- The paper proposes a cost-sensitive Global Risk metric that penalizes false negatives more heavily to better reflect clinical diagnostic safety.
- It rigorously evaluates robust training methods including UNICON+CS, Co-teaching, DivideMix, and GMM filtering under varying label noise conditions on DermaMNIST and PathMNIST.
- The results emphasize that high balanced accuracy may still entail unacceptable clinical risk, underscoring the need for risk-based evaluation in medical AI.
Risk-Aware Robust Learning under Label Noise in Medical Image Classification
Introduction
The challenge of label noise in medical image classification remains a significant reliability bottleneck for deploying deep learning systems in diagnostic applications. Annotation errors resulting from inter-observer variability and case ambiguity systematically introduce incorrect labels, which deep neural networks are prone to memorize, leading to serious misclassification risks. The cost asymmetry between false negatives (FN) and false positives (FP)—delayed disease detection versus unnecessary follow-ups—renders accuracy-oriented metrics insufficient for safety-critical deployment. This paper proposes a comprehensive clinical risk analysis of state-of-the-art (SOTA) noise-robust training methods, integrating a cost-sensitive Global Risk metric that penalizes false negatives commensurately, with particular focus on robust learning under varying label noise conditions.
The authors employ DermaMNIST (skin lesion) and PathMNIST (colorectal pathology) datasets in their binary forms (malignant vs. benign), mirroring clinically meaningful screening scenarios. Label noise rates of 0%, 20%, and 40% are artificially introduced during training; test and validation splits remain clean. The evaluation eschews aggregate accuracy in favor of a risk metric defined as:
Risk=NCFN⋅FN+CFP⋅FP
where CFN and CFP delineate the clinical costs—set to CFN=20, CFP=1 in their primary scenario (Risk II), thereby strongly penalizing missed malignant cases. This risk-based assessment is performed in parallel with classical metrics such as Balanced Accuracy (BAC), Sensitivity, and Specificity, to enable nuanced tradeoff analysis.
Approaches: Robust Training and Cost Sensitivity
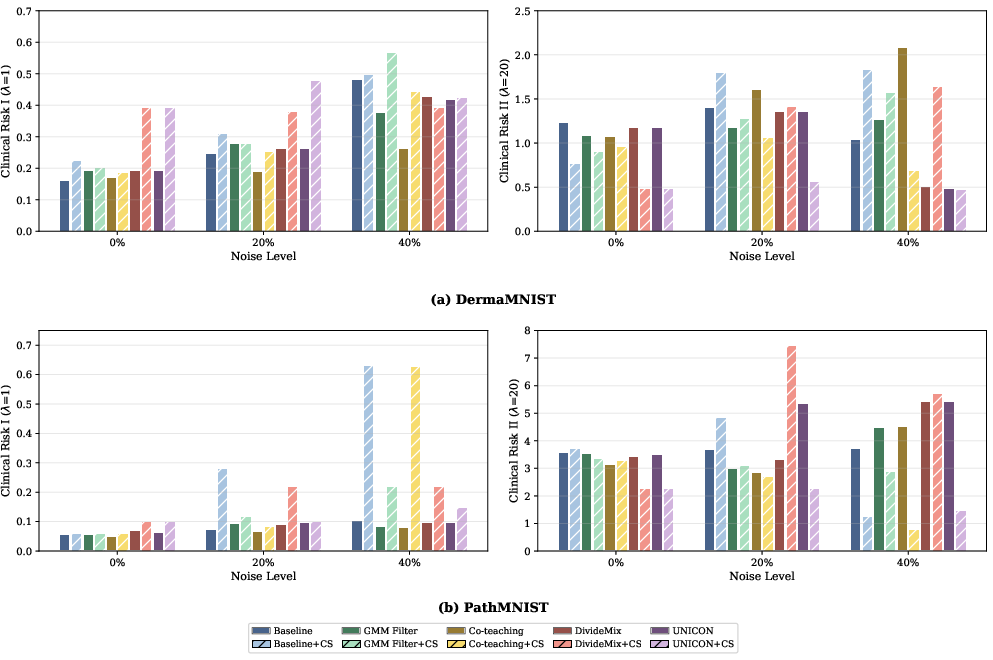
Four robust learning algorithms—Co-teaching, DivideMix, UNICON, and a GMM-based filtering method—are evaluated against a cross-entropy baseline. Each is also paired with a cost-sensitive (CS) variant, implemented via class-weighted loss. Notably, UNICON augments uniform selection and contrastive learning, potentially providing more resilience for minority (malignant) class preservation under label noise. The cost sensitivity is designed to directly optimize for minimization of FN, correcting for the clinical risk asymmetry ignored by conventional loss formulations.
