- The paper proposes the AMT-MA framework, which isolates transportable treatment effects from heterogeneous cardiovascular trials to aid modern clinical decision-making.
- It employs a Nuisance-Anchor Decomposition to separate stable effect components from nuisance variability and uses a sign-stability diagnostic to guide pooling decisions.
- Simulation studies and real-data applications show that AMT-MA reduces bias and quantifies transport uncertainty compared to traditional meta-analytic methods.
Introduction and Motivating Context
The paper proposes the Stable Transport Meta-Analysis (AMT-MA), a meta-analytic methodology specifically addressing the estimation of treatment effects from heterogeneous clinical trials, especially relevant in cardiovascular medicine. Conventional meta-analytic estimators (fixed-effect, random-effects) summarize the average effect across heterogeneous trials, thus conflating systematic variations arising from temporal, geographic, procedural, or patient-mix heterogeneity. The AMT-MA framework instead targets the stable, clinically relevant component of the effect that is transportable to a user-specified target population, operationalizing an explicit shift from the historical averaging paradigm to robust target-population inference.
Methodological Framework
Nuisance-Anchor Decomposition
Central to the methodology is the decomposition of the trial-specific treatment effect θ(x) into:
θ(x)=Z⊤β⋆+δA(x)
where Z are transportable moderators (e.g., age, year), β⋆ the stable effect surface invariant to anchor variables, and δA(x) an anchor-aligned nuisance component capturing systematic variability (e.g., era, adjudication procedures, geographical regime). The AMT-MA estimator estimates β⋆ but explicitly does not transport γ (the anchor coefficient), thereby restricting the target effect to the stable Z⊤β⋆ component.
Estimation Objective
The estimator blends two loss components: a global inverse-variance weighted average loss and a robust scale-normalized softmax-minimax loss across predefined regimes (typically interactions of anchor variables). Explicitly,
(β^,γ^)=argβ,γmin{(1−ρ)Lavg+ρLrob+λγ∥γ∥22+λR∥β∥22}
