- The paper introduces GlucoFM-Bench, a standardized benchmark to evaluate TSFMs for blood glucose forecasting across diverse CGM datasets.
- It demonstrates strong zero-shot and few-shot transfer capabilities, with TSFMs nearing the performance of traditional LSTM models in clinical settings.
- The study highlights challenges in extreme glycemic ranges and calibration, emphasizing the need for robust adaptation methods in diabetes management.
Benchmarking TSFMs for Glucose Forecasting: An Expert Analysis of GlucoFM-Bench
Motivation and Problem Scope
Glucose forecasting is a central problem in diabetes management, directly impacting the operation of automated insulin delivery systems and real-time risk assessment for hypo- or hyperglycemic events. Existing predictive models, ranging from traditional statistical to modern deep learning (RNNs, LSTMs, Transformers), face significant limitations in transferability and robustness across populations and datasets. Recent advances in time-series foundation models (TSFMs) have enabled zero- and few-shot transfer on generic forecasting tasks, but systematic benchmarking in health-critical, high-variability domains such as blood glucose dynamics remains lacking.
GlucoFM-Bench addresses this gap by providing a standardized, reproducible, multi-dataset benchmark for evaluating TSFMs, LLM-based forecasting models, and representative supervised DL baselines on blood glucose forecasting tasks. The benchmark covers heterogeneous cohorts across diabetes phenotypes, varied glycemic control, and demographic attributes, establishing a rigorous setting for probing generalization, adaptation efficiency, and clinical relevance.
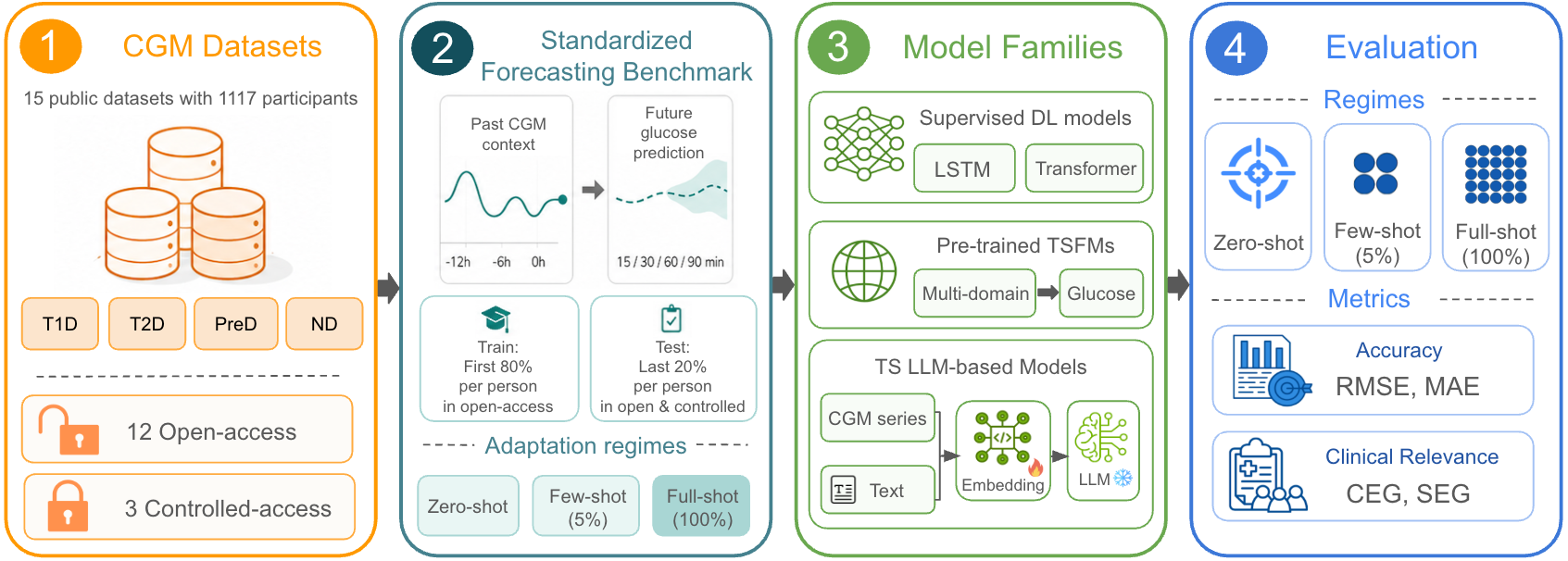
Figure 1: Overview of GlucoFM-Bench, including datasets, models, and evaluation protocols leveraged for glucose forecasting.
