- The paper provides a detailed theoretical and empirical characterization of how reference group choice can qualitatively reverse decomposition conclusions.
- It employs real-world ICU data and simulated health data to demonstrate sign flips in both the explained and unexplained components.
- Results underscore the need to report both reference configurations to ensure robust attribution and avoid misleading policy inferences.
Sensitivity of Reference Group in the Oaxaca-Blinder Decomposition: Implications for Attributive Inference
Introduction
The paper "Do covariates explain why these groups differ? The choice of reference group can reverse conclusions in the Oaxaca-Blinder decomposition" (2603.29972) investigates a fundamental subtlety in the Oaxaca-Blinder decomposition (OBD): the dependence of its conclusions on the arbitrary choice of reference group. Although the index-number problem—where switching the reference group alters decomposed quantities—is acknowledged in the applied literature, the extent to which this changes substantive, qualitative conclusions (not just numerical magnitudes) has not been systematically characterized. This work provides both theoretical and empirical analysis illustrating that the OBD's substantive conclusions can differ, including sign flips in the explained and unexplained components, strictly as a function of reference group choice. The study leverages both real and synthetic data, comprehensive mathematical characterization, and an exploration of the prevalence and drivers of such reversals.
Background: Oaxaca-Blinder Decomposition and the Index-Number Problem
The OBD is a canonical statistical method for decomposing group differences in mean outcomes into a component "explained" by differences in group means of covariates and an "unexplained" component attributed to differences in the conditional outcome models. Given outcome Y and covariates X for groups H,K, and assuming (possibly group-specific) linear models, the gap in average outcomes is decomposed as:
- With reference group H:
ΔY=(μH−μK)⊤βH+μK⊤(βH−βK)+(αH−αK)
- With reference group K:
ΔY=(μH−μK)⊤βK+μH⊤(βH−βK)+(αH−αK)
These formulations reveal that both explained and unexplained components depend on which group's conditional model is the reference, and the implied counterfactual is not symmetric. This well-known "index number problem" is typically acknowledged but rarely interrogated regarding its substantive consequence on inferential claims.
Empirical Existence of Substantive Reference Sensitivity
A central contribution is the explicit demonstration that the choice of reference can yield not only quantitatively different results, but also qualitatively different substantive conclusions. In a real-world example analyzing gender differences in ICU mortality among patients with moderate tachycardia from the PhysioNet database, the explained component's sign flips with the choice of reference. For instance, taking women as reference, the explained component is positive and statistically significant, indicating that covariate differences place men at greater risk. With men as reference, the explained component is negative and insignificant (Figure 1). These findings persist after accounting for sampling variability with bootstrap inference.
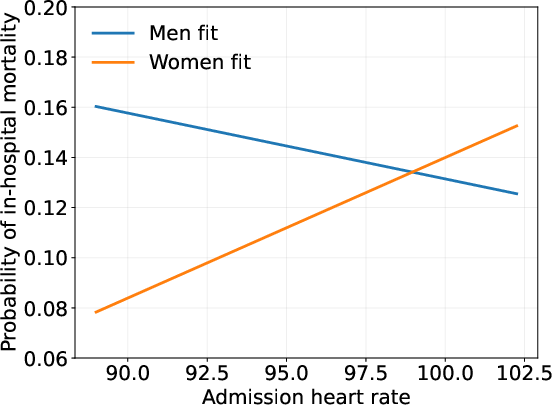
Figure 1: Linear fit of mortality on admission heart rate for each group when holding all other covariates fixed at their group means.
The sign reversal is not a numerical artifact—detailed analysis of group-specific coefficients shows that the direction of marginal effects for several covariates differs across groups, and the vector of mean differences in covariates preserves their contribution direction, inducing the sign inversion.
Further, a histogram of outcomes for the HR quartile two subgroup illustrates the population-level variability underpinning these results.
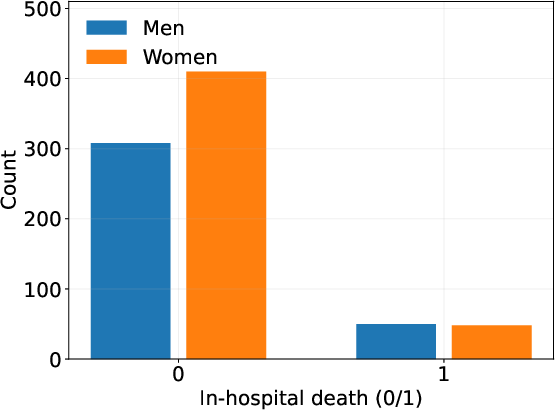
Figure 2: Mortality outcome histogram for HR quartile two subgroup.
A companion example employs simulated data in hypertension, with each group's systolic blood pressure (SBP) modeled as a function of BMI. Here, the unexplained component sign flips with the reference group, under perfect model specification and large samples. The slope and intercept parameters were chosen to reflect plausible healthcare disparities. The result demonstrates sign reversals are not an artifact of overfitting, misspecification, or small-sample instability.
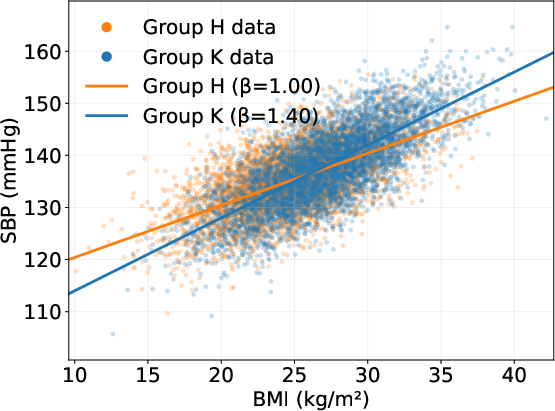
Figure 3: Population linear models of SBP on BMI by group and data samples.
