- The paper presents a progressive diffusion model that integrates spectral and anatomical priors to preserve both global structure and fine details in LDCT denoising.
- It employs three specialized modules—APGC for anatomical conditioning, RFDDS for frequency-specific enhancement, and TD³ for stage-adaptive noise suppression.
- Quantitative and qualitative evaluations on clinical and synthetic datasets demonstrate superior PSNR, SSIM, and preserved diagnostic cues for downstream tasks.
ProSAC-CT: Progressive Spectral-Anatomical Co-Guided Multi-Stage Diffusion for Low-Dose CT Denoising
Introduction
The use of low-dose computed tomography (LDCT) is essential for minimizing patient radiation exposure, particularly in repetitive or screening contexts. However, LDCT images are fundamentally limited by elevated quantum noise, streak artifacts, and texture degradation, which often obscure subtle anatomical structures and boundaries. Preservation of high-fidelity, anatomically-consistent representations through effective denoising is thus critical for both interpretability and downstream computer-aided diagnosis.
Diffusion models present a flexible generative paradigm for LDCT denoising. In spite of recent progress—including methods such as RDDM, I2SB, and CoreDiff—existing approaches typically lack explicit anatomical constraints, exhibit frequency-agnostic recovery, and perform uniform reverse-process modeling, which collectively lead to deficient boundary preservation and potential over-smoothing. "ProSAC-CT: Progressive Spectral-Anatomical Co-Guided Multi-Stage Diffusion Model for Low-Dose CT Denoising" (2607.01756) proposes an architecture that incorporates structural and spectral guidance within a time-step-adaptive diffusion process, achieving superior fidelity and downstream task utility compared to prior methods.
Model Architecture and Methodology
Anatomical-Prior-Guided Conditioning (APGC) Module
APGC introduces explicit anatomical structure into the encoding pipeline via priors derived directly from the LDCT input, eliminating reliance on external data. This module aggregates three branches: global anatomical features from MedDINOv3, coarse structure via the Sobel operator, and fine boundaries via the Laplacian operator. Their learnable aggregation produces an anatomical-edge enhanced feature map (AEFM), injected into the encoder to yield an anatomy-conditioned latent representation.
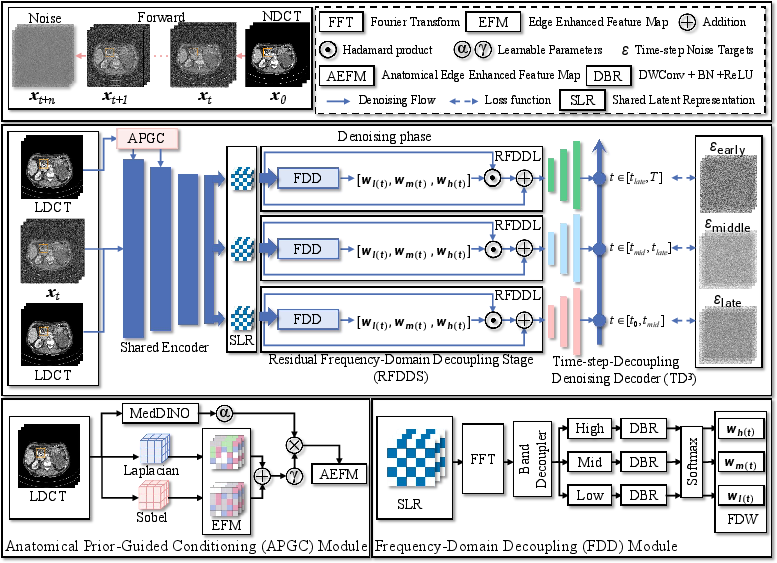
Figure 1: Overall ProSAC-CT architecture integrating anatomical-prior-guided conditioning, residual frequency-domain decoupling, and time-step-decoupling denoising.
Residual Frequency-Domain Decoupling Stage (RFDDS)
RFDDS explicitly disentangles the shared latent representation into low-, middle-, and high-frequency bands using radial frequency masks in the Fourier domain. Each band is reweighted by channel-wise importance metrics generated via lightweight DBR blocks and global average pooling, followed by branch-specific residual enhancement. This design achieves frequency-sensitive denoising, preserving global structure, boundaries, and fine textures in a coordinated manner.
Time-Step-Decoupling Denoising Decoder (TD3)
A key innovation is the division of the reverse diffusion trajectory into early, middle, and late stages, each with its branch-specific decoder. Each stage receives different frequency-enhanced representations tailored by RFDDS. Early-stage denoising focuses on anatomical stabilization, the middle stage on boundary refinement, and the late stage on residual detail consolidation and noise suppression. This time-step-adaptive mechanism matches denoising functions to the evolving needs of the reverse diffusion process, improving both convergence and anatomical fidelity.