Dataset Curation and Preprocessing
GlucoFM-Bench aggregates 15 continuous glucose monitoring (CGM) datasets (12 open-access, 3 controlled-access), spanning over 1,100 individuals with type 1 diabetes (T1D), type 2 diabetes (T2D), prediabetes (PreD), and no diabetes (ND). These datasets collectively represent over 2.8 million CGM records, with sampling frequencies harmonized to 5 minutes. Data preprocessing includes upsampling/downsampling, linear interpolation for short missing gaps, and strict regime for handling longer gaps to maintain sequence integrity. Cohort diversity with respect to metabolic phenotype, age, and glycemic dynamics was preserved (see cohort stratification tables in the Supplement).
The standardized forecasting task uses sliding windows with context lengths up to 24 hours and prediction horizons of 15-90 minutes. Chronological splits (80/20) are applied per participant, maximizing temporal coverage within and across cohorts.
Model Selection and Evaluation Protocols
Eight models were included:
- Supervised DL Models: LSTM (Martinsson et al. [Martinsson2019]), GPFormer (Zhu et al. [Zhu2025])
- Pretrained TSFMs: Chronos-2, Moirai 2.0, Timer, TimesFM v2.5
- LLM-based Forecasting: TimeLLM (Jin et al. [Jin2023timellm]), CALF (Liu et al. [Liu2024calf])
- Persistence Baseline: Last-value repeat
Evaluation comprises zero-shot (direct transfer), few-shot (5% fine-tuning), and full-shot (complete training set) settings. Metrics include RMSE, MAE, and two clinical error grids: Clarke Error Grid (CEG) and Surveillance Error Grid (SEG).
Main Results and Model Comparisons
Zero-shot Transfer: TSFMs vs. Baseline
Pretrained TSFMs demonstrate strong zero-shot transfer, with TimesFM v2.5 achieving average RMSE within 4.3% of the full-shot LSTM model—the best zero-shot RMSE was 18.75 mg/dL (SEG no-risk 88.59%), compared to a 22.25 mg/dL baseline. Chronos-2 and Moirai 2.0 rank closely behind. Timer lags, indicating architectural effects on transfer. Notably, high external validity is confirmed on challenging controlled-access test sets (OhioT1DM, DiaTrend, T1DEXI).
Few-shot Adaptation and Data Efficiency
Few-shot fine-tuning closes the gap between TSFMs and supervised baselines: TimesFM surpasses all others on open-access sets (RMSE 15.20 mg/dL), Chronos-2 yields the best external set performance. The LSTM baseline remains highly competitive under few-shot, confirming that domain-specific inductive biases retain value with limited task data.
Full-shot: Revisiting Task-specific DL
With abundant data, the LSTM achieves the lowest overall RMSE (17.97 mg/dL), outperforming TSFMs by 4–21% depending on dataset and metric (statistically significant; see pairwise Wilcoxon tests in the Appendix). This pattern confirms the lack of consistent scaling advantage for foundation models in high-data regimes for this domain; model design and adaptation mechanisms are decisive.
