- The paper presents a novel single-camera, world-spaced 3D HMR pipeline for extracting clinically relevant gait metrics during the TUG test.
- It employs automated subtask segmentation and signal processing to derive key parameters like step length, variability, and sit-to-stand duration.
- Statistical analyses show strong associations between objective gait measures and fall risk scores, underscoring its clinical and scalable potential.
Accessible 3D Gait Analysis and Fall Risk Assessment in Community-Dwelling Older Adults via World-Spaced Human Mesh Recovery
Introduction
This work presents a single-camera, world-grounded 3D Human Mesh Recovery (HMR) pipeline for extracting clinically relevant gait parameters and assessing fall risk in older adults during the Timed Up and Go (TUG) test. The pipeline is based on the Ground View HMR (GVHMR) model and operates entirely from ordinary monocular RGB video, without the requirement for dedicated clinical motion capture systems, marker placements, or multi-view calibration. This paradigm significantly enhances the ecological validity and scalability of gait assessment within realistic community settings, targeting improved accessibility of objective fall risk evaluation.
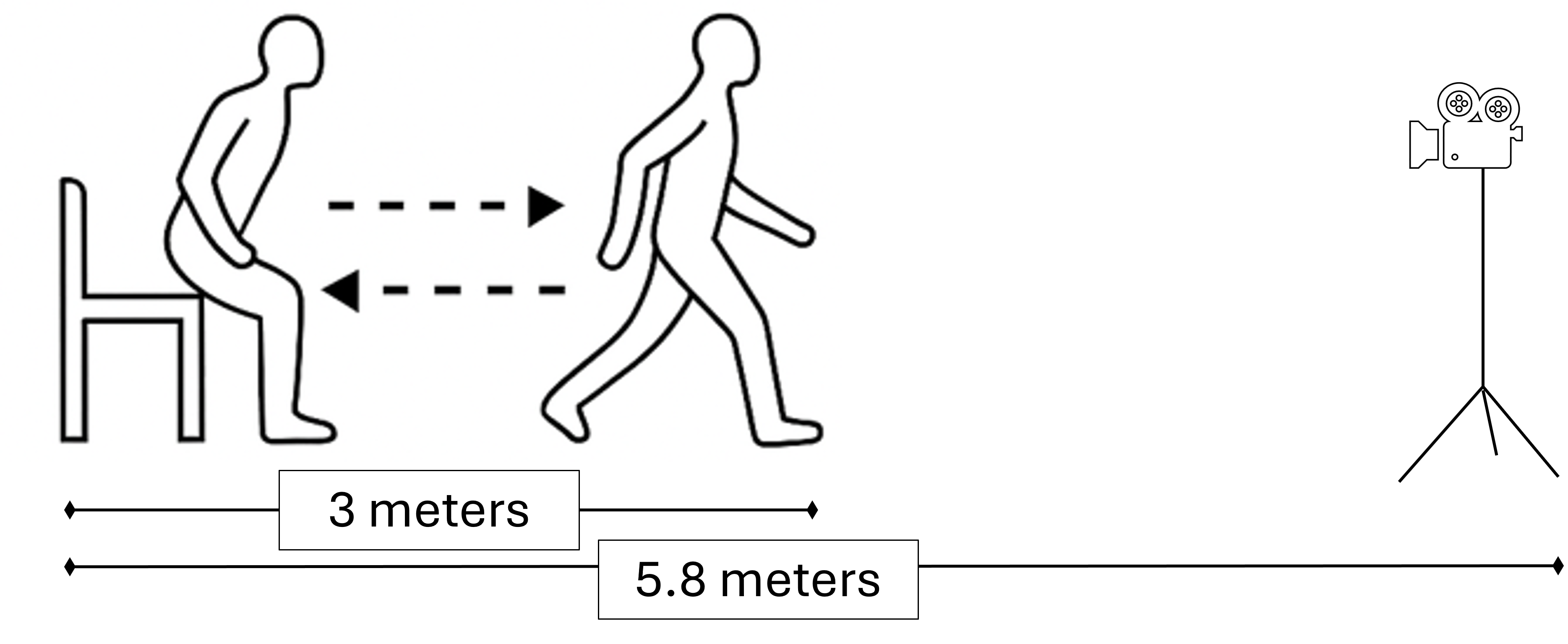
Figure 1: Schematic of the standard Timed Up and Go (TUG) test protocol as implemented in the study.
