- The paper introduces Risk-Calibrated Loss (RCL) which integrates a clinical severity matrix to penalize fatal classification errors in medical imaging.
- RCL shifts the error landscape by converting critical Type II errors into less severe Type I errors to improve overall diagnostic safety.
- Extensive experiments demonstrate that RCL significantly reduces critical error rates, achieving up to a 92.4% reduction in fatal misclassifications.
Risk-Calibrated Learning for Minimizing Fatal Errors in Medical Image Classification
Introduction
The proliferation of deep learning within medical imaging has accelerated diagnostic tasks across modalities such as radiology, dermatology, and histopathology. However, prevailing models trained with standard objectives (e.g., cross-entropy and its cost-sensitive or reweighted variants) do not differentiate between harmless misclassifications and those that are categorically hazardous. As a result, present systems frequently exhibit semantic incoherence: high-confidence errors that cross critical clinical boundaries (e.g., predicting benign for a malignant lesion), undermining safety and trust in clinical settings.
This work formalizes a taxonomy of medical classification errors, introduces the Risk-Calibrated Loss (RCL) framework to embed clinical risk asymmetry into the training objective, and demonstrates empirically that minimizing fatal, Type II errors (i.e., critical false negatives) can be decoupled from standard performance without recourse to architectural changes or complex inference pipelines.
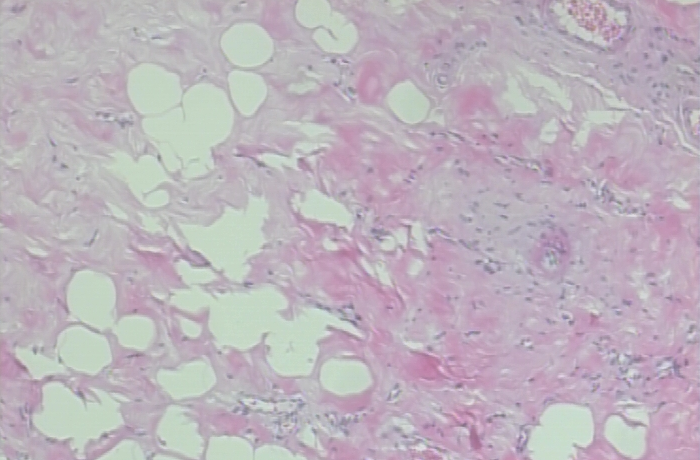
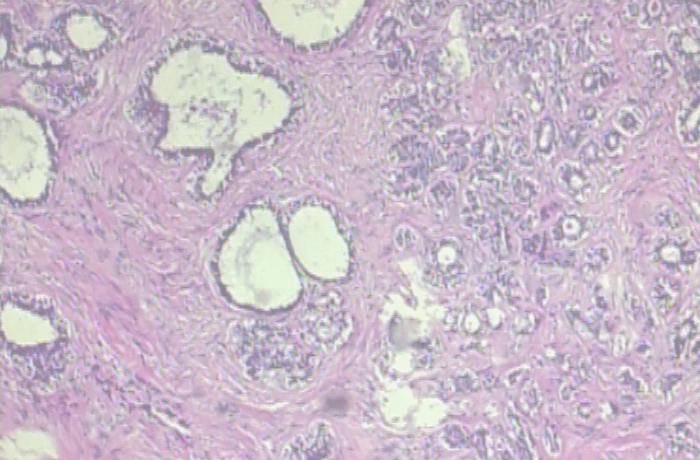
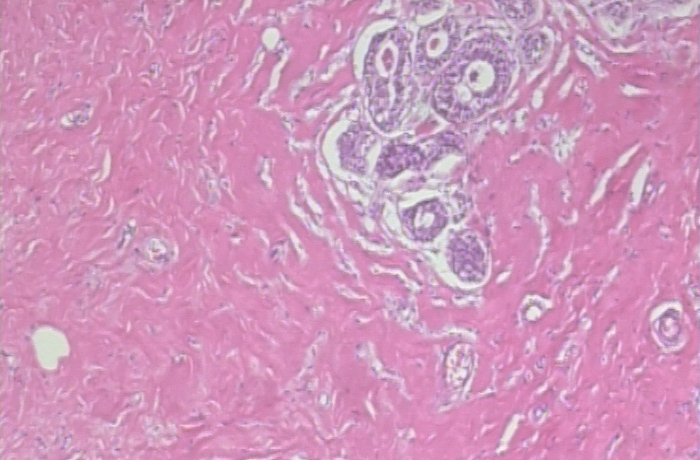
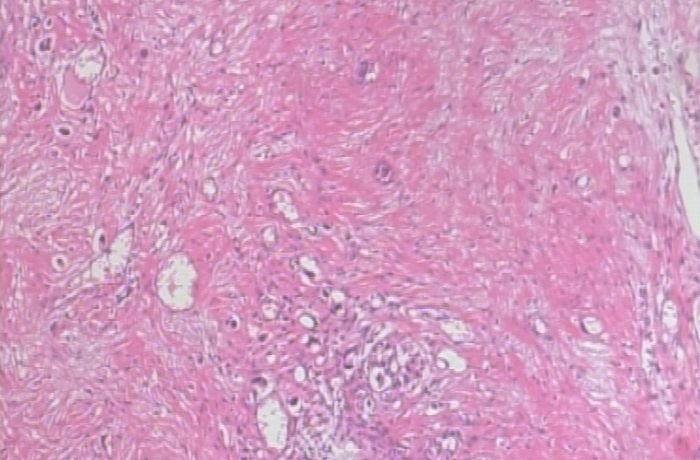