Evaluation and Quantitative Results
Data and Experimental Protocol
ProSAC-CT is evaluated across four task-representative benchmarks:
- Mayo-2016 and Mayo-2020: Clinical paired LDCT/NDCT datasets covering both abdominal and thoracic anatomies.
- QIN-Lung and LoDoPaB: Synthetic LDCT degradation via projection and reconstruction processes.
All baselines, including RDDM, RED-CNN, UNAD, DU-GAN, CTformer, AMIR, I2SB, ResShift, and CoreDiff, employ identical preprocessing and a 2.5D three-slice input configuration.
ProSAC-CT demonstrates consistent superiority across metrics, including PSNR, SSIM, FSIM, NQM, and VIF, outperforming strong baselines by robust margins (e.g., >1.7 dB PSNR gain on Mayo datasets; see Table 1 in the paper). Improvements extend across clinical and synthetic settings, indicating strong generalization and data distribution robustness.
Qualitative results (Figure 2, Figure 3) highlight sharper anatomical boundaries, accurate intensity recovery, and minimized residual artifacts—especially around tissue interfaces and low-contrast regions.
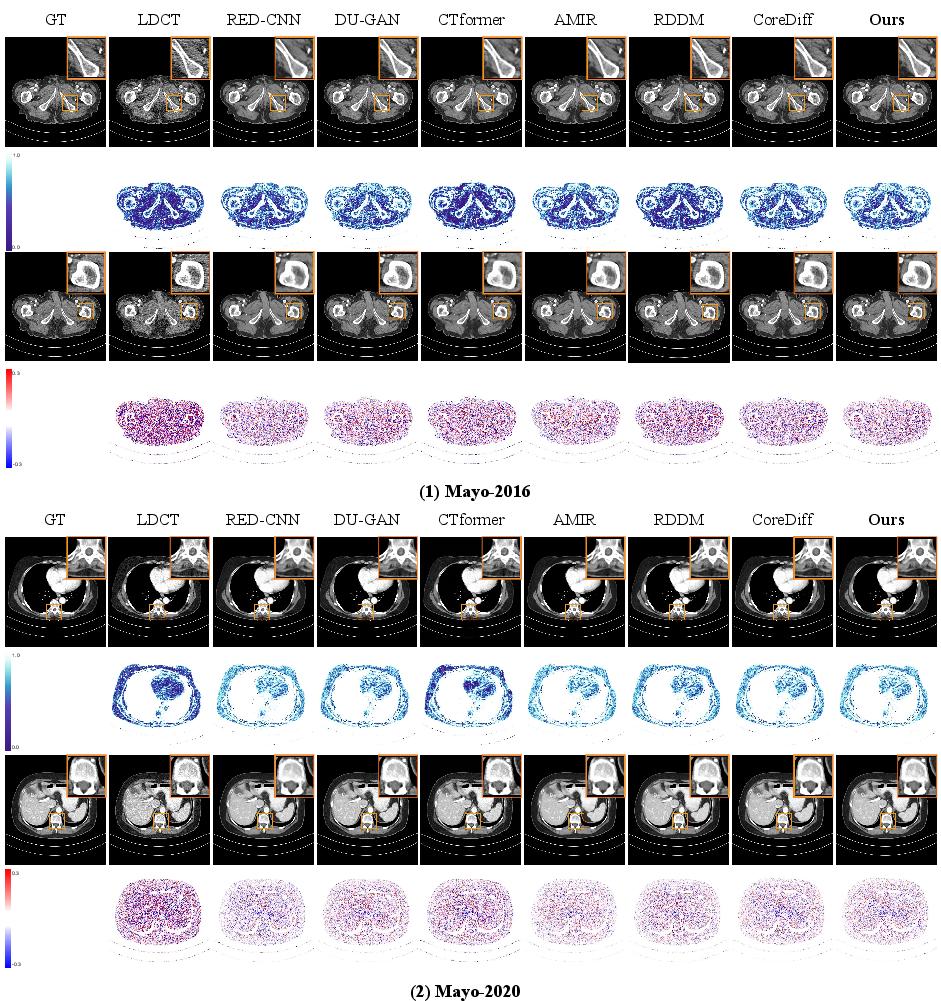
Figure 2: Structural fidelity and residual analysis on Mayo-2016 and Mayo-2020, highlighting preservation of boundaries and reduced error in ProSAC-CT outputs.