Empirical Evaluation: Clinical Risk under Noise
Systematic experiments quantify the interplay between label noise, robust training, and clinical risk. A pivotal observation is that increasing label noise destabilizes both BAC and risk metrics, but in dataset-dependent patterns. On DermaMNIST at 40% noise, the baseline model collapses to near-universal positive predictions, sharply reducing FN but inflating FP. This results in an artificial decrease of Risk II, while diagnostic utility is actually undermined—a degeneracy only visible when analyzing the error decomposition beyond aggregate risk.
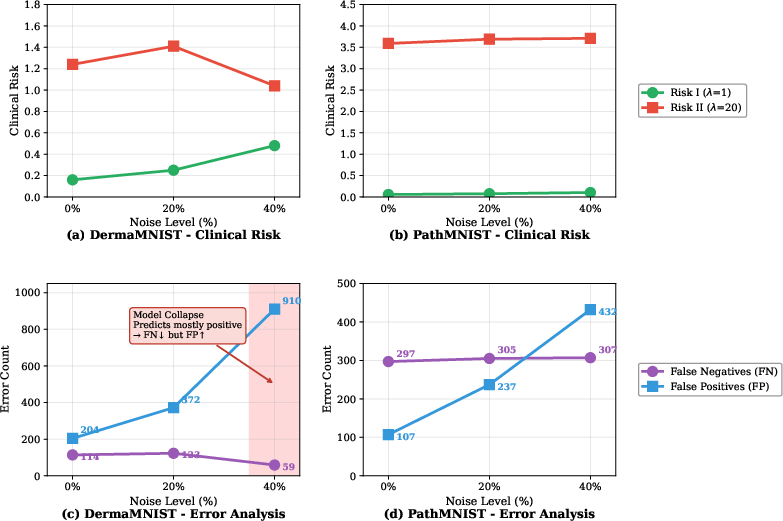
Figure 1: Impact of label noise on the Baseline model; note the non-monotonic changes in Risk I and Risk II and the collapse in FN/FP balance at high noise.
Comparative results indicate that:
Tradeoff Analysis: Accuracy vs. Asymmetric Risk
Tradeoff plots of BAC against clinical risk (Risk I and II) underscore that optimal accuracy does not guarantee clinical safety under high noise. In particular, models may exhibit high BAC but unacceptable Risk II (i.e., excessive FNs), directly contravening clinical objectives. The top-left region (high BAC, low Risk) is only reached by select method/cost combinations, reinforcing the argument for joint optimization.
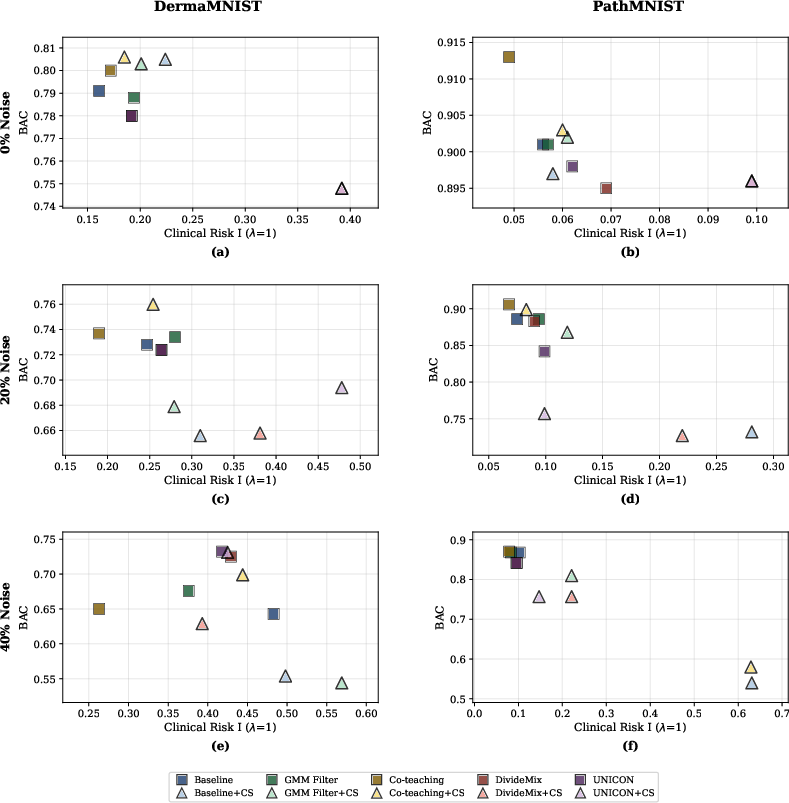
Figure 3: BAC vs. Clinical Risk I. Optimal models reside in the upper-left quadrant.