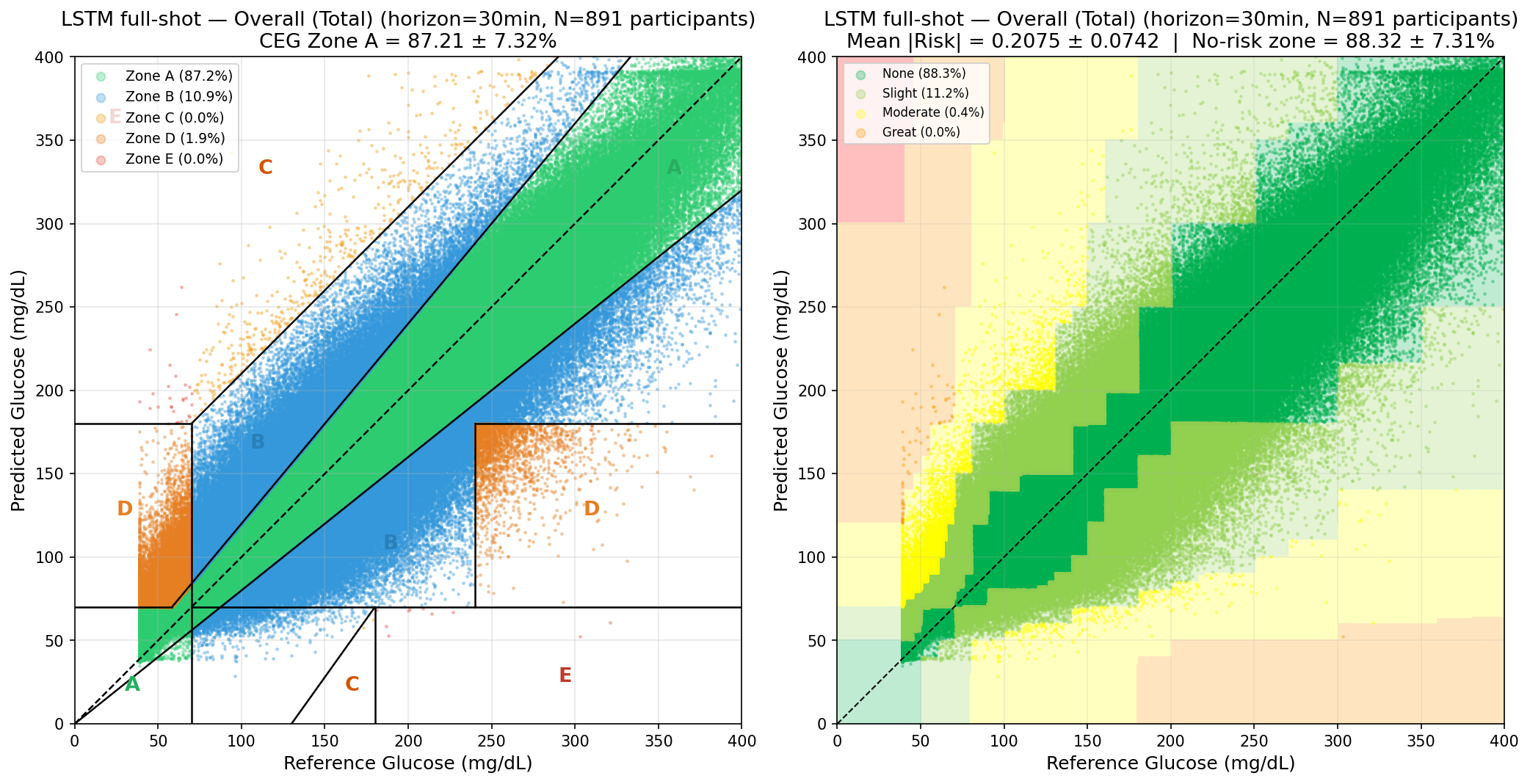
