- The paper demonstrates that high-fidelity synthetic data generated by latent diffusion models can achieve statistically equivalent performance to real data in predicting childhood vaccine uptake.
- It employs Logistic Regression and XGBoost classifiers, achieving >90% precision, recall, and F1-scores for early-cycle vaccines even when using synthetic or hybrid data approaches.
- The study underlines the potential for scalable, privacy-preserving ML pipelines in low-resource settings, addressing equity challenges in vaccination coverage.
Machine Learning and Synthetic Data for Vaccination Prediction in Narok, Kenya
Introduction and Motivation
Equitable childhood vaccine coverage remains a major challenge in low- and middle-income countries due to geographic, socioeconomic, and infrastructure barriers, particularly among nomadic and rural populations. In Kenya's Narok County—home to the Maasai—missing, inconsistent, and non-digitized data further hinder timely and targeted immunization interventions. Existing electronic health record (EHR) adoption is minimal, and data privacy concerns are pronounced due to the vulnerability and identifiability of population subgroups.
This paper addresses two interlinked objectives: (1) predicting childhood vaccination outcomes using classical and ensemble machine learning classifiers, and (2) preserving patient privacy and facilitating data scalability through synthetic dataset generation with state-of-the-art diffusion-based models.
Data Collection and Preprocessing
Eight years of childhood vaccination records were digitized from the MOH 510 registry, capturing 6,913 individuals after rigorous data cleaning and filtering. Preprocessing addressed categorical feature outliers, continuous variable mislabeling, and strong collinearity (notably between village, latitude, and longitude). Missing, inconsistent, or underrepresented categorical data led to exclusion, ensuring that synthetic data generation and model training phases operated on a stable, representative distribution.
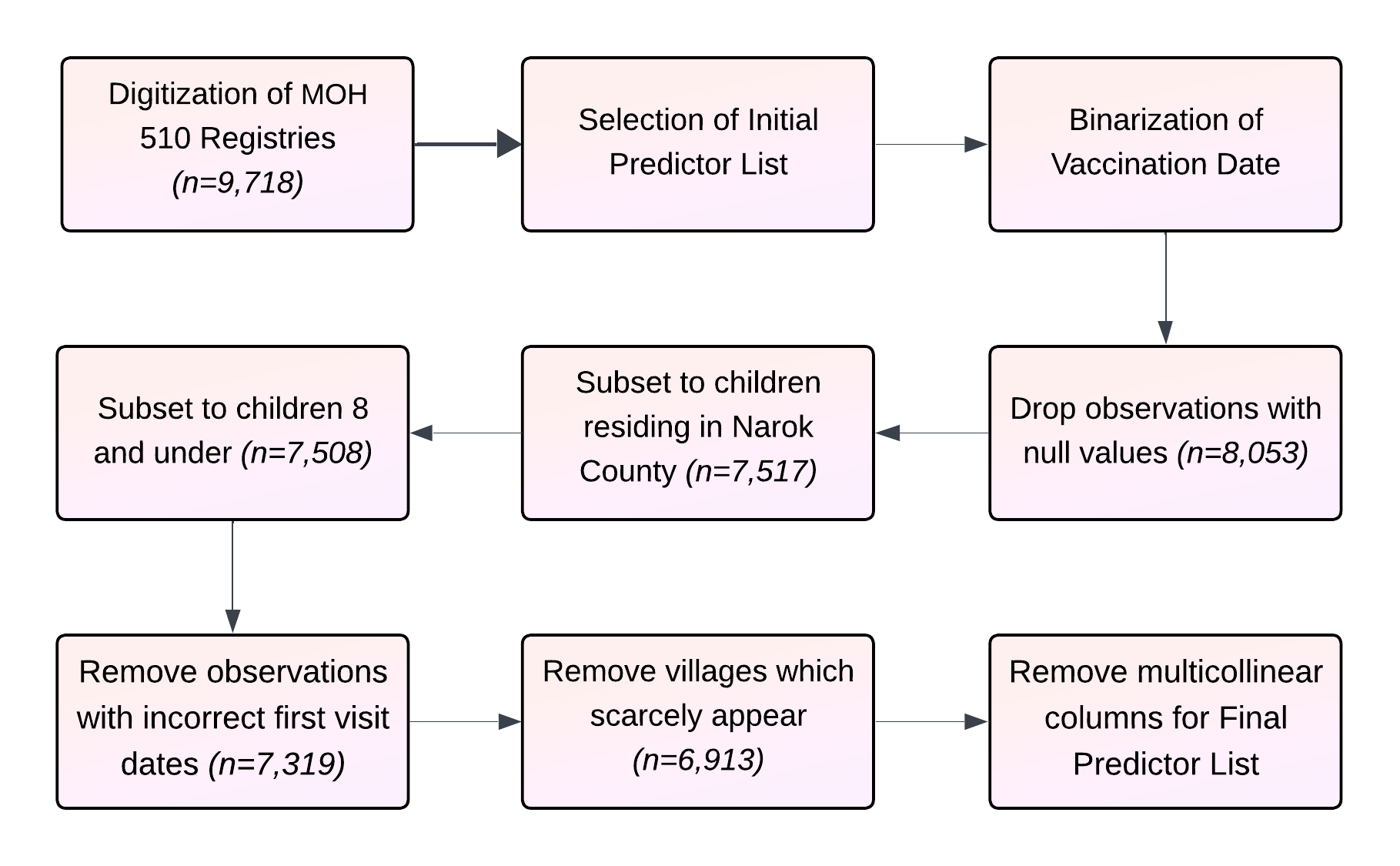
Figure 1: Data Preprocessing Steps highlighting the exclusion of outlier geographic values, correction of inconsistent numerical features, and preparation for robust model training and synthesis.
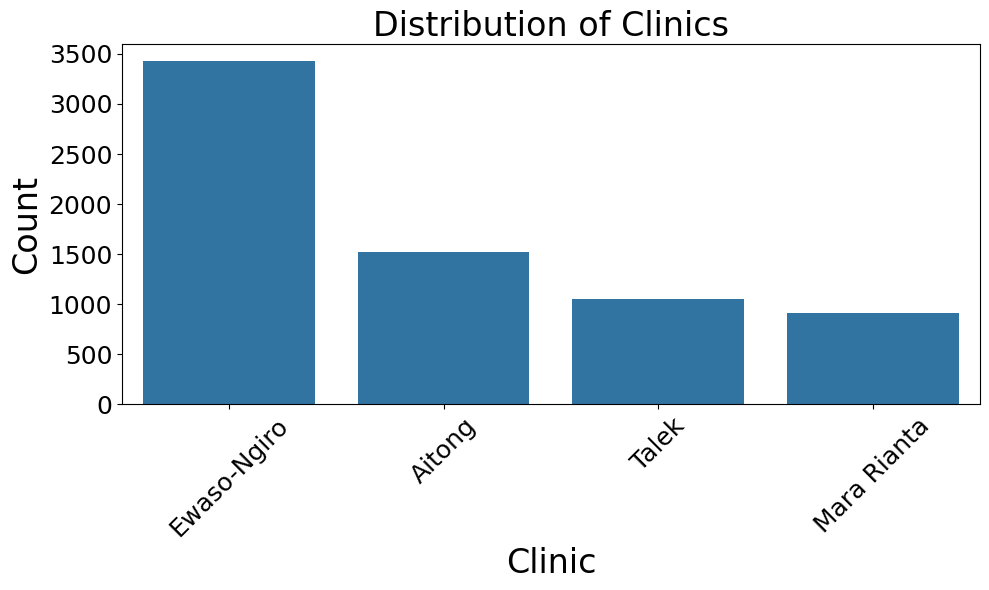
Figure 2: Number of Individuals Within Each Clinic Registry, revealing regional heterogeneity in the dataset’s clinic distributions.