where the blend weight ρ calibrates between average-fitting and robustness, and θ(x)=Z⊤β⋆+δA(x)0 regularizes the anchor nuisance term. Empirically, θ(x)=Z⊤β⋆+δA(x)1 offers a strong balance in simulation settings.
Target Effect and Abstention Mechanism
The estimated effect transported to the target population θ(x)=Z⊤β⋆+δA(x)2 is
θ(x)=Z⊤β⋆+δA(x)3
To mitigate overinterpretation in the presence of structural confounding or effect reversal across studies (sign-flip heterogeneity), a sign-stability diagnostic computes the precision-weighted proportion of studies aligned (above threshold and with consistent sign) with the estimated target effect. If the sign-stability score is below a threshold and the precision is sufficiently split across effect directions, AMT-MA abstains from producing a pooled estimate.
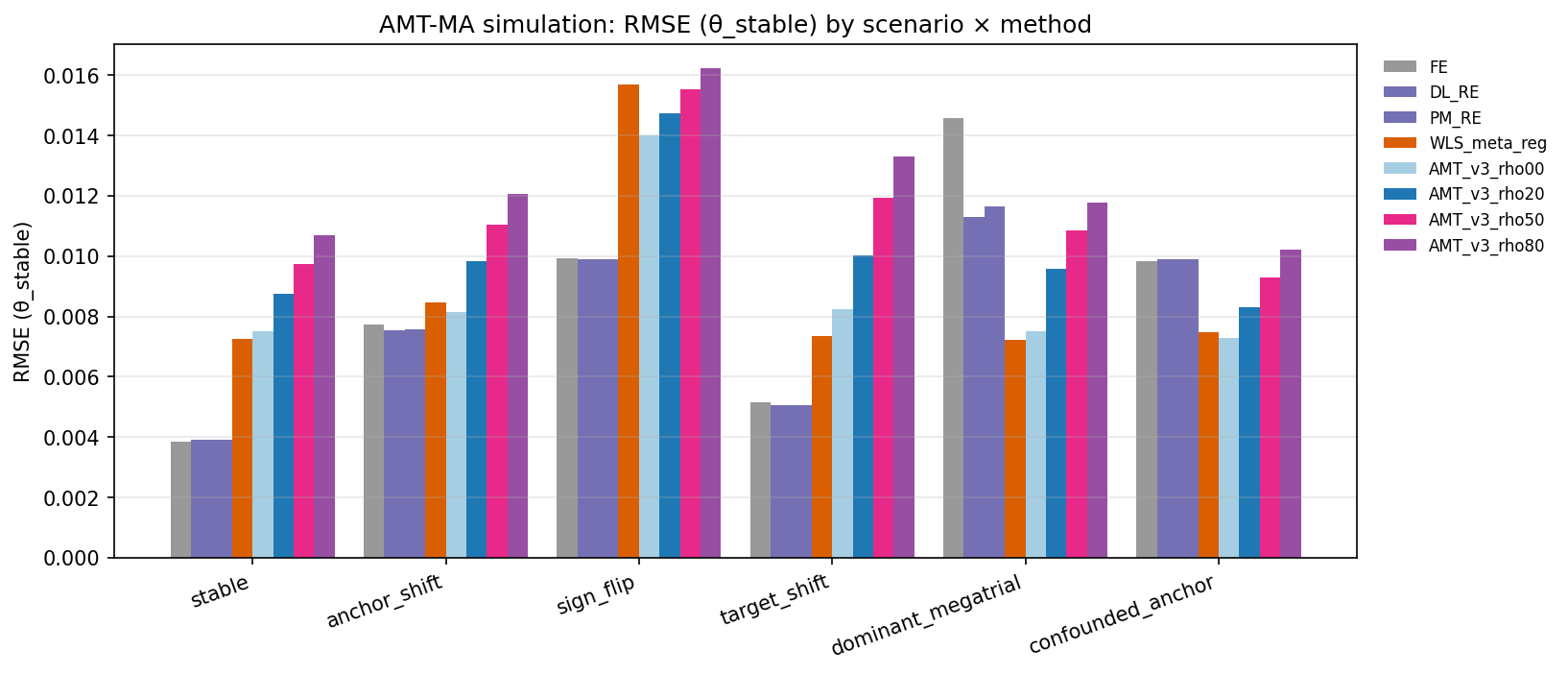
Figure 1: RMSE of θ(x)=Z⊤β⋆+δA(x)4 across simulation scenarios comparing AMT-MA with classical methods; robustness/efficiency trade-off is governed by method and θ(x)=Z⊤β⋆+δA(x)5.
Six simulation regimes systematically explored the AMT-MA performance:
- Homogeneous scenario: All trials share the same effect.
- Anchor shift: Older-era trials systematically bias effect.
- Sign-flip: Regions with opposing true effects.
- Target shift: Modern target differs from historical trial population.
- Dominant mega-trial: One large outlier trial dominates.
- Confounded anchor: Anchors highly correlated with important moderators.
Numerical results indicate:
- Under genuine homogeneity, AMT-MA incurs an expected efficiency loss (RMSE of 0.0087 with θ(x)=Z⊤β⋆+δA(x)6 versus 0.0039 for DerSimonian-Laird RE) due to robustness reservation.
- In anchor shift and confounded anchor settings, classical pooling exhibits substantial bias (θ(x)=Z⊤β⋆+δA(x)7 and θ(x)=Z⊤β⋆+δA(x)8, respectively), while AMT-MA reduces bias by an order of magnitude.
- Under sign-flip heterogeneity, AMT-MA abstains from pooling in 84% of replications, in contrast to stable settings (abstention 28–30%); specificity is strong but not perfect.
- Coverage probabilities for AMT-MA’s perturbation intervals are typically better than classical Wald intervals in adversarial regimes but are not universally nominal.