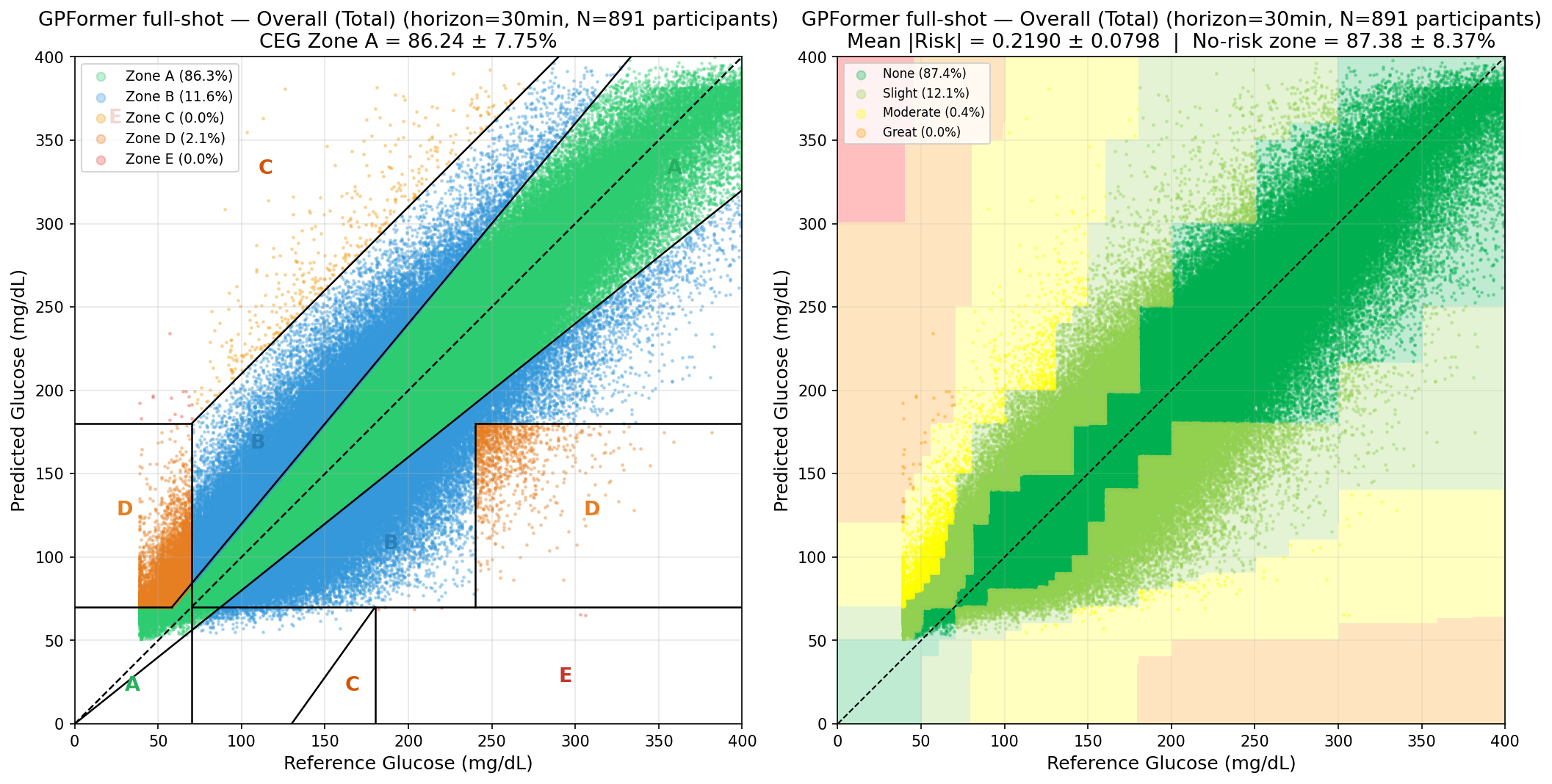
