- The paper presents a game-based digital platform that boosts CHW efficiency in collecting anthropometric data via engaging gamification strategies.
- It employs a quasi-experimental design, showing a significant efficiency improvement from 49.04 to 73.9 (p=0.00004) compared to traditional methods.
- It highlights enhanced spatial malnutrition mapping through improved data coverage, though sustaining long-term engagement remains a key challenge.
Introduction
The paper "Mapping Child Malnutrition and Measuring Efficiency of Community Healthcare Workers through Location Based Games in India" (2604.07299) examines the utilization of a location-based, game-inspired digital platform to crowdsource anthropometric data through Community Health Workers (CHWs) and evaluates its impact on measurement efficiency and engagement in the Indian context. Addressing the persistent gap in continuous, high-resolution, georeferenced health data, the study proposes the integration of participatory game mechanisms as an engagement and data quality lever within public health data infrastructure.
Context and Rationale
CHWs, including Accredited Social Health Activists (ASHAs) and Anganwadi Workers (AWWs), are responsible for the acquisition and submission of child anthropometry data critical to malnutrition surveillance and targeted interventions. Legacy workflows predominantly involve manual register keeping followed by data entry into mobile applications, creating inefficiencies, data latency, and attrition in longitudinal data capture.
The authors argue that traditional mobile data entry approaches have limited success in incentivizing consistent, spatially comprehensive data collection among CHWs. Citing the five-year cycle of NFHS and resistance against contemporary data tracking platforms such as India's Poshan Tracker, the work situates itself at the intersection of HCI4D, participatory design, and serious games for digital health, extending the research through design (RtD) paradigm specifically to the challenge of inclusive geospatial health surveillance.
Game Design and Participatory Development
Employing a structured co-design methodology with 20 CHWs (organized in 10 pairs), the project iteratively synthesized context-appropriate game mechanics. The resulting application, implemented in Unity and distributed on mainstream app stores, was engineered to drive engagement over spatial and temporal axes—rewarding exploration of under-surveyed regions (spatial diffusion) and sustaining contribution over time via periodic campaigns, progressive narratives, and direct feedback regarding the societal impact of collected data.
An essential departure from prior work in this category is the explicit integration of game incentives with geolocation and longitudinal participation, leveraging both intrinsic and extrinsic motivators in a population of predominantly middle-aged, female, semi-literate para-health professionals. Figures illustrating the contrast between game-based digital data entry and traditional register-to-mobile workflows immediately underscore the operational context of the intervention.


Figure 1: CHWs entering data directly into a smartphone post-measurement (left) as opposed to the prior regime of recording in paper registers and later transcribing to app (right).
Experimental Methodology
A quasi-experimental, between-groups design compared a game-app intervention (n=94) with a standard data entry application control (n=94), with both arms balanced demographically. The recruitment aimed for sufficient power (anticipated effect size d=0.5, power=0.95). Baseline, immediate post-test (1 month), and delayed retention (3 months) assessments captured measurement efficiency. To mitigate placebo effects, the control group received equivalent attention absent the actual intervention.
Ethical conduct, detailed informed consent, and de-identification strategies were rigorously applied. The study setting encompassed diverse Indian states, adding to external validity regarding digital health tools in low-resource, heterogeneous environments.
Results
The intervention group demonstrated statistically significant improvement in measurement efficiency post-intervention (mean increase from 49.04 to 73.9, p=0.00004, Cohen's D=1.6), with partial retention of gains at the 3-month checkpoint (mean 69.14 vs. 54.84 in controls). Both groups showed a decline in retention scores over time, but efficiency remained substantially higher in the intervention group, suggesting both an initial persuasive effect and moderate persistence beyond the novelty window. The scores were independent of formal education levels, emphasizing the primacy of hands-on experience and appropriateness of participatory digital tool design for capacity building.
Strong claims are made regarding the superiority of the game-based approach, with the intervention group consistently outperforming the control on both immediate and delayed retention of efficiency. However, the authors note declining interest, underscoring the challenge of sustaining engagement without continuous refresh of game incentives.
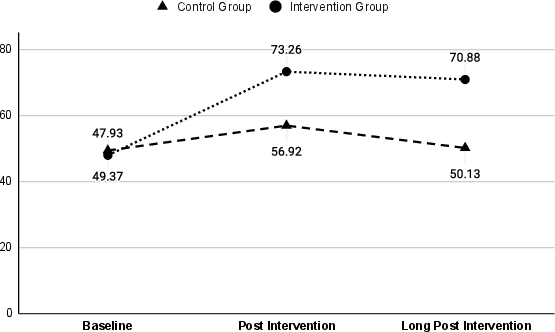
Figure 2: Trends in mean measurement efficiency scores for both groups over baseline, post-test, and long-post test periods.
The spatial data coverage enabled by the intervention prominently facilitated high-resolution hotspot mapping of malnutrition prevalence, which would not be feasible under the conventional reporting paradigm.