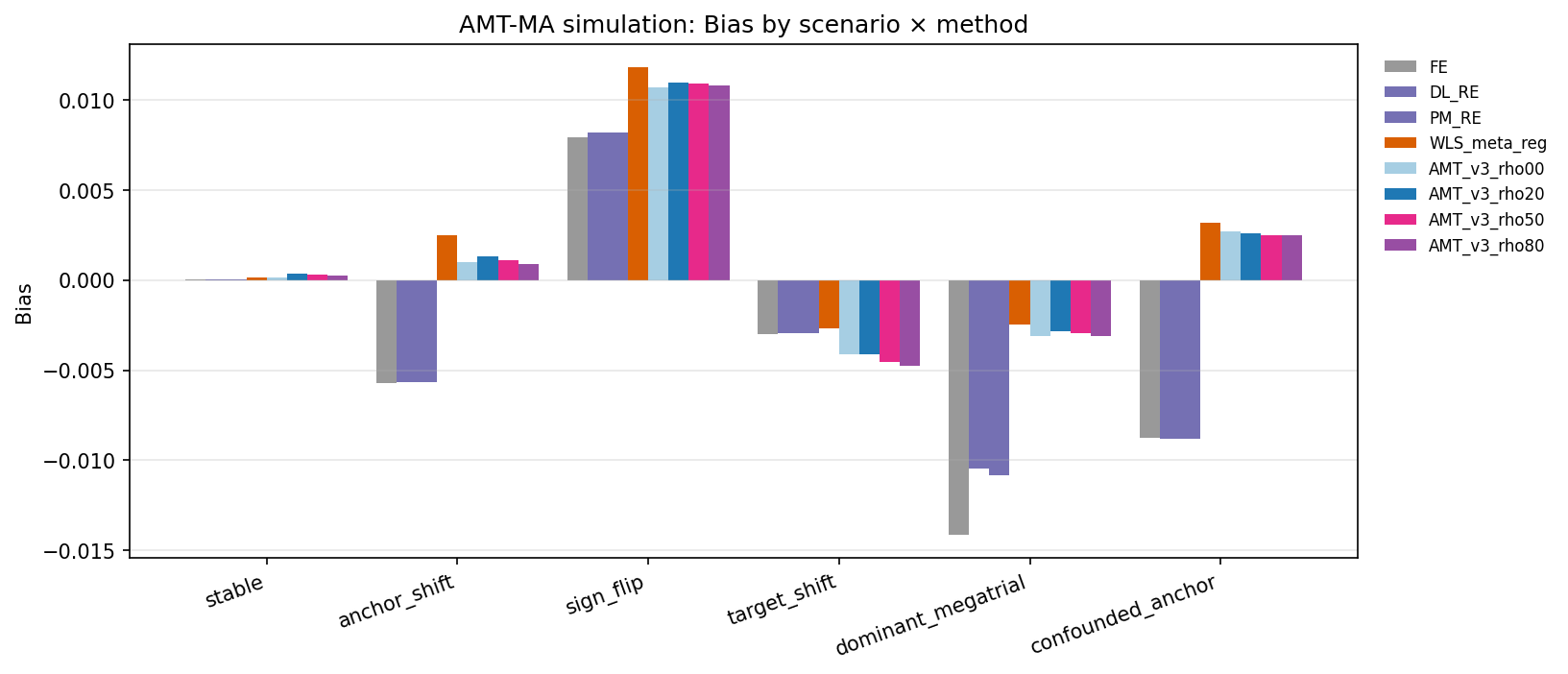
Figure 2: Bias of θ(x)=Z⊤β⋆+δA(x)9 by scenario and estimator, highlighting bias attenuation by AMT-MA in anchor-shifted and confounded regimes.
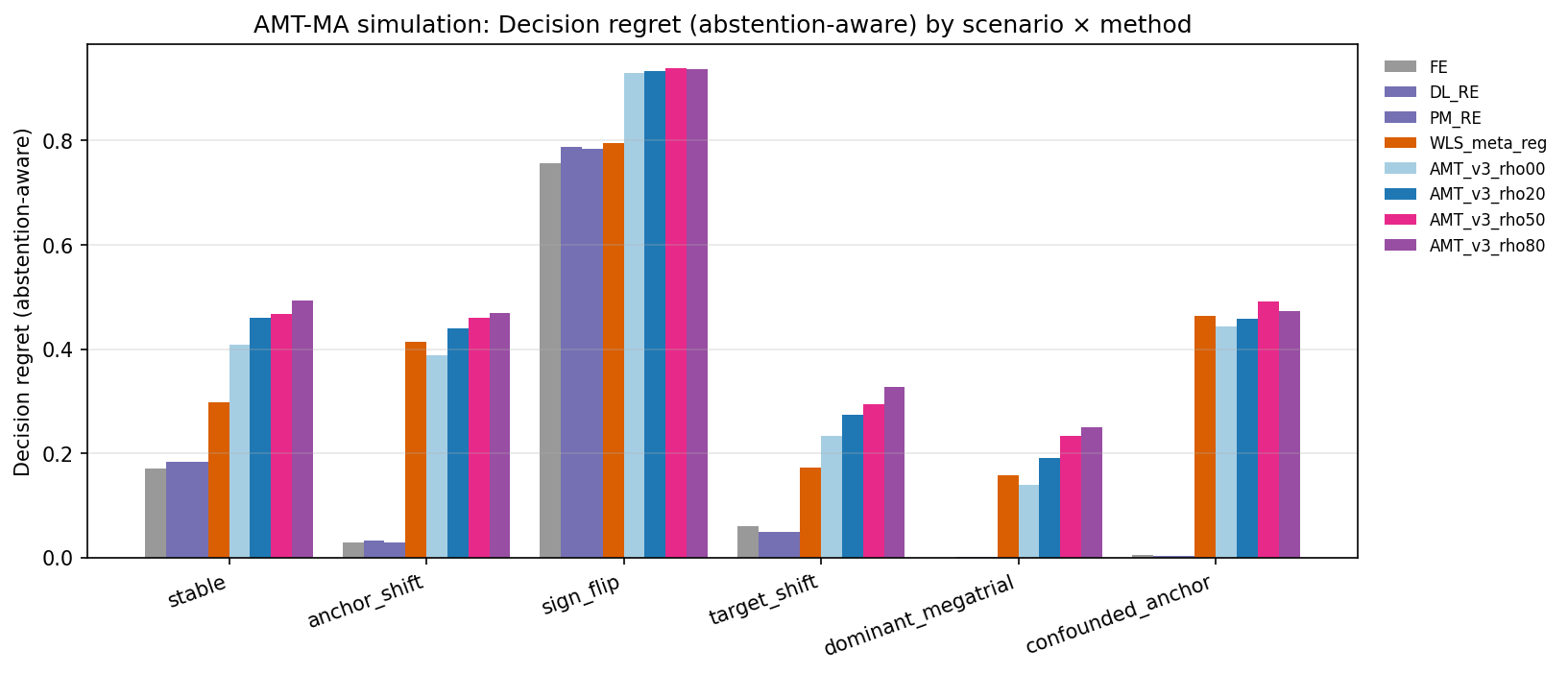
Figure 3: Decision regret of treat-if-negative-threshold policies, illustrating the decision cost when the transported effect shifts across target populations.
Olkin 1995 Streptokinase Trials
The Olkin dataset represents 70 post-MI mortality trials over 1959–1988, with varying patient mix, therapy, and endpoints. AMT-MA, using era and trial size as anchors, estimates the modern-era (1995) effect. The classical random-effects pooled log(OR) is Z0 (OR Z1), but the AMT-MA perturbation interval at the later era is notably wider (Z2 to Z3), including the null, quantifying explicit transport uncertainty rather than attenuation of point estimate.
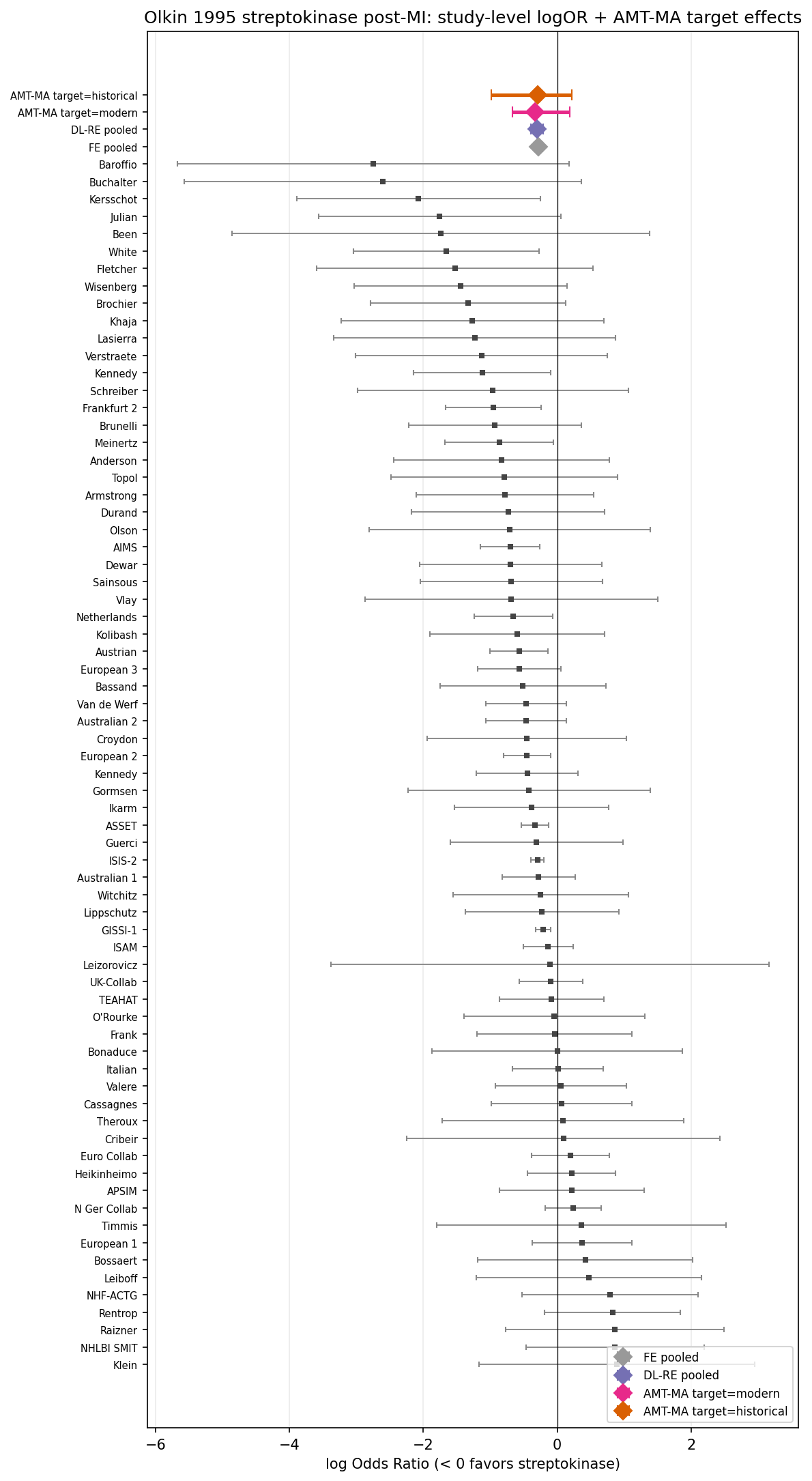
Figure 4: Olkin 1995 streptokinase trial effects with classical pooled and AMT-MA target summaries; AMT-MA yields a wider interval incorporating transport uncertainty to newer era.