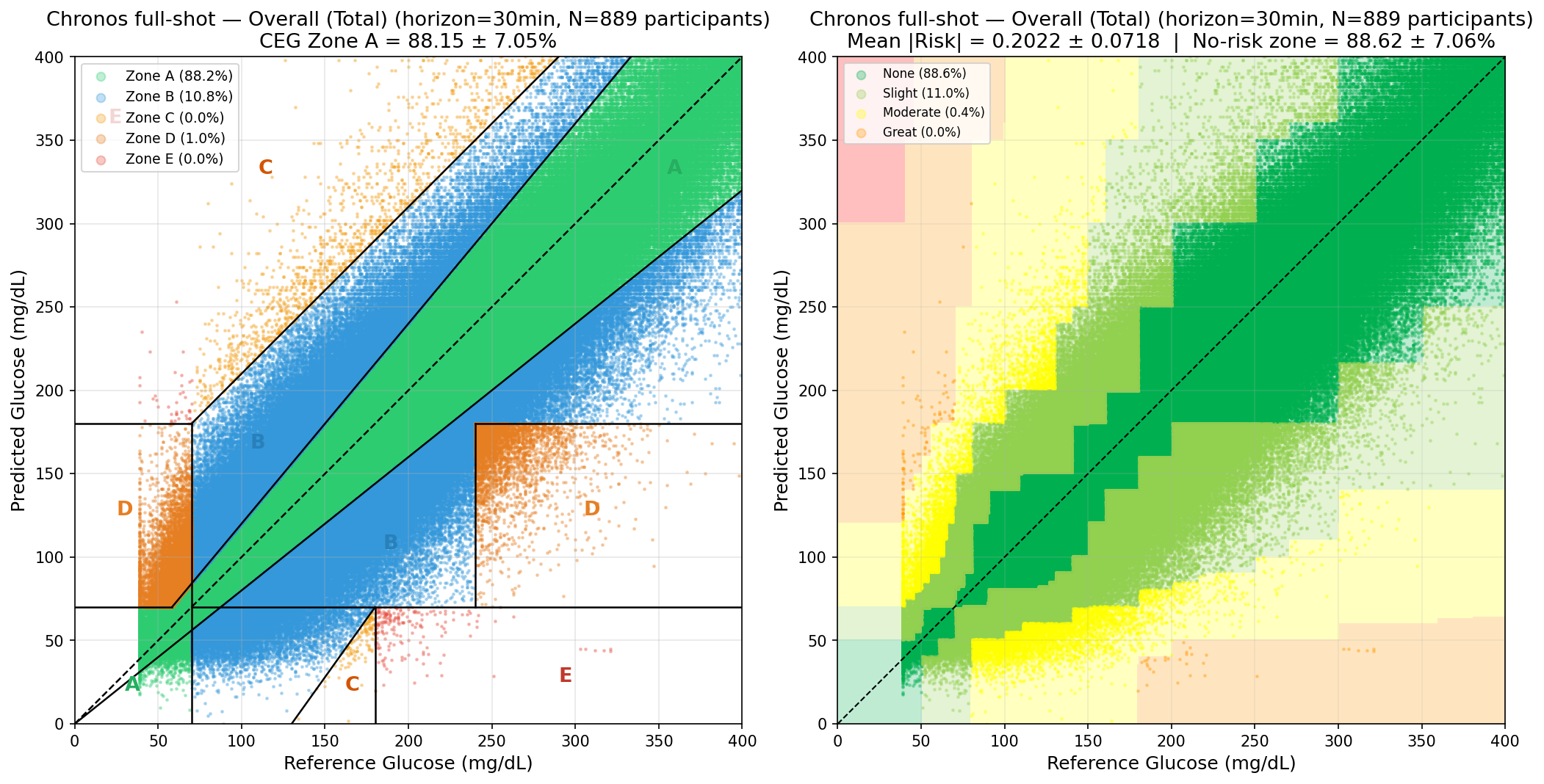
