- The paper introduces GlyLLM, a framework that fuses static metadata and continuous sensor signals via a multimodal LLM for enhanced glycemic forecasting and diabetes staging.
- It leverages a ViT-based sensor encoder and LoRA-adapted LLM to achieve notable improvements in RMSE, MAE, and AUROC compared to traditional ML models.
- Ablation studies underscore the critical impact of diabetes survey and biometric data in boosting prediction accuracy and risk stratification.
LLM-Powered Personalized Glycemic Assessment in Type 2 Diabetes with Wearable Sensor Data
Introduction
The manuscript presents GlyLLM, a LLM-powered framework for personalized glycemic assessment in type 2 diabetes (T2D), leveraging both static metadata and multimodal wearable sensor signals. It addresses the limitations of established ML approaches, especially their constrained integration of individual-level context and sensor heterogeneity. The proposed GlyLLM framework exploits LLMs’ inherent sequential and multimodal abstraction capabilities to fuse static metadata and real-time continuous glucose monitoring (CGM) with auxiliary sensor streams for advanced glycemic forecasting and diabetes categorization.
Framework Architecture and Integration Paradigm
GlyLLM constitutes a multimodal architecture, where textual embeddings of static metadata (demographics, diabetes survey responses, and biometric assays) and sensor data embeddings produced via a patched Vision Transformer (ViT) encoder are concatenated alongside task-specific instruction prompts. These sequential representations enter the backbone LLM, fine-tuned using parameter-efficient low-rank adaptation (LoRA). The architecture enables rich cross-modal attention and interaction modeling over both immediate temporal sensor dynamics and longer-term individual attributes.
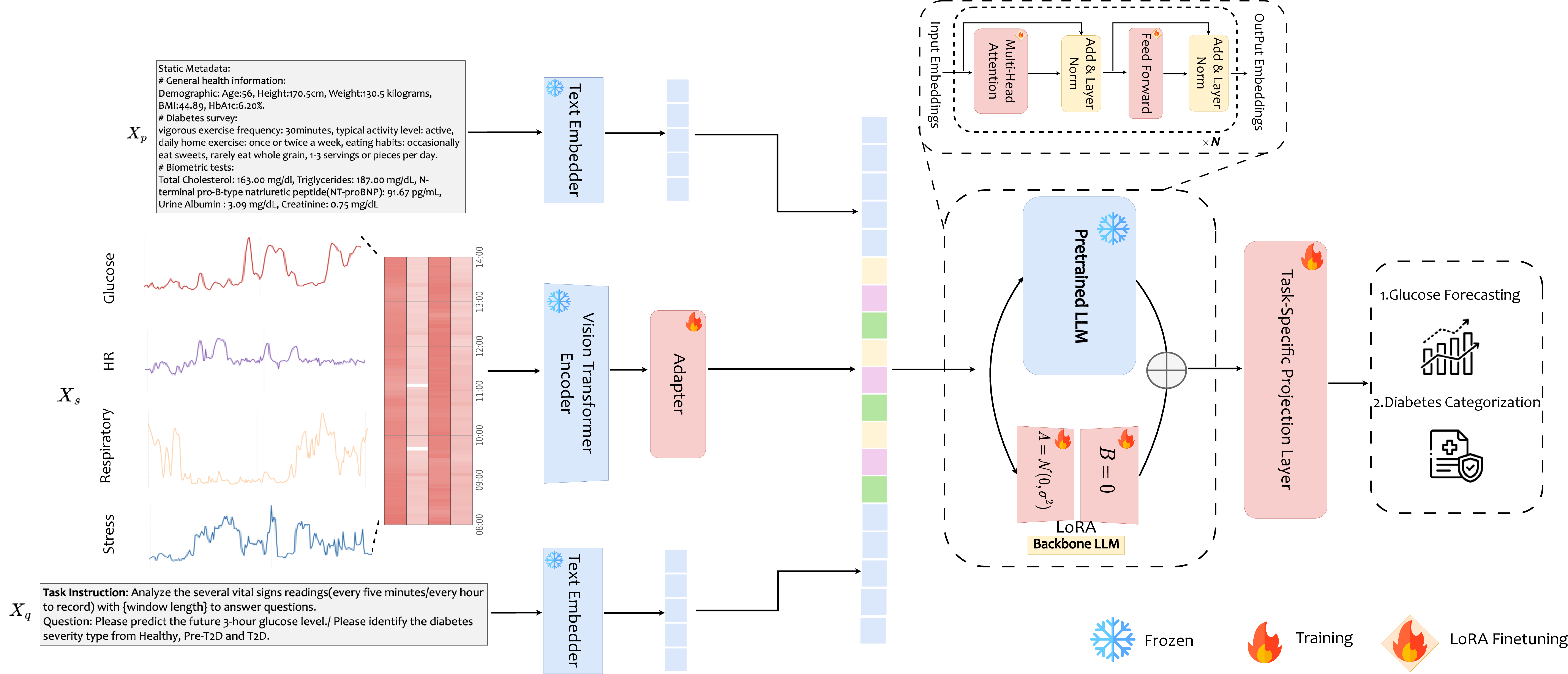
Figure 1: GlyLLM architecture integrates textual metadata, ViT-encoded sensor patch streams, and task instructions for sequential LLM analysis.