Aspirin Primary Prevention Trials
For five aspirin primary prevention trials, AMT-MA (using contemporary-vs-older era as anchor) yields a modern-target OR of Z4 with a wide interval (Z5–Z6), ruling out only large benefits and bracketing the null, reflecting the limited and shifting trial evidence regarding aspirin’s efficacy in modern populations.
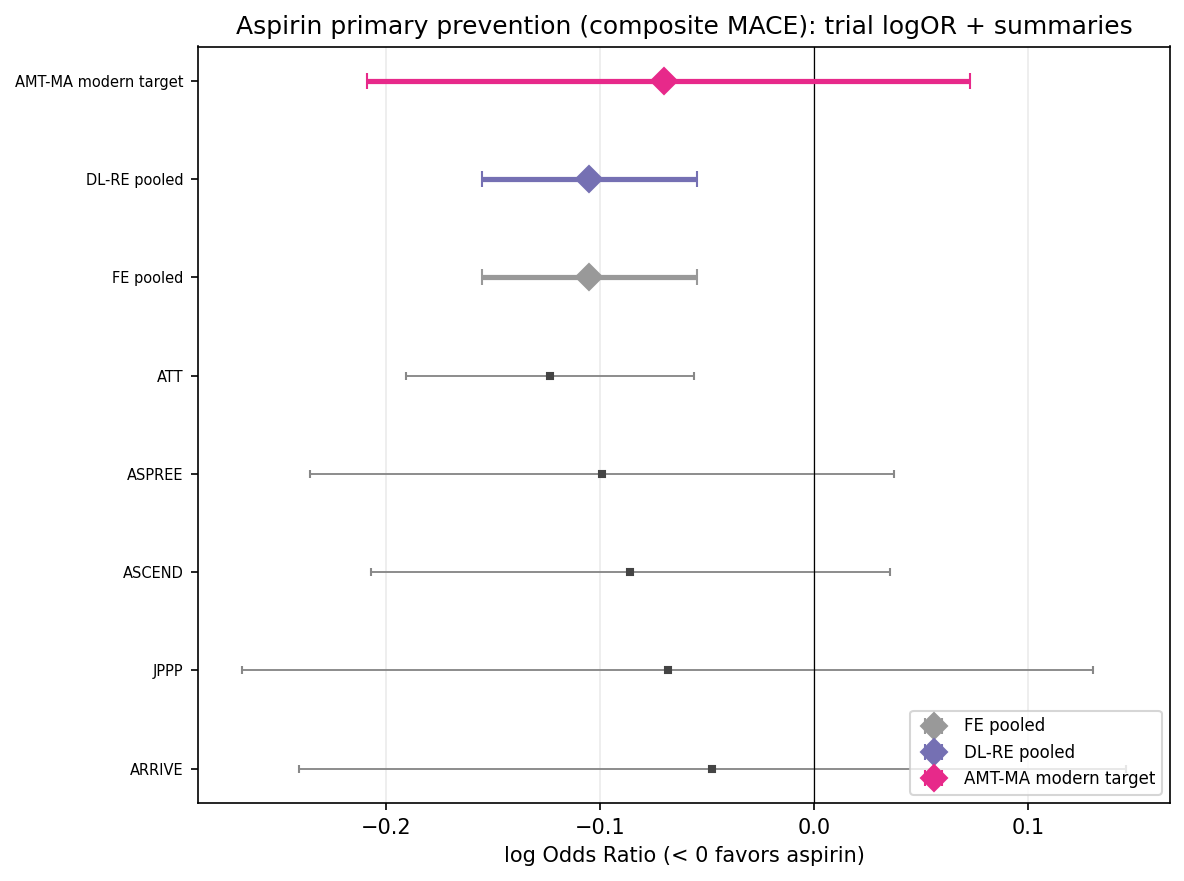
Figure 5: Contemporary aspirin primary prevention MACE trials; AMT-MA interval at the modern target brackets the null effect, reflecting lack of robust benefit and substantial transport uncertainty.
Practical and Theoretical Implications
AMT-MA operationalizes an explicit estimand shift for systematic evidence synthesis under heterogeneity:
- The framework enables transport of trial evidence into contemporary clinical populations with quantified uncertainty, superseding historical averaging that is often irrelevant for modern decisions.
