- The paper presents a post-training self-supervised temporal regularization strategy that significantly reduces landmark jitter while preserving high spatial segmentation accuracy.
- It employs a hybrid graph-based VAE with a compound loss, integrating Chamfer distance and temporal penalties to ensure anatomically consistent motion.
- The method enables automated AHA regional mapping, yielding clinically relevant insights for regional wall motion and strain analysis in echocardiography.
Self-Supervised Temporal Regularization for Landmark-Based Cardiac Segmentation with Automatic AHA Regional Mapping
Introduction and Motivation
This work addresses key limitations in landmark-based cardiac segmentation, particularly the lack of temporal consistency when models are trained on independent frames. Previous approaches leveraging pixel-based CNN and transformer architectures have demonstrated high spatial accuracy but fall short in anatomical rigor, often yielding segmentations with holes, boundary artifacts, or topology errors. Graph-based methods with implicit anatomical correspondences resolve these spatial issues and enable robust population-wide analyses, but independent-frame training introduces temporal discontinuities in landmark predictions, impairing motion estimation and derived clinical metrics.
The proposed method introduces a post-training self-supervised temporal regularization strategy for graph-based landmark segmentation, targeting the reduction of non-physiological landmark jitter and ensuring temporally smooth motion trajectories consistent with cardiac physiology, without requiring temporally dense manual annotation. Additionally, the method leverages population-level correspondences to facilitate fully automated mapping of landmarks to the standardized 17-segment AHA model for regional wall motion and strain analysis.
Methodology
Implicit Anatomical Correspondence Learning
The segmentation backbone is a hybrid graph-based VAE (Mask-HybridGNet Dual), which is trained on pixel-wise segmentation masks using a compound loss function combining Chamfer distance for shape alignment, regularizations for edge length, uniformity, elasticity, curvature, and standard VAE KL-divergence, along with an auxiliary pixel-level Dice loss. Learned landmark correspondences are consistent across patients due to training on a common anatomical atlas, enabling downstream analyses requiring anatomical repeatability.
Temporal Regularization Objective
Temporal smoothness is imposed as a post-training refinement stage. Landmark velocity and acceleration discontinuities across cardiac cycles are penalized via two regularizers:
- Velocity regularization: Penalizes large landmark displacements between consecutive frames.
- Acceleration regularization: Penalizes abrupt velocity changes, enforcing adherence to physiologically plausible acceleration profiles.
These temporal penalties are optimized alongside the original spatial losses in an alternating scheme: batches of single annotated frames reinforce spatial fidelity, interleaved with batches of full sequences reinforcing temporal coherence. Fine-tuning leverages unlabeled image sequences, as the supervisory signal emerges self-supervised from the predicted landmark motion.
Automated AHA Regional Mapping
Implicit correspondences facilitate a reproducible mapping from learned landmarks to AHA segments. The procedure, executed once per view and applied universally, involves:
- Atlas construction from population mean landmark coordinates at end-diastole.
- Identification and division of the long-axis into basal, mid, apical levels, and circumferentially bisected for wall separation.
- Assignment of each landmark to an AHA segment based on spatial proximity.
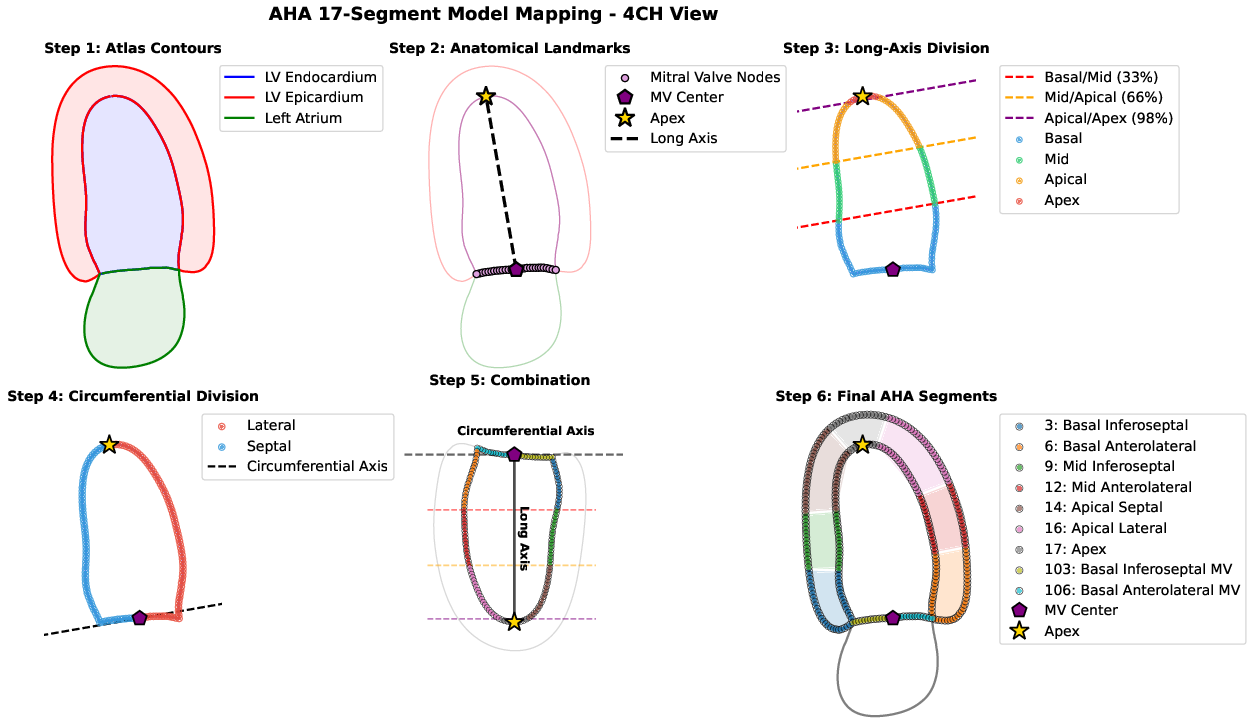
Figure 1: Stepwise atlas-based process for automatic mapping of landmarks to AHA segments using learned population correspondences.