Theoretical Characterization: Geometry of the Index Problem
The authors formalize the class of "sign flip" events, precisely defining when the sign of the explained or unexplained OBD component depends on reference group; i.e., when sign(Δμ⊤βH)=sign(Δμ⊤βK) for explained, and a more involved condition involving group-specific means, slopes, and intercepts for unexplained.
Analytic bounds are provided for the fraction of parameter space leading to such qualitative reversals. For both components, as the dimension of X increases, the region of parameter space that can produce sign flips approaches 50% (Figure 4), with no vanishing measure even for moderate-dimensional settings.
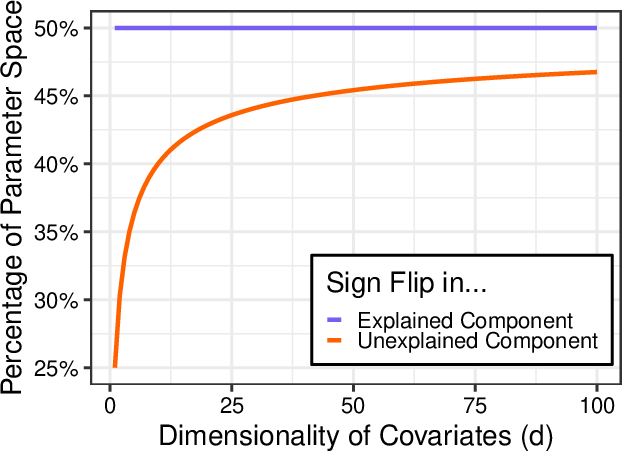
Figure 4: Percentage of parameter space leading to sign flips.
Simulation studies further confirm that even without standardizing the covariates, the fraction of sign-reversal solutions remains substantial (Figure 5).
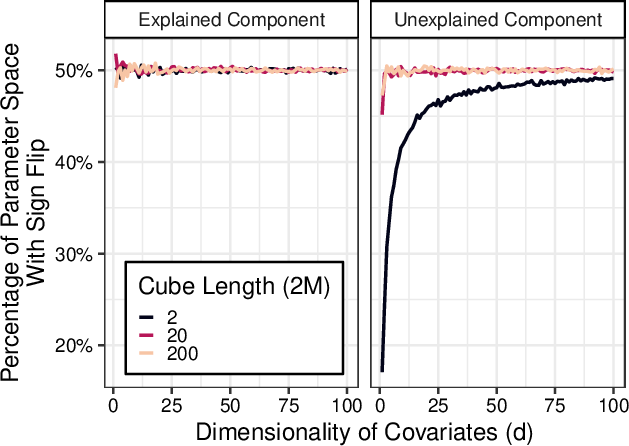
Figure 5: Percentage of parameter space leading to unexplained component sign flips, without covariate standardization.
Empirical Prevalence and Its Determinants
Despite the large theoretical measure, empirical tabulations across thousands of OBDs on real datasets (ICU and American Community Survey income/insurance analyses) find sign flips to be rare in practice. For example, among 139 partitions of ICU data, only 27 (19%) exhibited any sign reversal, and most were on small or randomly subsampled sets. For US labor force data, out of 355 candidate decompositions, essentially none displayed sign flips of practical significance.
The reason for this empirical rarity is elucidated via domain-specific structure: in most applied contexts, the direction of effect (e.g., the slope of a risk factor) is a-priori matched across groups. For the explained component, sign flips require that a covariate increases risk in one group while reducing it in another, which is generally inconsistent with most clinical, biological, or economic realities. For the unexplained component, a sign flip occurs when baseline differences (intercepts) and differential slopes misalign in a specific way—a scenario empirically suppressed by omitted variable structures and the intertwining of group-wide risk and sensitization.
Implications and Recommendations
The findings have significant implications for applied practice using OBD to attribute disparities:
- Substantive inference (even at the level of directionality) can be contingent and fragile with respect to reference group choice.
- Sign flip scenarios, while rare in typical covariate-outcome systems, are not pathological edge cases and can arise in meaningful applications, particularly in highly stratified or narrowly defined subpopulations or when omitted variable bias diverges between groups.
- Analysts should always report results under both reference rules. Blind acceptance of a single reference choice can mislead policy inference and conceptually misallocate sources of disparity.
From a theoretical perspective, this work shows the dangers of assuming that qualitative causal-order interpretation (e.g., "this gap is explained by observed covariates") is robust under standard OBD.
Potential for Future Developments
This analysis confronts the limitations inherent to linear OBD, even under correct model specification. As OBD is extended via more flexible ML-based conditional estimators in high-dimensional or nonlinear settings, the instability identified here may only worsen. This motivates:
- Investigation of reference-invariant or symmetrized decomposition frameworks;
- Formal sensitivity analysis for reference group selection;
- Development of reporting standards that force transparency about reference dependence for regulatory, scientific, and clinical usage;
- Further theoretical work on the geometric/topological characterization of “sensitive” regimes, perhaps leveraging group representation or information-theoretic approaches.
Conclusion
The paper demonstrates that the choice of reference group in the Oaxaca-Blinder decomposition can result in divergent substantive conclusions—specifically, opposite sign attribution of group differences to covariate distributions or group-specific coefficients. Though such reversals are structurally prevalent in the space of possible linear parameterizations, empirical analyses suggest practical rarity due to domain-driven correlations in group-wise parameters. Given this sensitivity, all practitioners using OBD should examine both decompositions and report the full spectrum of possible inferences. The work also provides a foundation for further methodological exploration on the limitations of covariate-based attributions in disparity analysis.