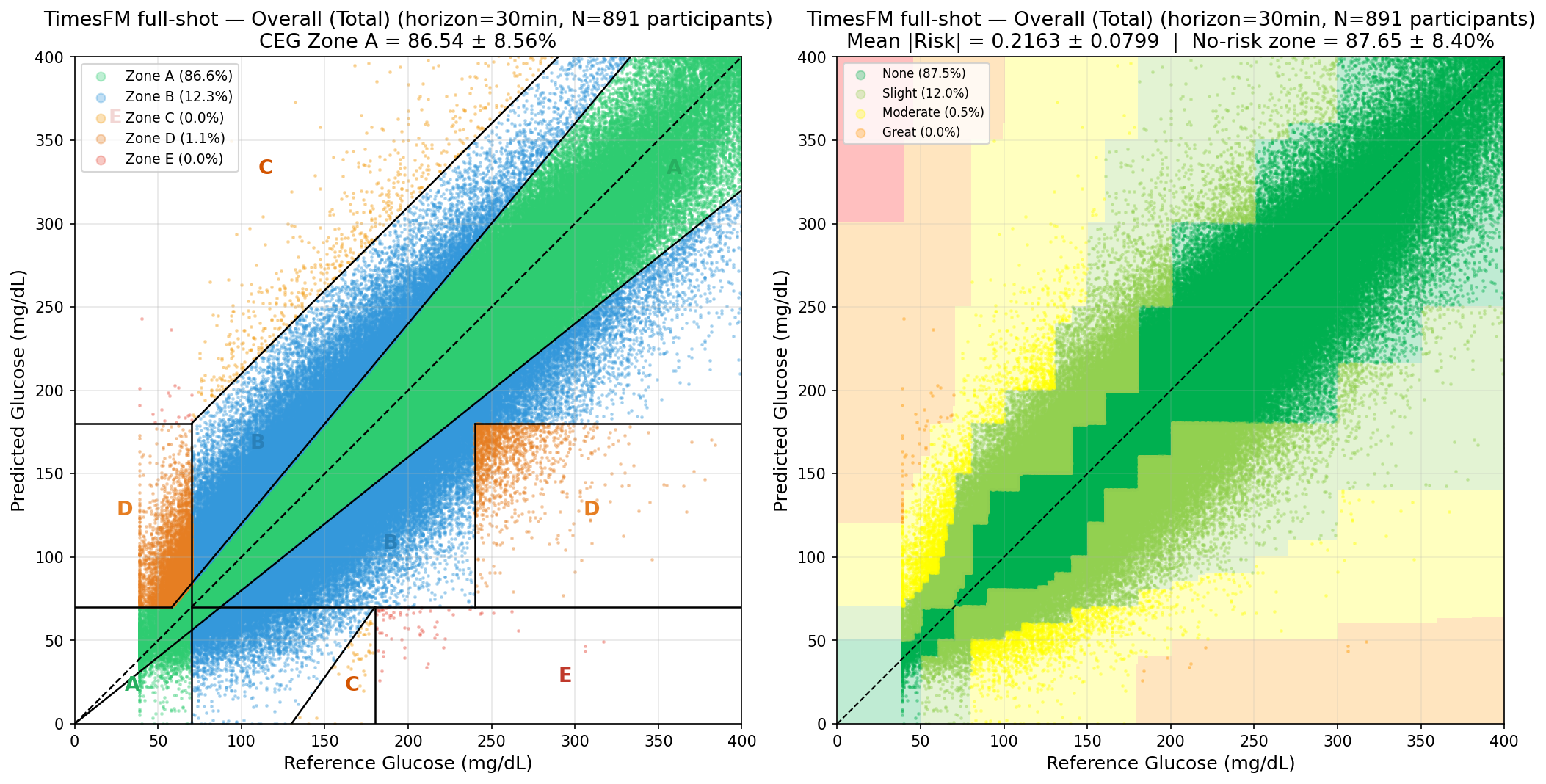