Experimental Validation
Setup and Metrics
Performance is evaluated on the CAMUS echocardiography dataset using spatial (Dice, HD95), clinical (MAE for EF, EDV, ESV), and three trajectory-based temporal coherence metrics: jitter (RMS error between trajectory and its low-pass filtered version), FTD (average inter-frame node excursion), and jerk (RMS third-order finite difference as a measure of smoothness).
Comparative Results
Baseline Mask-HybridGNet Dual models trained without temporal regularization yield high Dice and low HD95, on par with state-of-the-art CNN (nnUNet). However, these baseline models exhibit temporal artifacts and discontinuities in landmark trajectories, resulting in elevated jitter and jerk scores.
Temporal regularization (Mask-HybridGNet Dual + Temp. Reg. w/o Raster) significantly reduces jitter, FTD, and jerk, evidenced by boxplot summaries across all test patients.
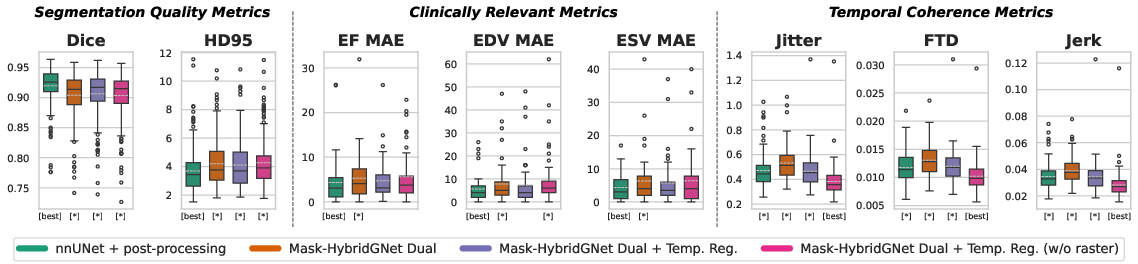
Figure 2: Distribution of segmentation accuracy (Dice, HD95), clinical metrics (EF, EDV, ESV MAE), and trajectory smoothness (Jitter, FTD, Jerk) across methods, highlighting pronounced gains in temporal quality for temporally regularized GraphNet models.
The nnUNet, even with post hoc landmark recovery from segmentation masks, does not match the temporal consistency of regularized graph-based methods, due to lacking explicit spatial-temporal coupling and anatomical correspondence.
Clinical and Qualitative Analysis
Applying the AHA mapping procedure enables consistent regional wall motion and strain quantification. Temporally regularized predictions yield smoother segment centroid trajectories and more regular longitudinal displacement curves, both in patients with normal ejection fraction and those with reduced function, specifically improving analysis in wall motion abnormality detection.