Methodology Overview
The protocol involves video capture of older adults completing three TUG trials per session, with recordings performed in local community centers. Each monocular video is processed by GVHMR to infer full 3D body pose trajectories and body shape parameters in a gravity-aligned, metric world coordinate space. The model explicitly disentangles human kinematics from camera egomotion, unlike canonical 2D keypoint-based or camera-relative 3D HMR systems, which is crucial for extracting physically meaningful trajectory and gait measures.
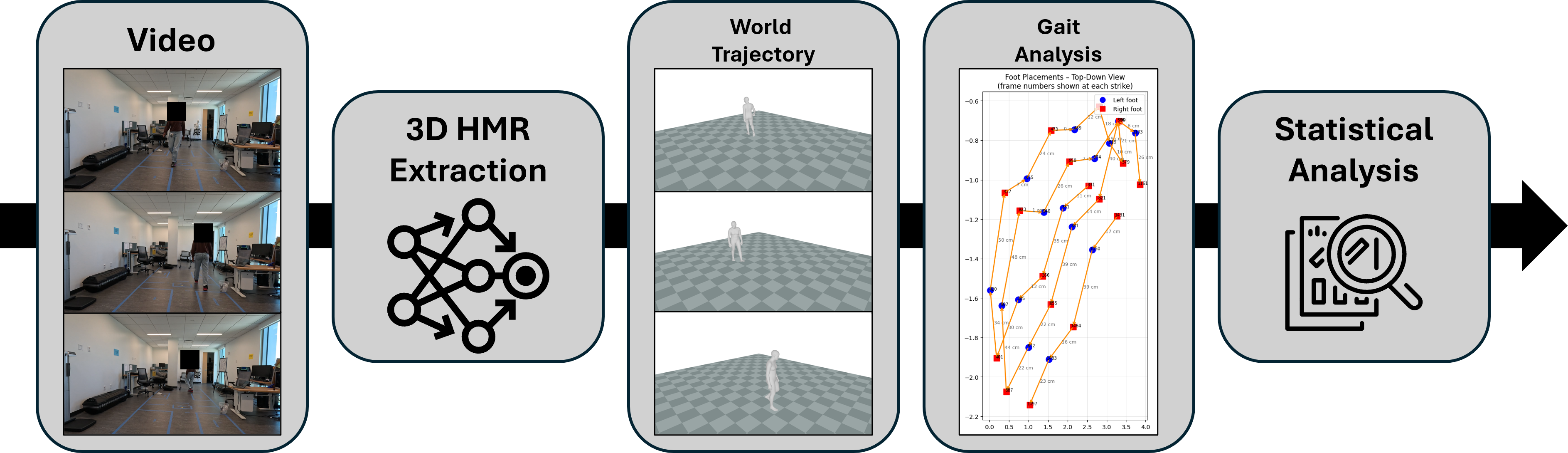
Figure 2: End-to-end pipeline built on GVHMR outputs: monocular video input, metric world-trajectory extraction, automated spatiotemporal gait analysis, and statistical modeling against fall risk indicators.
Temporal and spatial parameters derived from GVHMR are cross-validated against those produced by instrumented in-shoe sensors (XSENSOR), deployed as a reference for ground-truth foot contact times and step cycles.


Figure 4: Wearable XSENSOR insole and IMU system employed for sensor-based reference measurement.
Automated Subtask Segmentation and Gait Quantification
Robust signal processing is performed on GVHMR joint trajectories to automatically segment the canonical TUG subtasks (sit-to-stand, straight walking, turning, stand-to-sit) by combining vertical and anterior-posterior velocities and trunk flexion angles via bespoke composite signals. Step cycles are identified using ankle trajectory peak detection, and heel strikes are accurately located.