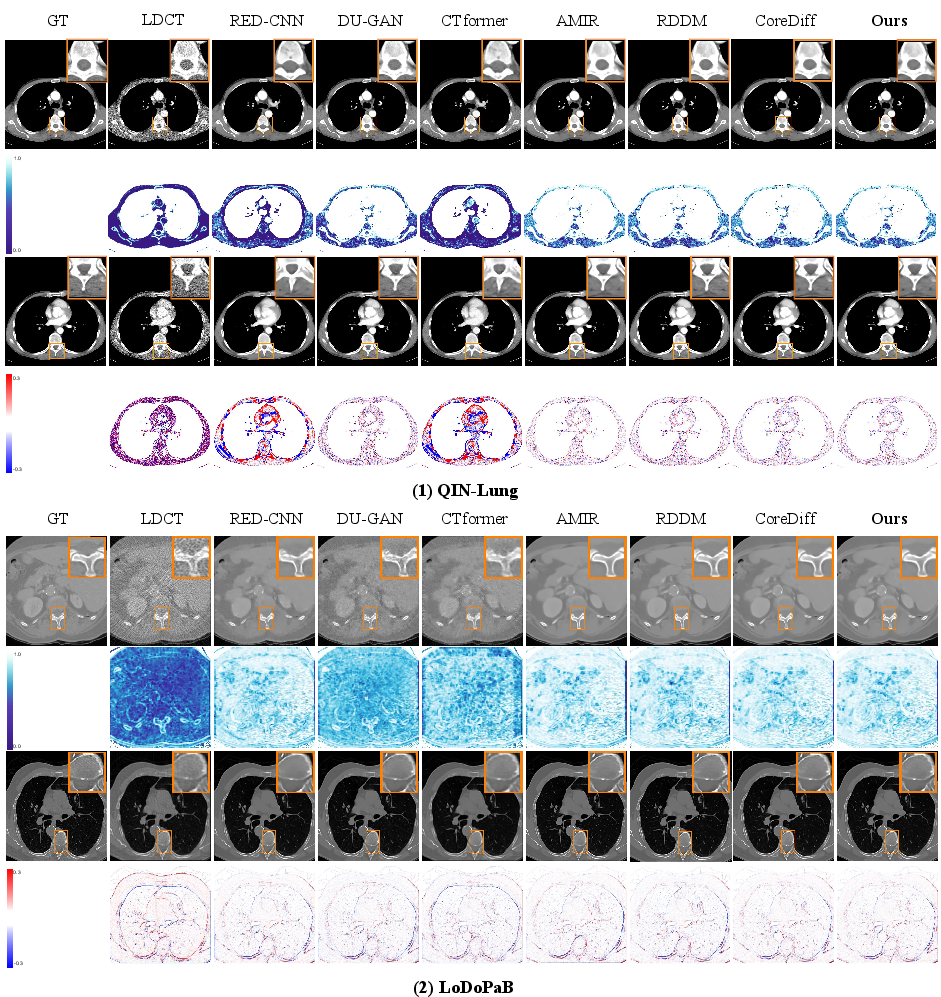
Figure 3: Structural fidelity on QIN-Lung and LoDoPaB, showing robust performance on synthetic degradation scenarios.
Anatomical Prior and Ablative Insights
Figure 4 visualizes the APGC-produced anatomical prior, confirming extraction of high-SNR, spatially-precise contours from severely degraded LDCT data. The anatomical-edge enhanced feature map retains structure cues necessary for conditioning the diffusion process, supporting the claim that leveraging LDCT-intrinsic structure is sufficient for effective priors.
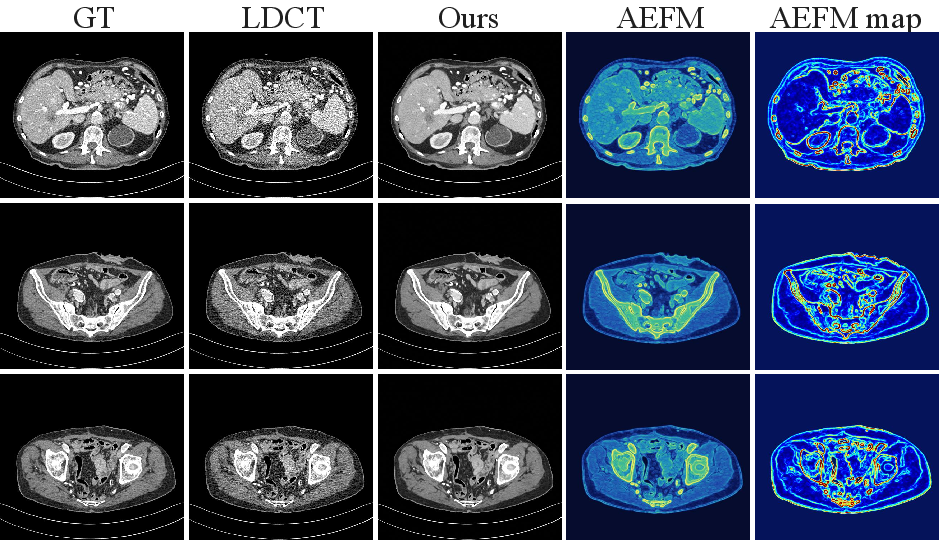
Figure 4: LDCT-derived anatomical prior (AEFM), with strong responses at organ/tissue boundaries even under heavy noise.