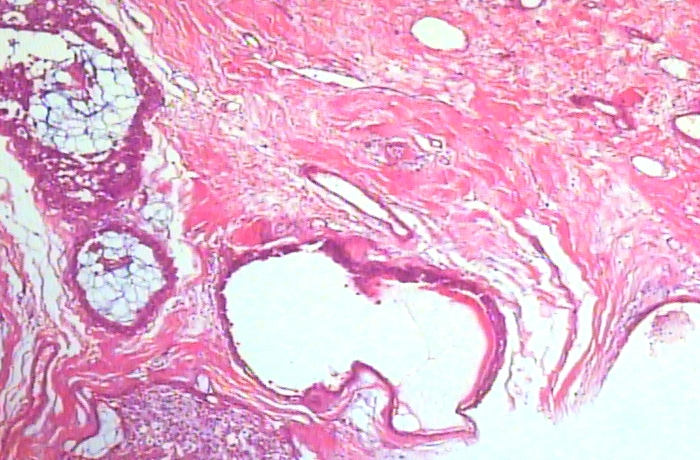
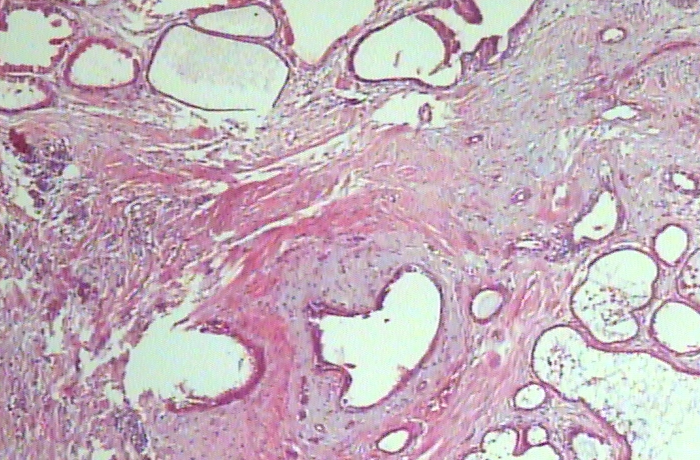
Figure 1: Example errors on the BreaKHis dataset. (a) Visual ambiguity: benign confusions are safe; (b) Type I (costly): benign as malignant yields unnecessary intervention; (c) Type II (fatal): malignant as benign is clinically catastrophic.
Taxonomy of Medical Classification Errors
The study delineates medical AI errors into three semantically distinct classes:
- Visual Ambiguity (Safe Errors): Intra-class errors reflecting genuine visual similarity (e.g., confusion between histological subtypes within the benign category).
- Type I Errors (False Positives): Cross-superclass errors where benign is flagged as malignant. Although non-fatal, these induce significant psychological and procedural costs.
- Type II Errors (False Negatives): Critical cross-superclass errors where malignant lesions are classified as benign, introducing fatal diagnostic lapses.
This taxonomy properly aligns the model’s learning objective with real-world safety demands. Unlike traditional approaches (WCE, Focal Loss) that address data imbalance or statistical hardness, these do not model the direction and consequences of error.
Risk-Calibrated Loss: Embedding Asymmetric Safety in Optimization
The central contribution is the Risk-Calibrated Loss (RCL), which embeds a clinical severity matrix M into the loss computation. Each off-diagonal element of M is parameterized by α and β, corresponding to the penalties for Type I and Type II errors, respectively, while safe intra-class confusions are minimally penalized. This construction yields a loss landscape where the optimizer is explicitly driven away from the subspace corresponding to fatal semantic incoherence.