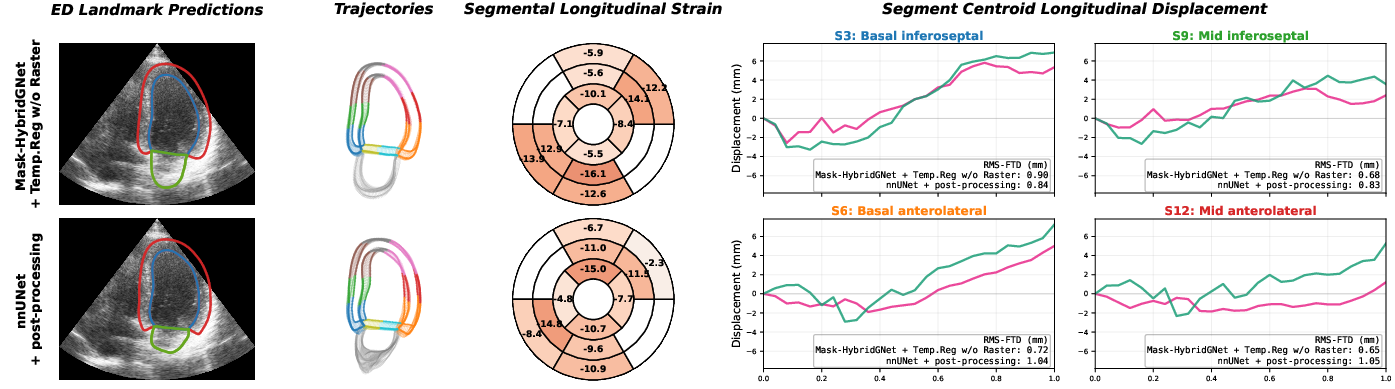
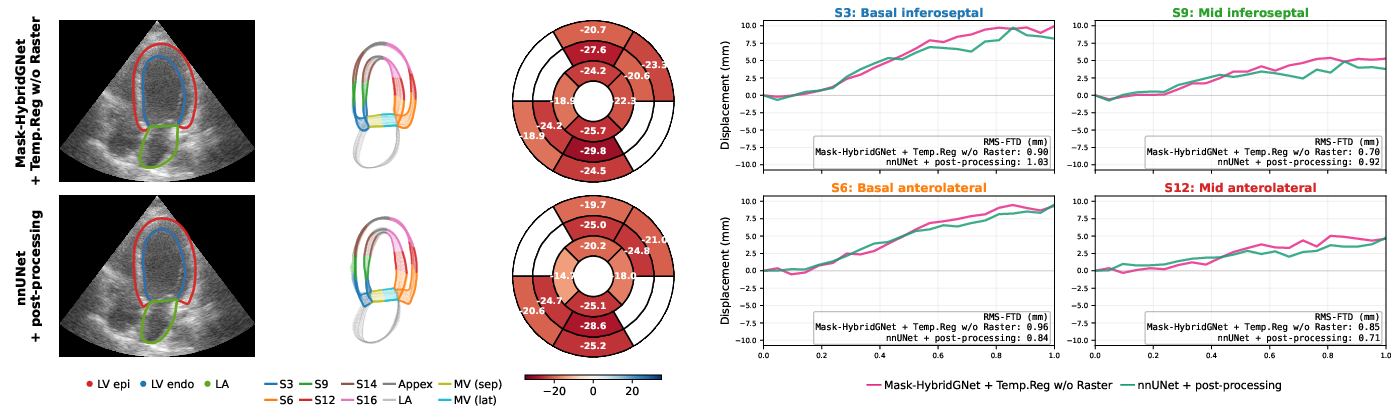
Figure 3: Regional motion and strain trajectories for two cases (low and normal EF), comparing Mask-HybridGNet + Temp.Reg. and nnUNet post-processing; regularized pipeline produces smoother, physiologically congruent curves, especially at left atrial boundaries.
Discussion
Empirical findings reveal that spatial segmentation accuracy, even at high Dice scores, is insufficient for applications needing temporally consistent outputs such as volumetric cardiac functional analysis and regional motion assessment. The proposed post-training self-supervised regularization substantially boosts temporal regularity of landmark trajectories without degrading anatomical or clinical performance, outperforming post-processing approaches applied to pixel-based segmenters. Notably, the automatic AHA regional mapping leverages the strength of population-learned correspondences, providing direct clinical interpretability and facilitating downstream quantitative tasks (e.g., regional strain estimation) that are otherwise error-prone with independently segmented frames or methods lacking explicit correspondence.
Theoretical and Practical Implications
The method demonstrates how self-supervised learning can meaningfully regularize temporal dynamics in structured output spaces (anatomical graphs) without sacrificing spatial fidelity. By not requiring fully annotated sequences, the approach is scalable and extensible to other dynamic segmentation tasks. In practice, automated, robust, and regionally standardized analysis pipelines offer direct routes toward large-scale quantitative studies and AI-assisted diagnostics in echocardiography.
Future directions may include integration of biomechanical constraints, extension to 3D/4D acquisitions, and unification with transformers for improved sequence modeling. Explicit quantification of clinical end-points in larger, more pathological cohorts and adaptation to other imaging modalities are natural next steps.
Conclusion
This work establishes an effective post-training regularization mechanism for enforcing physiologically consistent landmark motion, producing temporally smooth, anatomically corresponded cardiac segmentations that can be automatically and reproducibly mapped to the AHA framework. The approach substantially improves downstream clinical utility and sets a principled pathway for generalizing temporally consistent segmentation in other biomedical video analysis domains.