Ablation experiments isolate each architectural contribution; APGC yields strong gains in structure and SNR, RFDDS further boosts recovery of frequency-localized features, and TD3 facilitates stage-specific refinement. The complete pipeline consistently achieves optimal denoising across metrics and visually.
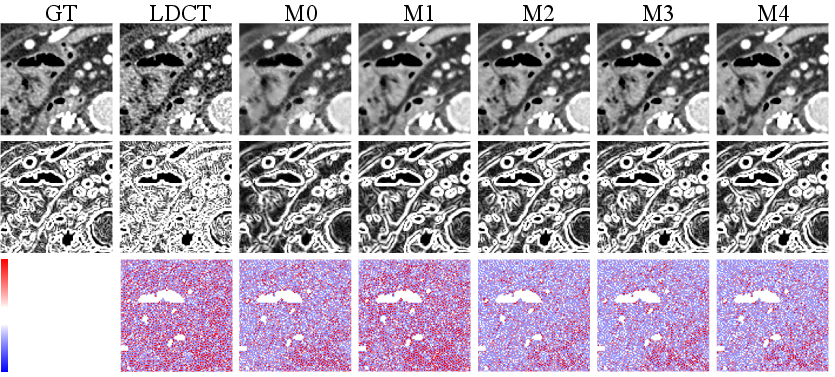
Figure 5: Visual ablation shows progressive recovery with each modular addition, culminating in best structure/detail preservation for ProSAC-CT.
Progressive Denoising and Spectral Analysis
Stage-wise error mapping (Figure 6) and image decomposition (Figure 7) validate a coarse-to-fine error reduction trajectory: global structure and low frequency are stabilized early, boundaries are refined at intermediate stages, and high-frequency textures and noise are addressed late. The spectral error trajectory quantitatively demonstrates reduced magnitude-spectrum discrepancies band-wise at each diffusion stage.
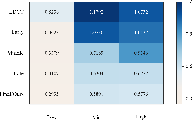
Figure 6: Stage-wise spectral error on Mayo-2016; frequency-specific improvements emerge along the reverse denoising trajectory.
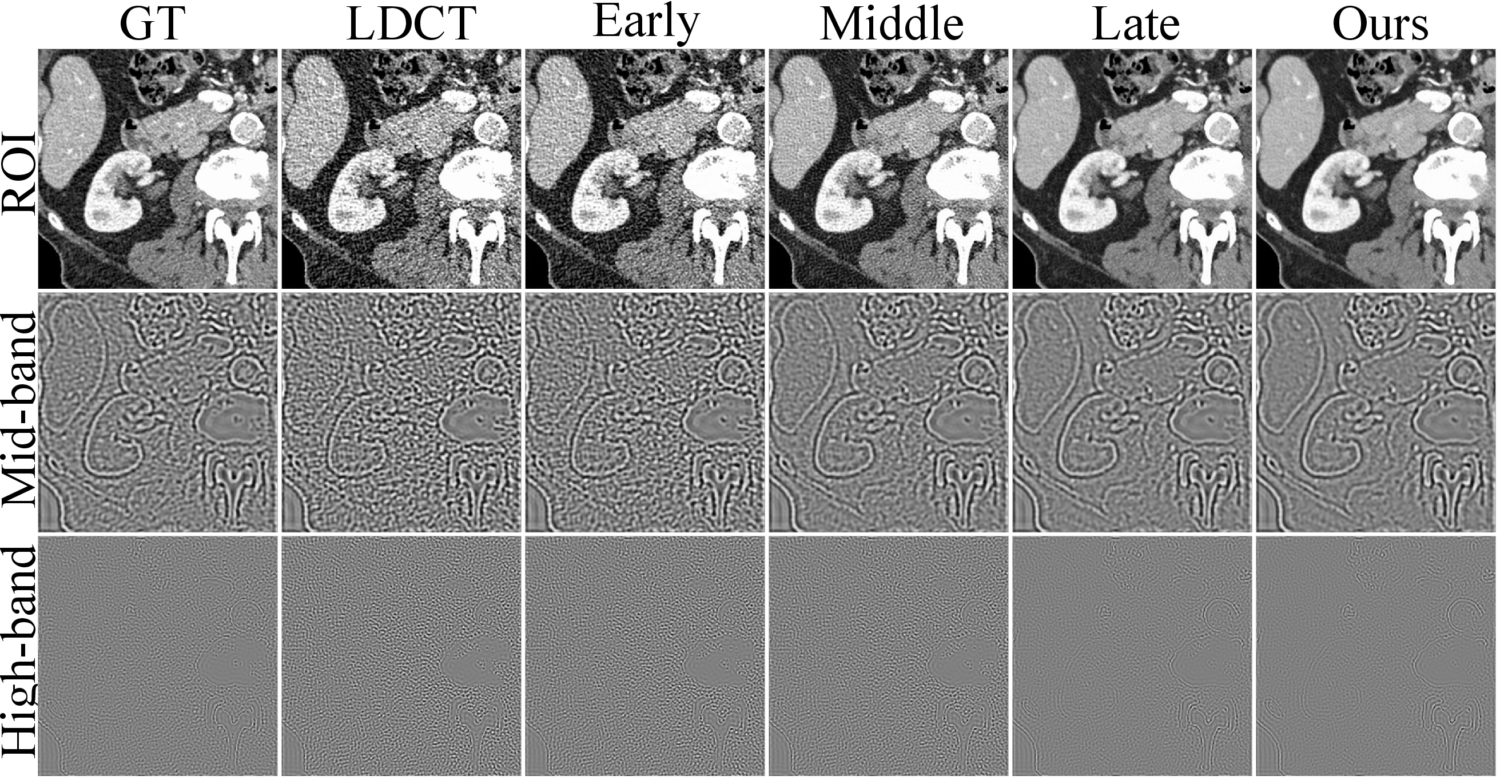
Figure 7: Inverse-FFT decomposition visualizes restoration of middle/high-frequency components at appropriate stages.
Downstream Task Preservation
Superior restoration of anatomy and texture should manifest in preservation of features used by downstream classifiers. Six-class anatomical-region classification on Mayo-2020 demonstrates that ProSAC-CT outputs yield higher F1, balanced accuracy, and AUC on ResNet50, Swin-Tiny, and MambaOut-Tiny compared to all competing denoising methods—with performance approaching that of NDCT. Notably, some visual denoisers (e.g., RED-CNN) underperform raw LDCT in classification, establishing that ProSAC-CT uniquely preserves diagnostic cues essential to subsequent tasks.