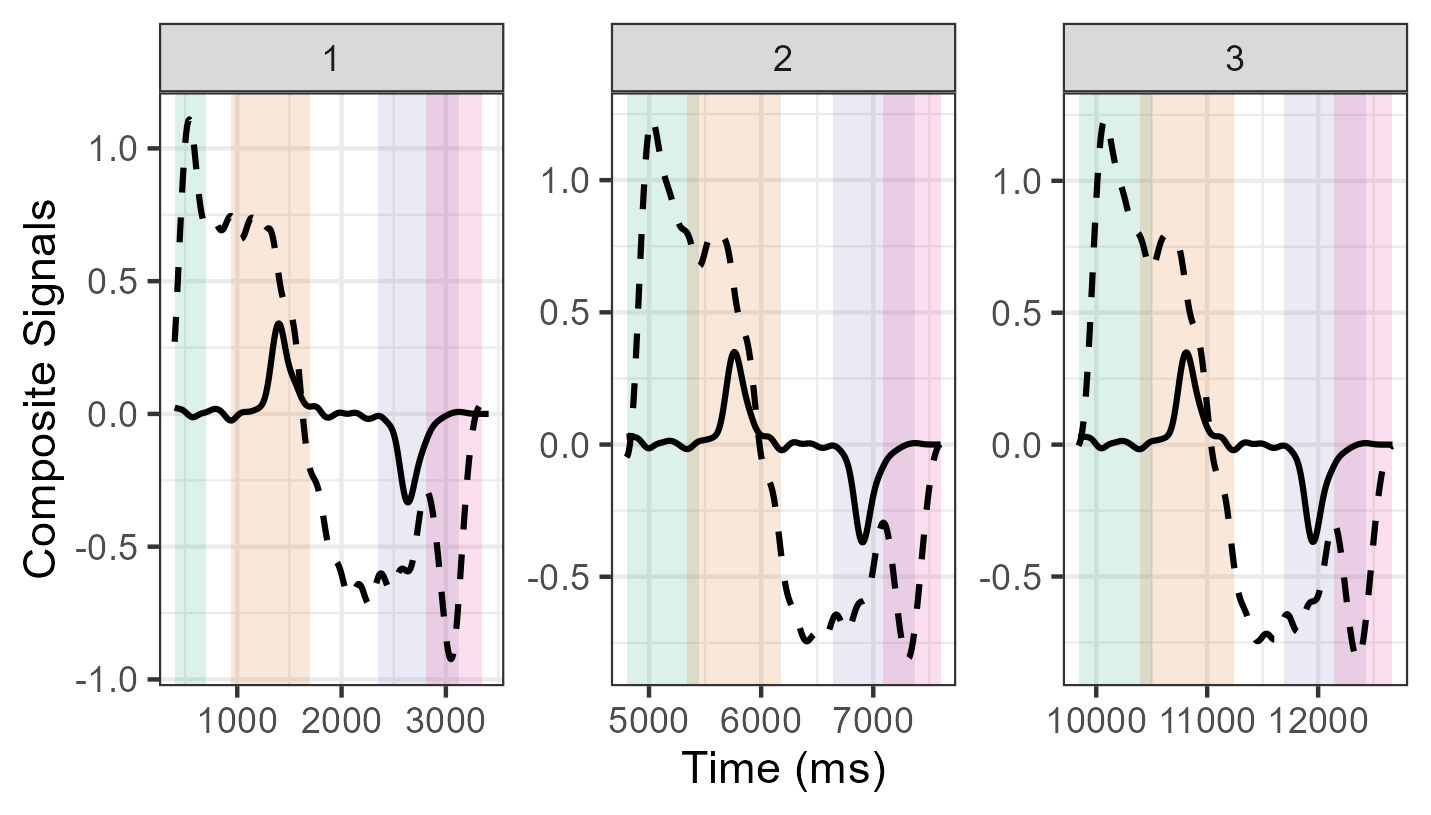
Figure 5: Example of subtask segmentation in TUG trials: hip-line velocity and composite sit-to-stand/trunk signals automatically delineate transitions.