Mathematically, for true class y and predicted class y^:
LRC(x,y)=My,y^⋅LCE(x,y)
with Mvisual=1, Mtype1=α, and Mfatal=β (M0).
By contrast, standard WCE or Focal Loss are agnostic to which class is predicted incorrectly, enforcing only global (frequency- or confidence-based) rescaling. RCL introduces a directionally-aware gradient amplification for medically unacceptable errors.
Empirical Validation across Modalities
The method was evaluated across four heterogeneous datasets: Brain Tumor MRI, ISIC 2018 (dermoscopy), BreaKHis (breast histopathology), and SICAPv2 (prostate histopathology). RCL consistently exhibited superiority in minimizing Critical Error Rate (CER) across all backbones.
Safety Gains Analysis
On the ISIC 2018 dermoscopy dataset—reflecting high class imbalance and visual ambiguity—Focal Loss delivered a CER of 39.41% (ResNet-50), whereas RCL reduced it to 18.24%, a relative improvement of 53.7%. For SICAPv2 (ViT-B16), CER dropped from 10.69% to 0.81% (a 92.4% reduction).
Safety-Accuracy Trade-off
Reduction of Type II errors does incur a marginal decline in fine-grained F1 or overall accuracy (ISIC 2018: F1-macro drops from 0.692 to 0.595, accuracy from 80.9% to 76.1%), as shown in Figure 2. In all examined clinical setups, this trade-off is highly preferable: improved sensitivity to malignancy (lowering fatal misses) at the expense of increased benign alarms is consistent with best clinical practice.
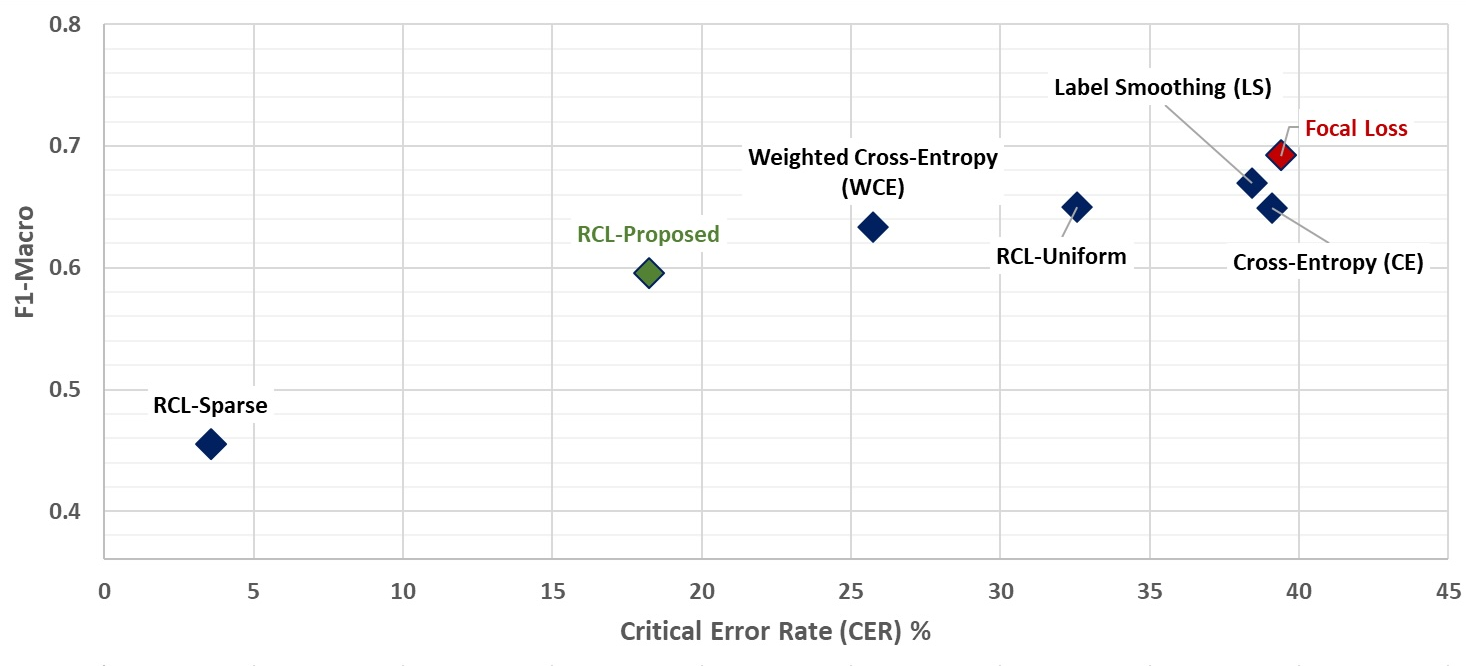
Figure 2: The safety-accuracy frontier (ISIC 2018, ResNet-50): RCL moves the operating point toward lower CER with an acceptable reduction in F1.