- The sign-stability diagnostic provides a rigorous, transparent criterion for when pooled estimation is inadmissible—critical in settings with directionally conflicting evidence or effect reversal.
- In scenarios where the anchor-moderator structure is correctly specified, joint WLS meta-regression will often suffice; the incremental benefit of AMT-MA is robust diagnostic and explicit non-transport of anchor components.
- The method naturally extends to individual participant data (IPD) and domain-adaptive frameworks.
Limitations and Future Directions
Key limitations include dependence on correct anchor versus moderator variable selection, requisite domain knowledge, and the practical restriction of the number of variables when Z7 is small. Inference via perturbation resampling is limited by the quality of reported standard errors in aggregate-level data. While AMT-MA generally improves bias and coverage relative to unadjusted pooling in adversarial settings, it is not strictly dominant and incurs efficiency costs under homogeneity.
Future developments include:
- Extension to Bayesian or cluster-bootstrap inference paradigms.
- More automated or model-based anchor selection, including sensitivity procedures for the Z8/Z9 assignment.
- Asymptotic and finite-sample theory for robustness and interval validity, especially under cross-trial non-exchangeability and model mis-specification.
Conclusion
AMT-MA offers a principled approach to meta-analytic inference in the presence of systematic trial heterogeneity, refocusing on transportable effects relevant for clinical decisions. The framework’s blend of robust estimation, explicit estimand definition, and diagnostic abstention provides rigorous guardrails for evidence synthesis and decision support in settings where historical averaging is conceptually and practically inadequate. While not a replacement for random-effects pooling as a descriptive tool, AMT-MA substantially enhances the formalization and interpretability of projection from the trial evidence base to target populations.