- The paper introduces CDTI, a novel observational study design that uses clinician evaluations to reveal unobserved confounders affecting treatment effect estimation.
- It employs three matching strategies—Z-matching, π-matching, and Z-dominance—with theoretical guarantees based on stochastic dominance and log-supermodularity assumptions.
- Experimental evaluations on synthetic, semi-synthetic, and real ICU data validate the framework's ability to improve causal inference by accounting for latent biases.
Confounder Detection via Treatment Intent: An Observational Study Design for Eliciting Unobserved Covariates
Motivation and Theoretical Foundations
The paper introduces Confounder Detection via Treatment Intent (CDTI), a novel observational study design targeting the identification of unmeasured confounders in causal inference tasks using observational data (2605.26413). The problematic nature of unobserved confounding is rigorously addressed: in practical domains (e.g., critical care medicine), observational estimates of treatment effects are well-known to be vulnerable to systematic bias when not all relevant covariates are observed. Standard back-door adjustment is rendered invalid in the presence of such latent confounders, and empirically, ICU datasets produce strongly positive estimated effects of mechanical ventilation on mortality—in contradiction to expert clinical expectations, indicating substantial unmeasured confounding.
The CDTI framework is predicated on the insight that treatment decisions are informed by variables accessible to clinicians but absent from the recorded data. By querying clinicians to compare pairs of patients (matched or dominated by observed variables), the approach aims to elicit explanations—ideally revealing unobserved causes—that drove the differences in treatment assignment.
The methodology is formalized as a two-part design: a matching strategy (M) proposing treated-control patient pairs for comparison, and an extraction strategy (E) modeling how clinicians articulate the factors underpinning their decisions. Three concrete matching strategies are developed: Z-matching (exact match on observed covariates), π-matching (match on estimated propensity scores), and Z-dominance (pairs where the treated unit is no sicker than control on observables).
Stochastic Dominance Framework and Theoretical Guarantees
Central theoretical results delineate conditions under which the matching strategies yield pair distributions informative about genuine unobserved confounders. The main theorem establishes stochastic dominance relationships for matched pairs: under monotonicity and log-supermodularity assumptions governing the treatment assignment mechanism and latent variable dependence structure, the distribution of unobserved confounders in treated units is stochastically larger than in controls, conditional on matched observed covariates or propensity scores.
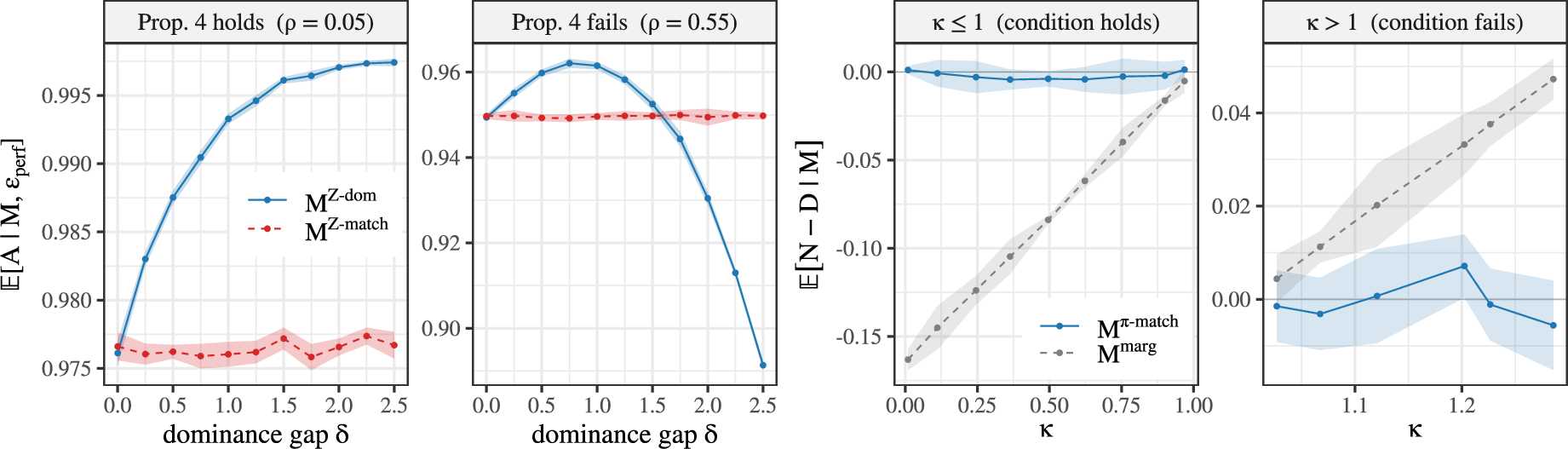
Figure 1: Synthetic verification of stochastic dominance assertions, comparing Z-dominance and Z-matching across varying dominance gap δ and correlation regimes.