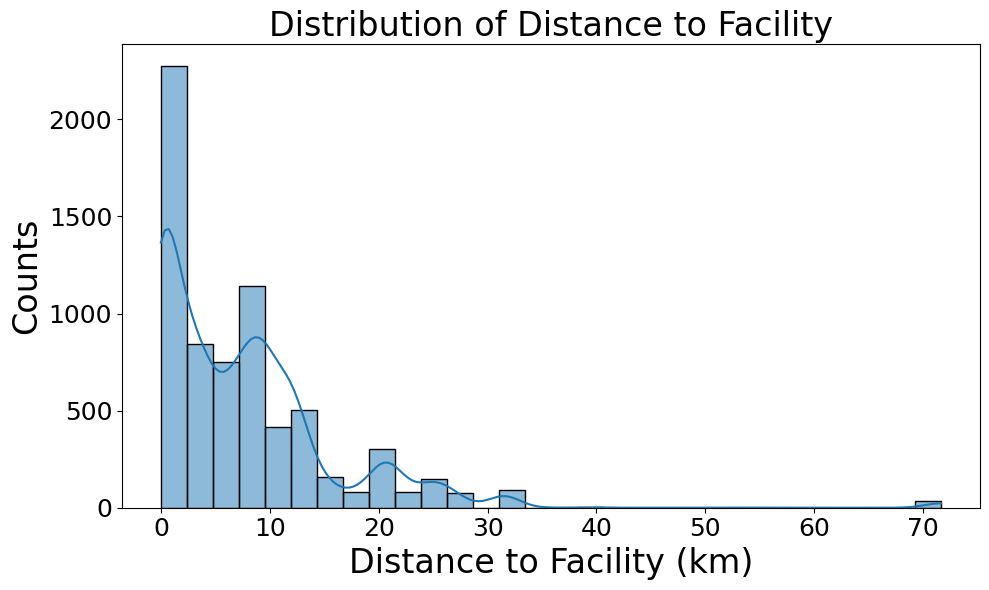
Figure 3: Distances Traveled by Individuals to the Nearest Health Facility, showing substantial travel for a notable subset of the cohort.
Coverage rates are highly variable across the 17 recorded vaccines, with high uptake for early-schedule antigens (e.g., 95.6% for BCG) and severe attrition for late-stage vaccines (e.g., 13.7% for MR2), indicating equity and adherence gaps that predictive models aim to help address.
Predictive Modeling Approach
Two machine learning classifiers—Logistic Regression and XGBoost—were deployed to predict vaccine uptake for each antigen, using a standard 80/20 train-test split. To assess privacy-preserved modeling, the TabSyn latent diffusion-based synthetic data generator was trained on the real data. Three training regimens were considered per antigen: (1) real data only, (2) synthetic data only, and (3) a hybrid of real and synthetic data. Synthetic Minority Oversampling Technique (SMOTE) was optionally applied to mitigate class imbalance.
The TabSyn pipeline leverages a VAE to map mixed-type tabular records to a continuous latent space, making them tractable for diffusion-based modeling. Multiple samples of synthetic datasets were evaluated to assess consistency and fidelity.
Evaluation Metrics and Analysis
For predictive tasks, class-balanced precision, recall, and F1-scores were used due to marked outcome imbalance. For generative fidelity, distributional similarity (via Kolmogorov–Smirnov and Total Variation Distance), as well as feature+pairwise correlation preservation, quantified the statistical fidelity of synthetic data to the real distribution.
Column-wise density and correlation metrics were >0.95 for all categorical and several continuous features, demonstrating high-fidelity synthesis. Minor drops were observed for certain pairs involving continuous age features.
Key Results
The predictive models trained on either real or synthetic data produced statistically equivalent performance for most vaccines, with F1, precision, and recall commonly exceeding 90% for early-cycle antigens. Inclusion of synthetic data resulted in no significant loss of performance and modest gains in some late-cycle vaccine targets.
Feature importance analysis identified "first visit day," "age," and "gender" as the dominant predictors in both real and synthetic XGBoost models, reaffirming biological and operational relevance.