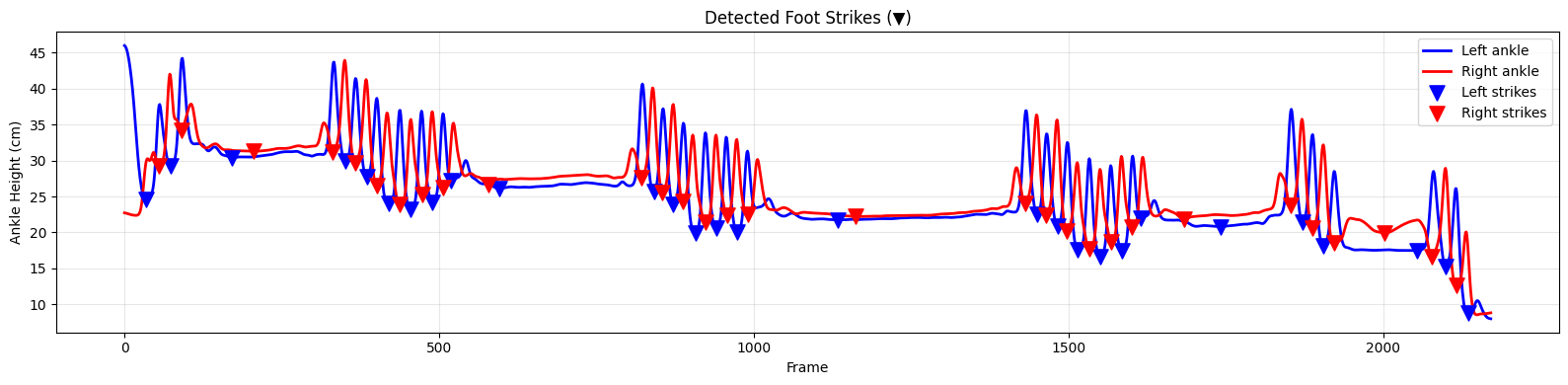
Figure 3: Automatic detection of heel strikes from video-based GVHMR joint trajectories by temporal peak analysis.
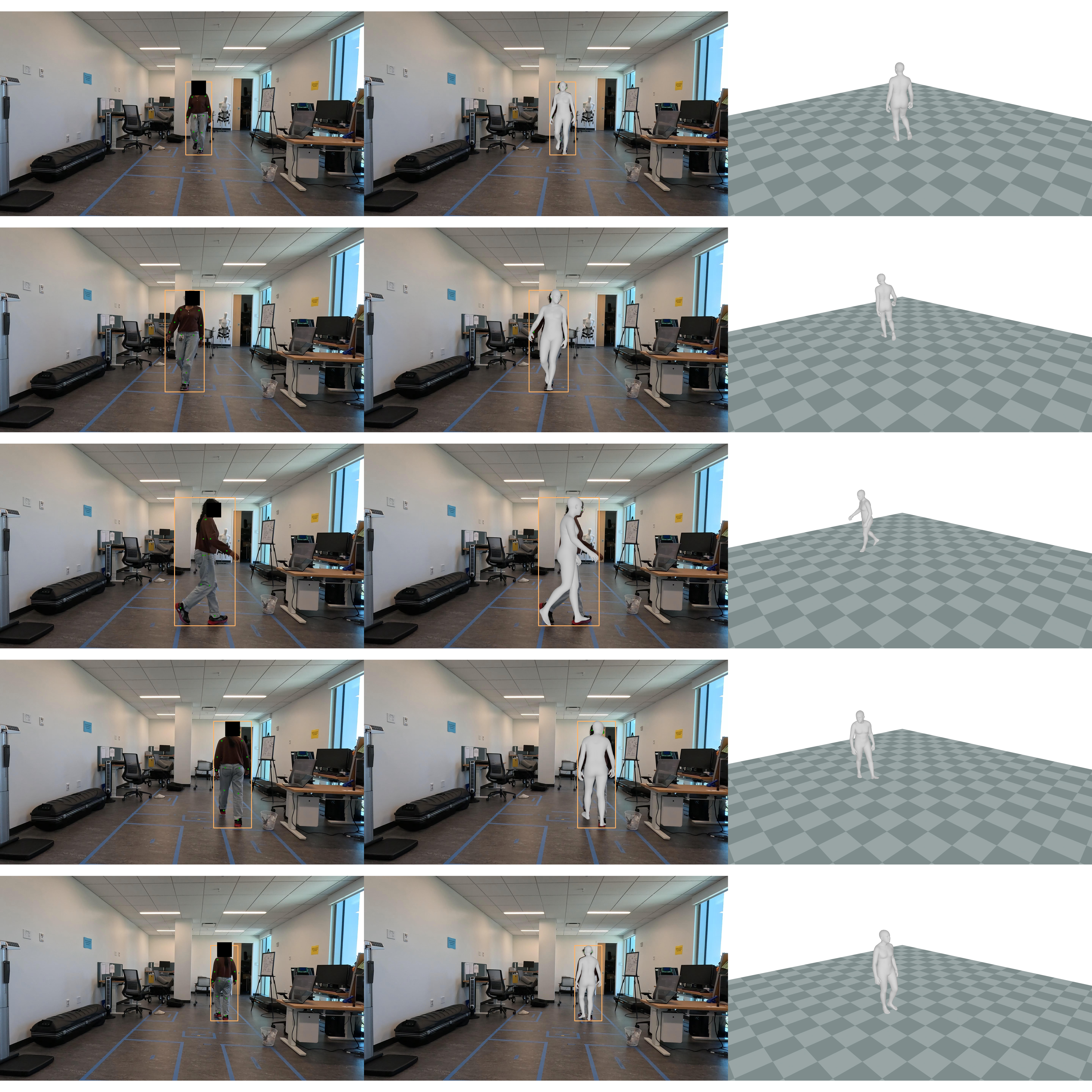
Figure 7: Illustration of video pipeline outputs: Research assistant performing TUG, camera-centric HMR overlay, global-centric 3D mesh trajectory recovery.
Extracted metrics include step length (SL), step length variability, step width (SW), sit-to-stand (STS) duration, and turn durations. Gaussian smoothing and filtering mitigate video pose jitter and ensure robust subtask delineation.
Statistical and Validation Analyses
Video versus Sensor Reliability
The GVHMR-derived step time (ST) aligns moderately with simultaneous insole-derived ST (n=90 trials, ρ=0.673, p<0.001), demonstrating the pipeline's competitive reliability for gait cycle timing. A systematic underestimation bias is observed, potentially attributable to differences in trajectory definition, reference points, and temporal synchronization.
Fall Risk Predictors and Gait Outcome Modeling
Linear mixed effects models are deployed to assess associations between objective gait features and established self-reported or balance-based fall risk scores (STEADI score, Short FES-I, BTrackS sway). The models accommodate repeated measures for each individual and include age as a covariate.
Key findings, with strong statistical significance, are:
- Higher self-rated fall risk (STEADI) predicts reduced step length (β=−1.36, p<0.001), increased SL variability (β=−19.62, p<0.001), and increased sit-to-stand duration (β=1.23, p=0.002).
- Greater fear of falling (Short FES-I) also predicts shorter and more variable step length.
- Step width variability is predicted by age (p=0.01) but not by fall risk factors.
- Turn durations are not significantly predicted by any fall risk indicator, diverging from certain prior studies.