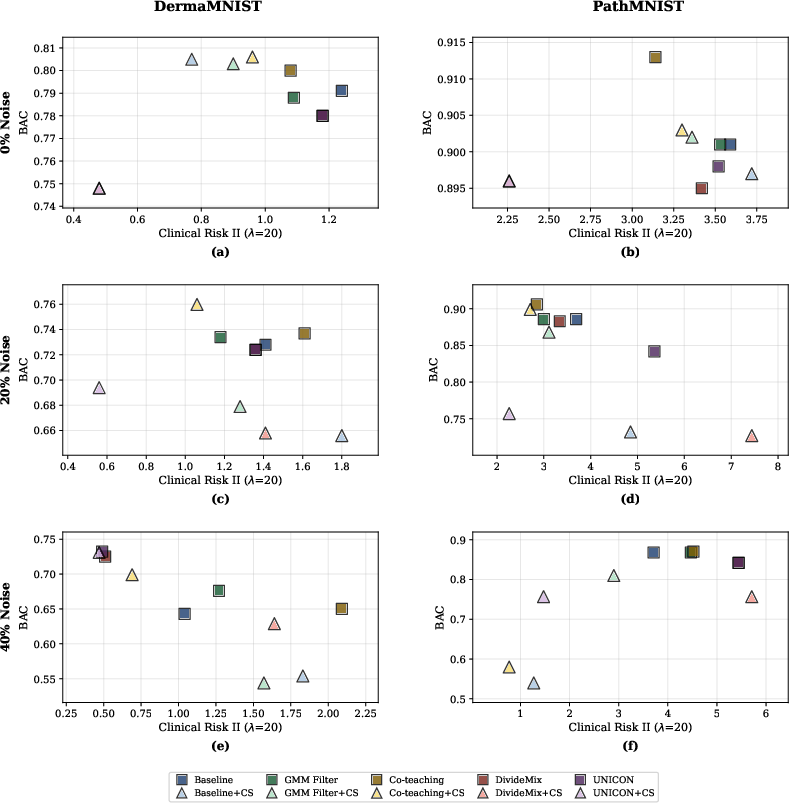
Figure 4: BAC vs. Clinical Risk II. UNICON+CS situates closest to the optimal regime with low risk and sufficient BAC.
Methodological Implications and Theoretical Considerations
The findings reveal that robust learning and risk minimization are distinct and sometimes orthogonal: methods that maximize accuracy or resist noise do not necessarily minimize clinical risk due to asymmetric error costs. Effective risk reduction via cost-sensitive loss requires compatible robust learning mechanisms, notably those that ensure positive class retention under severe label corruption. Uniform class-aware sampling, as in UNICON, emerges as a key enabler.
A further implication is that risk-based metrics should be primary evaluation endpoints for medical AI development pipelines, with post hoc accuracy analyses providing secondary interpretability. Trivial strategies that minimize FN by predicting positives for all cases can result in misleadingly low clinical risk if specificity and further clinical workflow costs are ignored.
Prospects for Future Research
These results motivate several future directions:
- Development of theoretically principled, class-aware filtering strategies that integrate cost asymmetry in sample selection—beyond loss- or class-agnostic filtering.
- Adaptive tuning of cost ratios and loss weights to dataset-specific class imbalance and clinical context, potentially leveraging meta-learning.
- Extension of the framework to multi-class, hierarchical diagnostic settings, where cost matrices, rather than scalars, drive optimization.
Practical deployment in real-world medical systems mandates risk-aware protocol adoption for regulatory compliance and patient safety.
Conclusion
Noise-robust deep learning for medical image classification, if evaluated solely by symmetric metrics, is insufficient for the practical requirements of patient safety. This study robustly demonstrates that standard and SOTA robust training approaches may fail to optimize for clinical risk, particularly as label noise increases. Integrating cost-sensitive optimization with appropriate robust algorithms—specifically, those maintaining minority class representation—substantially improves real-world safety. Risk-aware optimization and evaluation are essential, and future noise-robust classification frameworks must internalize clinical asymmetries to ensure alignment with diagnostic utility.