Unlike prior template-based prompting paradigms, GlyLLM harnesses a sensor-domain encoder to produce meaningful sensor abstractions, followed by an MLP adapter aligning sensor features with the LLM latent space. The framework’s output head is task-adaptive, supporting both regression (glucose trajectory forecasting) and classification (diabetes group identification).
Static Metadata and Sensor Data Contextualization
Static metadata are structured into three domains: general health indices (GHI: age, BMI, HbA1c), diabetes survey replies (DS: lifestyle, diet), and comprehensive biometric panels (Bio: blood, urine markers). Sensor streams encompass CGM readings, heart rate, respiratory rate, and HRV-derived stress indices at unified five-minute intervals. Personalized prompt templates unify these modalities and task goals, instructing the LLM to deliver individualized analysis per cohort and time window.
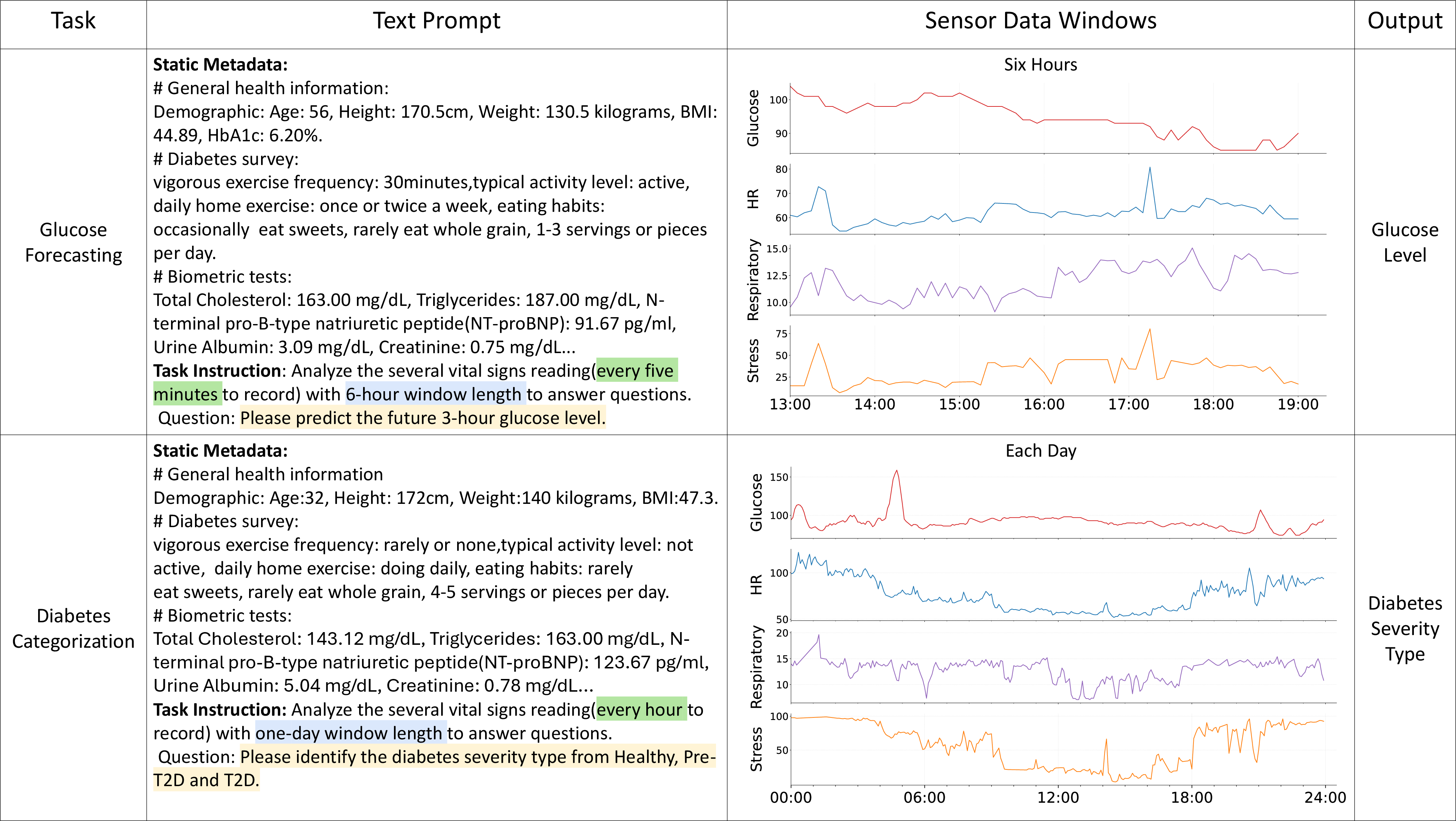
Figure 2: Example prompt template compositions and sensor patch input streams for glucose prediction and categorization tasks.