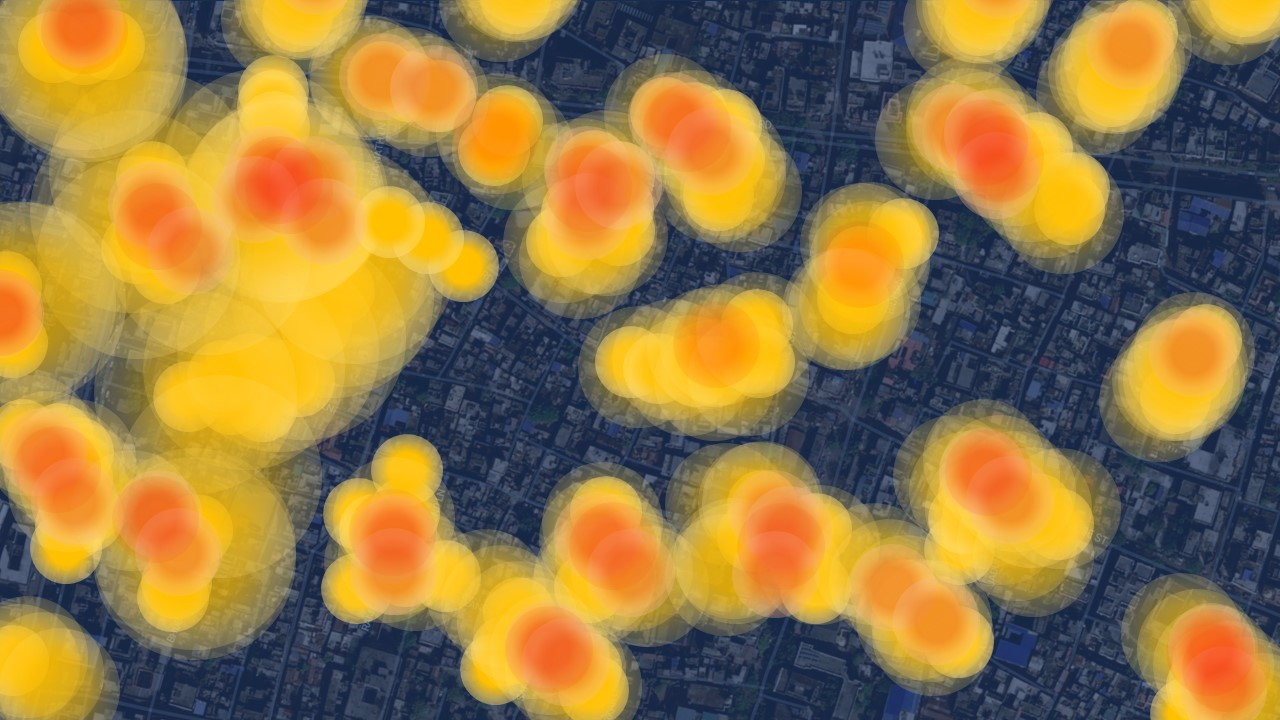
Figure 3: Density map visualizing malnutrition hotspots derived from game-app crowdsourced data.
Discussion
The study offers compelling numerical evidence that game-based digital health tools can not only accelerate engagement and accuracy in data entry among CHWs but also drive spatially distributed surveillance, overcoming both procedural inertia and motivational barriers. Uniquely, the work isolates the engagement and efficiency gains from confounding sociodemographic factors, highlighting the potential universality of the approach within similar health system architectures.
Importantly, the investigation surfaces operational risks including data falsification and negative peer dynamics (e.g., knowledge-based team criticism), stressing the need for robust data integrity checks and features for positive reinforcement in future app iterations.
The observed decline in retained efficiency after cessation of active incentives is consistent with literature on gamification for behavioral change and points toward the necessity of adaptive or continuously evolving game mechanics to maintain motivation in long-cycle health interventions.
From a technical and theoretical perspective, the work substantiates the application of RtD with embedded game analytics as a method to co-create, validate, and optimize digital tools for last-mile health actors. It reinforces the potential of combining geospatial, gamified, and participatory approaches for scalable, context-sensitive data infrastructure in resource-constrained settings.
Implications and Future Directions
Practically, the demonstrated approach can inform the design of future national health data systems, especially those reliant on distributed, para-professional data collection in low-resource and high-variance user environments. The inclusion of serious games as intrinsic workflow components, rather than adjunct training modules, could be transformative for sustained, spatially granular, and high-quality data flow.
Theoretically, the work pushes the boundary of serious games beyond conventional health education into the operational infrastructure of digital health surveillance and opens avenues for leveraging AI and adaptive gamification to personalize incentives, detect data anomalies, and optimize data acquisition strategies at scale.
In AI research, future investigations may extend this framework to semi-automated anomaly detection, real-time incentive adaptation based on engagement analytics, and integration with federated learning for privacy-preserving data synthesis across geographically distributed CHW cohorts.
Conclusion
The study delivers rigorous evidence for the efficacy of a co-designed, location-based game application in amplifying both the efficiency of anthropometric data acquisition and the geospatial resolution of child malnutrition mapping via CHW networks. Game-based data collection, when embedded in routine workflows and shaped through participatory design, can outperform traditional data entry in both immediate and medium-term efficiency, with ancillary benefits for spatial data completeness. The durability of these effects, however, depends on continuous engagement strategies, active incentive design, and attention to data integrity and user experience. This research provides a template for the future of crowdsourced public health monitoring at the intersection of HCI, AI, and digital epidemiology.