Analytical argument is provided for both univariate and multivariate settings, relying on monotone likelihood ratios and established orderings (Karlin-Rinott). Log-supermodularity is required for multivariate extension, ensuring coordinatewise dominance across dimensions of latent confounders. Sufficient conditions are dissected in detail, including their operationalization for real-world ICU data.
Additionally, the paper establishes theoretical dominance between the matching strategies themselves: Z-dominance provably increases the probability of eliciting unobserved confounders versus Z-matching under perfect extraction, and E0-matching (propensity-based) outperforms randomly selected pairs when observed variation explains substantially more treatment assignment than latent variation. All dominance relationships are rigorously substantiated with formal proofs.
Extraction and Selection Model
The extraction model formalizes the process by which the human annotator (clinician) articulates candidate explanations driving treatment. Under perfect extraction, the annotator identifies all variables (observed and unobserved) along which the treated patient exceeds the control. A selection model is defined: the probability that the annotator selects a genuine, unobserved confounder among all available is computed explicitly, and the matching strategies are compared by their expected ratio of latent to observed competitors. This analytical rubric provides a concrete foundation for quantifying the success rates of confounder detection—grounded in the structure of the underlying data and the extraction/selection procedure.
Experimental Evaluation
Empirical validation spans synthetic, semi-synthetic, and real clinical data domains.
Synthetic and Semi-Synthetic Data
The synthetic experiments utilize multivariate Gaussian latent structures with varying degrees of E1-E2 correlation and propensity parameterization, allowing direct control of theoretical assumptions. Synthetic verification confirms the theoretical predictions: E3-dominance surpasses E4-matching as the dominance gap E5 increases under mild E6-E7 correlation, but fails when correlation is strong—validating the necessity of log-supermodularity. For propensity-based matching, dominance is observed precisely as predicted by the marginal AUC threshold.
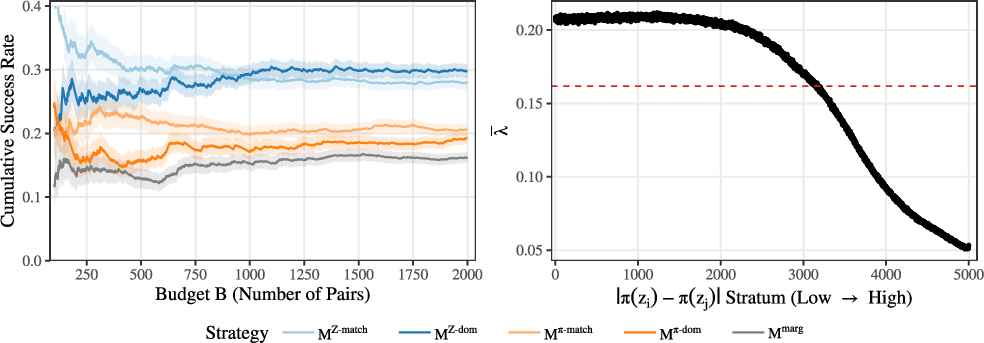
Figure 2: Semi-synthetic results on MIMIC-III show cumulative success rate versus budget, supporting superiority of E8-dominance and E9-matching strategies in successful confounder detection.
The semi-synthetic construction injects extracted UMLS entities (via robust biomedical NLP) as binary latent confounders into MIMIC-III data and samples treatment/outcome using a fitted logistic model. Success rates of confounder elicitation are tracked for each matching strategy; Z0-dominance and Z1-matching consistently outperform propensity and random matching, with empirical stratification by propensity gap further confirming success probability decay with increasing mismatch.
Real ICU Data: Mechanical Ventilation
Application to real MIMIC-III EHR yields top detected candidate confounders associated with mechanical ventilation, including direct pulmonary injury, SIRS-related infection, hemorrhage/trauma, cardiac comorbidity, and non-specific severity markers. Most elicited confounders are clinically plausible (17 of 20)—validating the capacity of the framework to recover meaningful unmeasured variables.