Analysis of error distributions reveals that the deployment of RCL predominantly converts fatal errors into alarm-triggering Type I errors without degrading discrimination among benign subtypes, confirming the method’s operation as a semantic safety margin without total collapse of utility.
Ablation and Configuration Sensitivity
Extensive ablation confirms the necessity of asymmetric penalties: configurations with excessive symmetry (M1) fail to suppress critical errors effectively. RCL’s optimal configuration (M2, M3) achieves substantial fatal error reduction while avoiding F1 collapse. Sparse penalization (low M4, high M5) entirely eliminates Type II errors but may severely depress discriminative metrics—a scenario analogous to a model defaulting to “malignant” for all ambiguous samples.
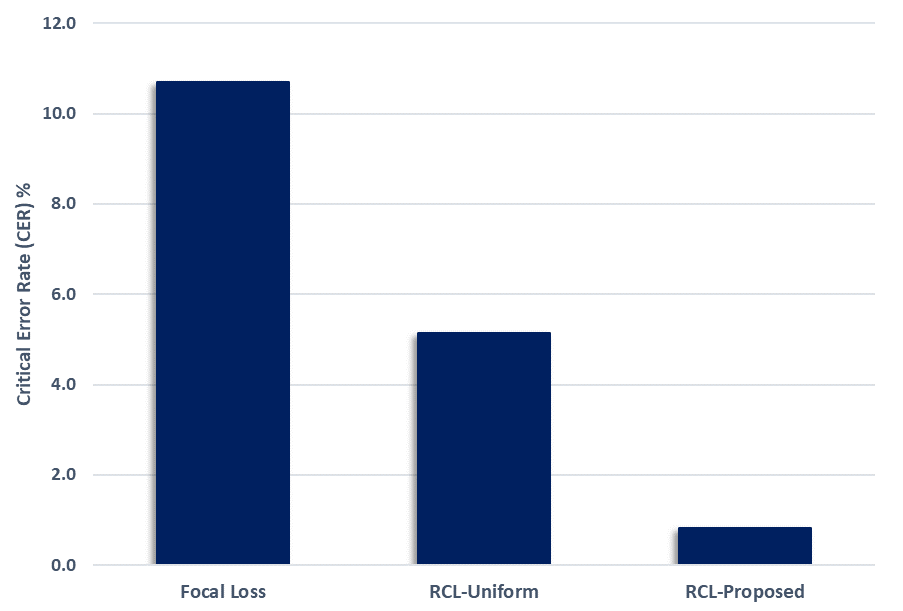
Figure 3: Effects of loss penalty configuration on CER; only asymmetric (Proposed) settings achieve sub-1% CER on challenging datasets.
Implications, Limitations, and Future Directions
Risk-Calibrated Learning provides a robust, parameter-efficient, model-agnostic framework for enforcing clinical safety. By minimizing catastrophic errors without augmenting architectural complexity or introducing inference-time overhead (e.g., cascading or secondary classifiers), RCL is ideally suited for integration into existing clinical pipelines as a safety-promoting drop-in replacement for standard objectives. The approach exposes the safety-accuracy Pareto frontier and allows for explicit, clinically guided tuning of Type I/Type II error trade-offs.
A key limitation is reliance on discrete, domain-expert-defined risk hierarchies; granular clinical settings may demand more nuanced, probabilistic severity models. Furthermore, the increase in false positives, while preferable to missed malignancies, could induce operational burdens such as alarm fatigue. RCL is thus positioned as a triage enforcer rather than a final decision-maker.
Future work should extend RCL to structured prediction tasks (segmentation, detection), multi-modal fusion (combining imaging, text, and biomarkers), and consider dynamic or context-dependent penalty matrices reflective of individualized clinical risk.
Conclusion
This work establishes that the clinical safety of medical AI models can be directly and efficiently optimized via a confusion-aware, asymmetric loss function. The Risk-Calibrated Learning framework enforces the operational imperative to prioritize the elimination of fatal errors above marginal improvements in standard metrics. Empirical results across diverse imaging modalities substantiate that this approach is superior to classical cost-sensitive or hardness-based objectives for safety-critical deployment. Ongoing extensions will generalize the framework to more complex and heterogeneous medical decision spaces.
ArXiv Reference: "Risk-Calibrated Learning: Minimizing Fatal Errors in Medical AI" (2604.12693)