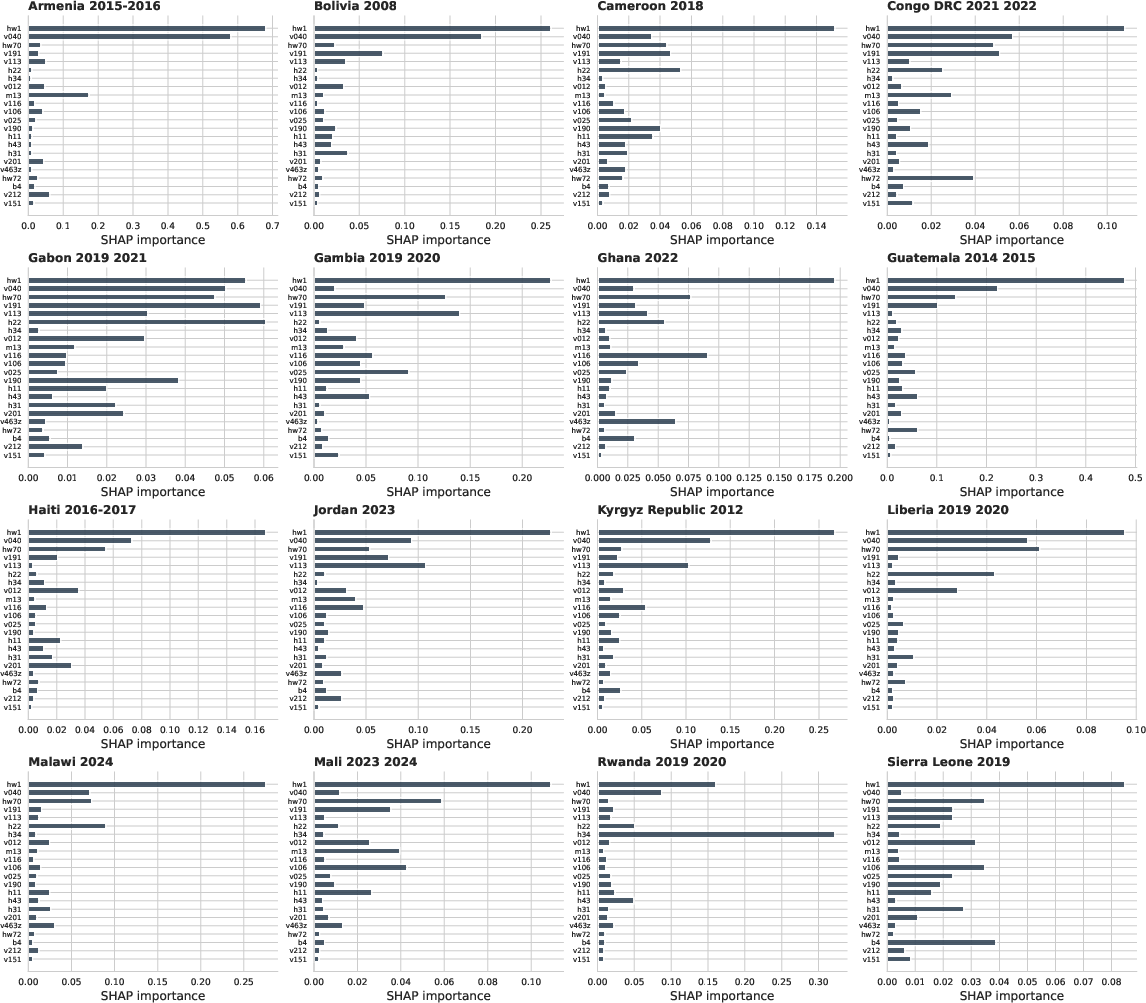
Figure 9: TabPFN within-country feature importance profiles illustrate heterogeneity in predictor impact across settings.
Practical and Theoretical Implications
The principal operational implication is TabPFN’s robust performance under extreme data scarcity, crucial for deployment in low-resource surveillance environments. Its calibration advantage translates to improved risk stratification and actionable screening, especially where labeled data acquisition is costly or infeasible. The dominance of cross-population heterogeneity over model effects underscores the practical need for domain adaptation, transfer learning, and multimodal approaches tailored to local epidemiologies.
Theoretical implications center on the non-uniform, asymmetric transferability of epidemiological knowledge across populations—highlighting the fundamental challenge of modeling distribution shift and structural variation in global health prediction. The foundation model paradigm (TabPFN) demonstrates implicit regularization and background knowledge utilization but faces challenges in interpretability, infrastructure dependence, and adaptation to evolving epidemiological profiles. Subgroup and decision curve analyses validate fairness and clinical utility, but sustained improvements depend on enhancements in local data curation, survey representativeness, and causal feature integration.
Future Directions in AI for Global Health
Future work should address methodological extensions including context-aware domain adaptation, explicit modeling of transfer directionality, integration of geospatial and environmental predictors, and development of interpretable foundation models mapping latent representations to causal epidemiological mechanisms. Regulatory and ethical constraints, especially pertaining to AI sovereignty and local adaptation, will require scalable infrastructure and transparent calibration pipelines.
Advances in self-supervised, multimodal, and causal representation learning for tabular clinical data are poised to improve transportability and generalization. Sustained interdisciplinary collaboration and investment in local data infrastructure remain essential for practical deployment.
Conclusion
The comparative evaluation demonstrates that, for childhood Anemia prediction, population heterogeneity and data characteristics set a more stringent constraint on predictive performance than model architecture. TabPFN, as a tabular foundation model, confers meaningful discrimination and calibration advantages in data-scarce regimes, supporting its suitability for low-resource settings. However, significant performance variability across countries and persistent constraints on transferability highlight the operational necessity of context-sensitive modeling, domain adaptation, and multimodal integration. These findings inform future methodological and practical priorities for deploying robust, reliable AI systems in global health surveillance and risk stratification.