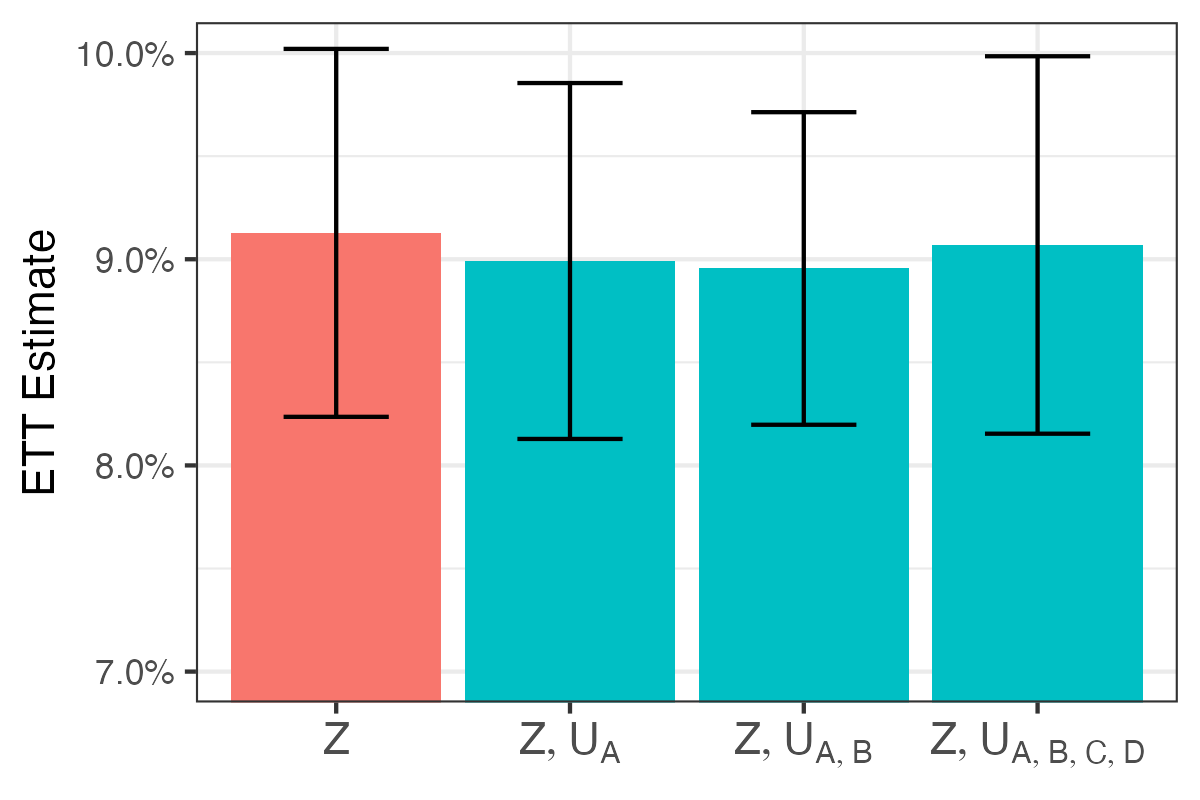
Figure 3: Top 20 discovered confounders (frequency-ranked) in real ICU data via ablation-based extraction and ETT estimates for various adjustment sets using causal forests with bootstrap CIs.
ETT re-estimation with adjusted sets incorporating detected confounders shows slight reduction when pulmonary and infection-related variables are included, but overall effect estimates remain substantially nonzero and statistically indistinguishable. This highlights the inherent limitations of EHR text proxies in capturing true latent covariates—binary indicators constructed from retrospective textual documentation are noisy, underscoring the need for improved measurement or extraction fidelity.
Limitations and Implications
Several limitations are acknowledged. Log-supermodularity imposes strong constraints on latent confounder dependence; relaxing to marginal dominance is suggested as a future direction. The extraction model assumes uniform selection and explicit articulation by clinicians—real-world annotation may not conform. Retrospective EHR notes only partially capture relevant factors, and framework cannot certify detected variables as confounders nor restore back-door validity.
Practically, CDTI provides a methodologically sound, actionable protocol for analytically eliciting candidate unobserved confounders without resorting to costly experimental interventions or relying solely on prior domain enumeration. Theoretically, it clarifies the structural requirements for successful causal identification in the presence of latent bias and opens avenues for systematic, human-in-the-loop causal analysis.
Conclusion
The presented framework introduces a principled observational study design for systematic confounder detection with theoretical guarantees on elicitation success under interpretable assumptions. Empirical results validate theoretical predictions and show practical success in both synthetic and real-world ICU settings. The approach highlights the tension between structural assumptions and extractive fidelity in causal inference, offers a valuable tool for improving the reliability of observational effect estimation, and sets the stage for future refinements in both statistical theory and clinical measurement.