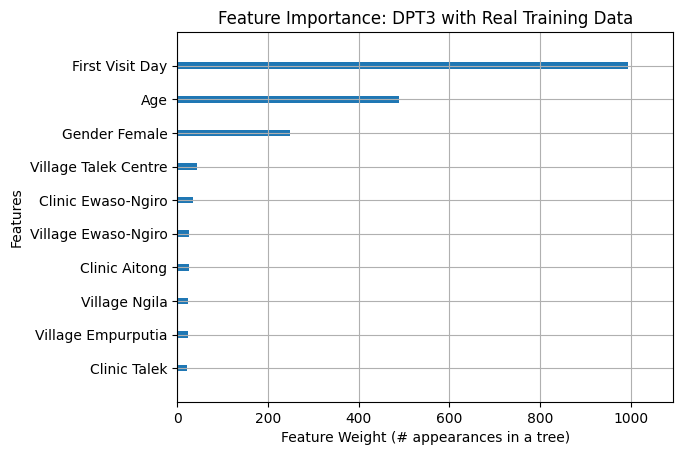
Figure 4: Feature Importance Analysis—DPT3 Real Data. "First Visit Day," "Age," and "Gender" emerge as the principal determinants in real-data models.
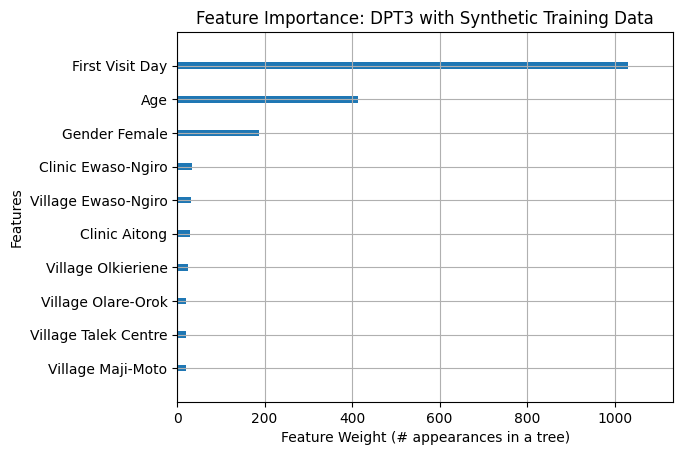
Figure 5: Feature Importance Analysis—DPT3 Synthetic Data. Synthetic-data-trained models identify equivalent feature importance profiles, confirming consistency.
Strong evidence supports both the viability of ML-based vaccine prediction in low-resource, heterogeneous environments and the use of synthetic data to fully substitute real data for downstream predictive modeling, with >95% distributional fidelity and negligible privacy risk.
Practical and Theoretical Implications
The deployment of synthetic data for ML-based vaccine forecasting demonstrates tangible benefit for privacy preservation in resource-constrained populations with high re-identifiability risk. By facilitating digital health analytics in the absence of robust EHR infrastructure—or with unscalable manual digitization—this approach supports rapid, scalable, and privacy-compliant modeling. The ability to locally train generative models on modest hardware further enables sustainable integration into line health operations.
From a methodological perspective, the findings empirically validate the recent advances in latent-space diffusion models for structured healthcare data, extending their utility beyond prior applications focused primarily on EHR and time-series synthesis. This will likely incentivize further research into context-specific data generation, privacy assurance, and the operationalization of ML toolchains in LMICs.
Limitations and Future Directions
Sample limitations reflect catchment bias—missed cases outside the clinic network and potential inaccuracies in historical digitization. Improving EHR roll-out, integrating mobile outreach data, and joint modeling of adherence pathways are needed for future work. Architecturally, enhancements to continuous feature modeling in synthetic data, as well as the integration of explainable AI components for clinical acceptability, are warranted.
Advancing practical deployment will require the development of user-friendly digital interfaces for health workers, ongoing validation of data-generation privacy guarantees, and regulatory alignment with evolving data protection acts.
Conclusion
This study demonstrates the joint utility of machine learning and generative synthetic data for predicting childhood vaccination outcomes in resource-limited, high-risk communities. Synthetic data can substitute for real records in supervised learning pipelines without compromising equity, accuracy, or privacy, thereby enabling scalable, actionable, and private health informatics in under-digitized settings.
The results decisively support the use of diffusion-model-based tabular synthetic data for privacy-preserving forecasting in public health operations. Future developments will likely coalesce around automated, interpretable, and privacy-assured ML systems for equitable vaccine distribution and broader health resource optimization.