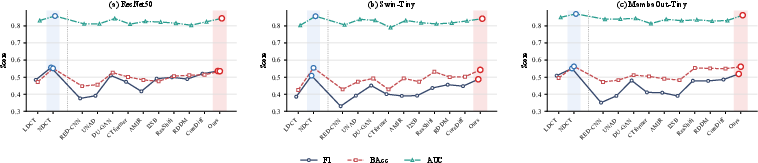
Figure 8: Downstream classification performance (F1, BAcc, AUC) for different denoisers; ProSAC-CT consistently yields the most accurate anatomical recognition.
Implications and Future Directions
ProSAC-CT advances diffusion-based medical image denoising by embedding explicit anatomical and frequency-aware priors in a stage-adaptive, modular framework. The practical effect is noise suppression that does not compromise structure, with direct evidence for conservation of downstream analysis fidelity. Theoretically, this architecture motivates further exploration into fully-conditional, multi-modal generative models for medical imaging that dynamically utilize both spatial priors and frequency-domain decompositions.
Possible extensions include fine-grained temporal adaptation, end-to-end optimization of anatomical priors in a self-supervised fashion, and joint training with downstream analysis networks. Applications readily extend beyond CT to other modalities where structure and frequency separation are paramount (e.g., MRI, PET).
Conclusion
ProSAC-CT integrates conditional anatomical priors, frequency-decomposed residual enhancement, and time-step-adaptive decoding within a diffusion framework for robust LDCT image denoising. The model delivers strong quantitative and qualitative denoising improvements, preserves critical anatomical detail, and retains features necessary for downstream analysis—narrowing the gap between LDCT and NDCT for both clinical and computational workflows. The approach provides a scalable blueprint for future generative models in medical imaging and related high-fidelity, structure-dependent restoration tasks.