Experimental Protocol and Baseline Comparisons
Empirical evaluation adopts AI-READI v2.0.0, a population-scale T2D dataset with granular sensor and metadata tracks. Tasks reflect clinical decision needs: (1) glucose forecasting (6-hour window, 3-hour prediction) and (2) diabetes categorization (24-hour window). Baselines comprise both transformer-based multivariate forecasting models (PatchTST, Crossformer, iTransformer) and ML-based classifiers (MLP, LSTM), as well as zero-shot and few-shot LLM prompting schemes.
Numerical Results
Glucose Forecasting
GlyLLM outperforms baselines across all participant strata, with improvements in RMSE (average gain: 13.66%), MAE, and CGM-derived composite iGlu-CE (average gain: 19.81% for Llama3-Med42-8B backbone). Traditional prompting-based LLMs exhibit suboptimal semantic abstraction for long-horizon sensor contexts, yielding unreliable numeric outputs.
Diabetes Categorization
Macro-AUROC is improved by an average of 13.08% (Llama3-Med42-8B), with accuracy, sensitivity, and specificity substantively elevated relative to both ML classifiers and prompting-only LLMs. GlyLLM demonstrates enhanced detection consistency across healthy, pre-T2D, and T2D classes, suggesting improved risk stratification and stage discrimination.
Ablation Study
The removal of either static metadata or sensor data substantially degrades forecasting RMSE and categorization AUROC. Further, omission of DS or Bio metadata yields more pronounced reductions in discriminative accuracy versus GHI, indicating that diabetes-relevant prior information (survey and biometrics) is more salient for glycemic assessment than broad demographic features.
Implications and Theoretical Perspectives
GlyLLM marks a shift toward LLM-based multimodal fusion for clinical time-series modeling, surpassing both classical ML and prompt-based LLM paradigms in integration and semantic abstraction. The critical role of specialized sensor domain encoders, coupled with parameter-efficient LLM adaptation, signals the need for modality-specific pretraining and fine-tuning at the clinical edge. The ablation results reinforce the theoretical importance of cross-modal contextualization, suggesting future designs should prioritize the integration of domain-relevant priors and comprehensive biophysical sensor streams for expanded phenotype prediction.
Practical Outlook and Future Directions
Practically, GlyLLM could provide clinicians with actionable real-time glycemic risk assessments and longitudinal diabetes staging, optimizing interventions for diverse T2D populations. The framework is extensible to additional modalities, such as ECG or retinal imaging, and could leverage broader foundation models to enhance temporal dynamics modeling. Expansion of domain-specific sensor encoders and fusion strategies will likely yield further gains in robustness and clinical validity. Direct clinical validation in real-world settings, cross-dataset generalization, and multi-modal expansion constitute essential future steps.
Conclusion
GlyLLM delivers an effective multimodal LLM framework for personalized glycemic assessment in T2D, achieving significant improvements in both continuous glucose forecasting and diabetes categorization. The architectural innovations in metadata-sensor fusion and LoRA-based LLM adaptation evidence the necessity of specialized cross-modal modeling for real-world medical time-series analysis, setting the stage for more sophisticated AI-empowered clinical tools in diabetes care.