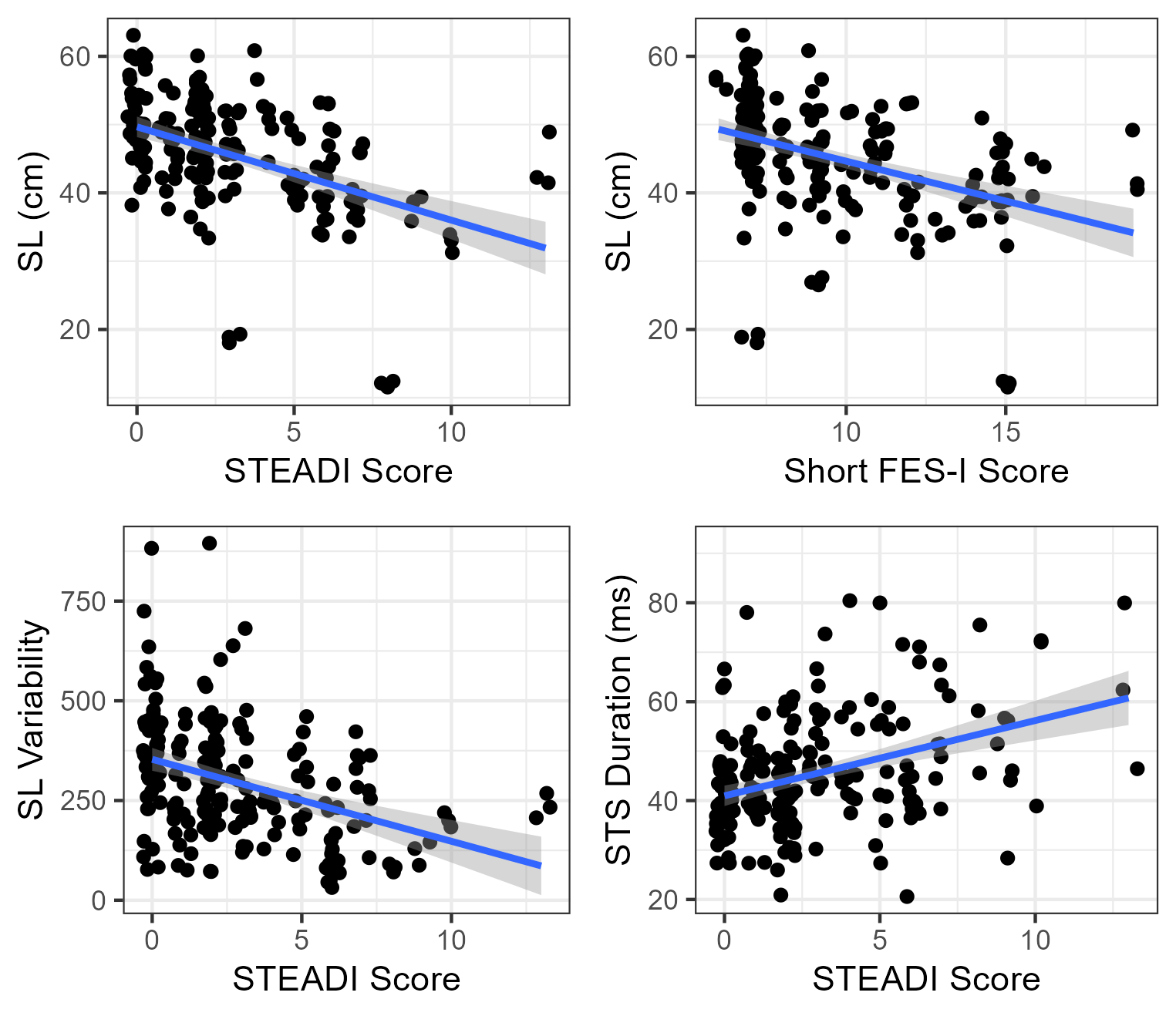
Figure 6: Associations between mean step length, step length variability, STS duration, and fall risk (STEADI, FES-I) across subjects.
Between-participant consistency for mean step length exhibits high intra-class correlation (ICC=0.81), with conditional ρ=0.6730 up to 0.85, underscoring the stability and clinical informativeness of the spatial gait features.
Implications and Limitations
This pipeline enables valid, markerless, ecologically realistic gait and movement assessment for older adults outside specialized laboratory contexts. World-spaced HMR, especially GVHMR, overcomes key technical limitations of earlier video-based and wearable-only solutions, supporting the extraction of depth-resolved and spatially invariant measurements critical for clinical interpretation.
However, sample size remains moderate (ρ=0.6731 older adults, 207 TUG videos), with future studies needed for expanded population diversity, prospective validation, and longitudinal tracking. Turn segmentation is sensitive to intra-individual movement strategy, motivating the development of finer-grained, participant-adaptive event detection within the GVHMR framework.
Conclusion
This work validates a robust, single-camera, world-space 3D pose estimation pipeline for gait and fall risk analysis in community-dwelling older adults. Strong associations between objective video-derived gait metrics—specifically step length/variability and sit-to-stand duration—and subjective/objective fall risk indicators demonstrate both clinical validity and feasibility for real-world deployment. The approach offers a viable, accessible augment to conventional sensor-based or manual screening tools, with potential for routine community, telehealth, or remote monitoring integration. Future directions include population scaling, extension to broader ADL assessment, and prospective functional decline prediction.