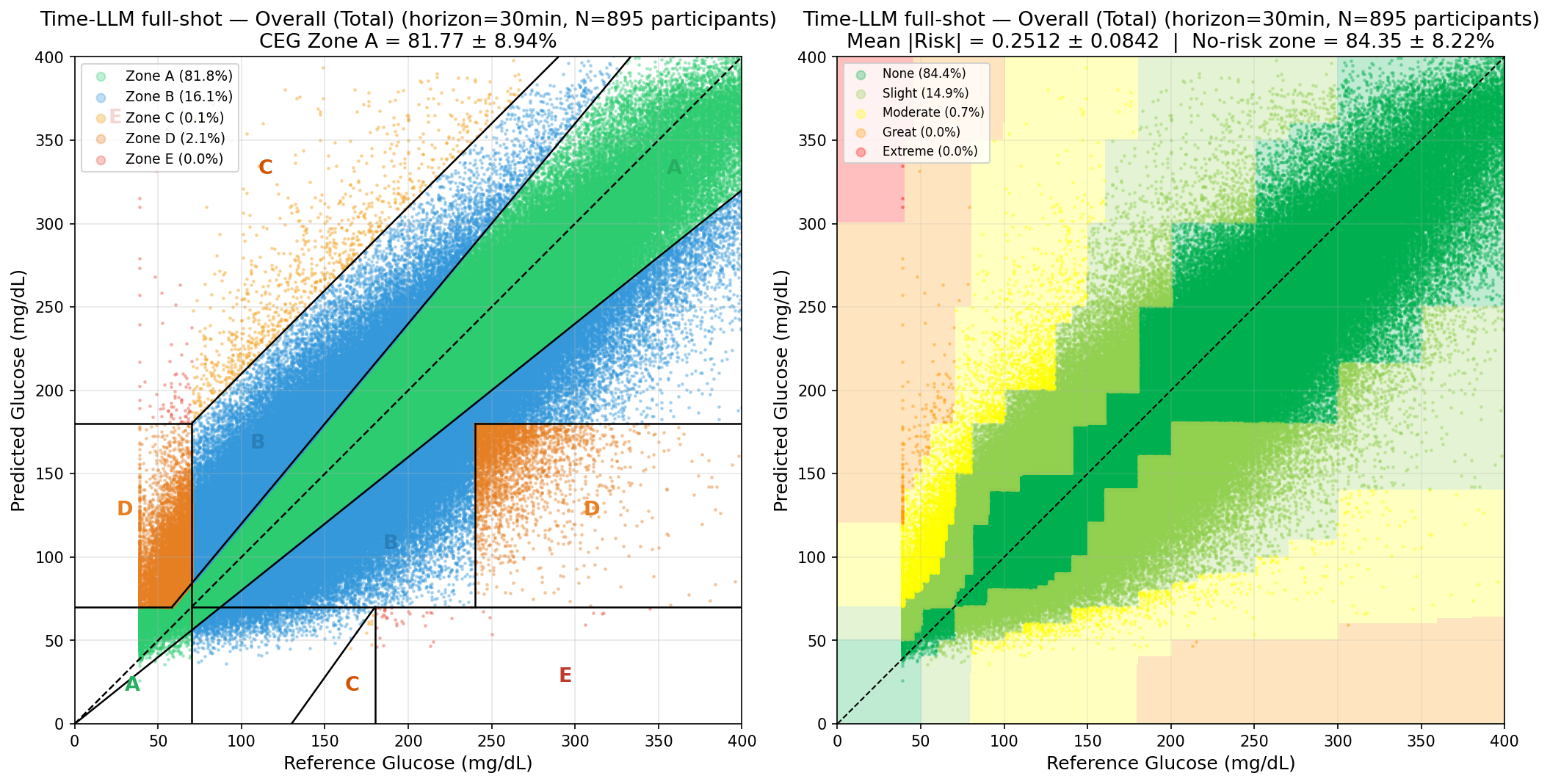
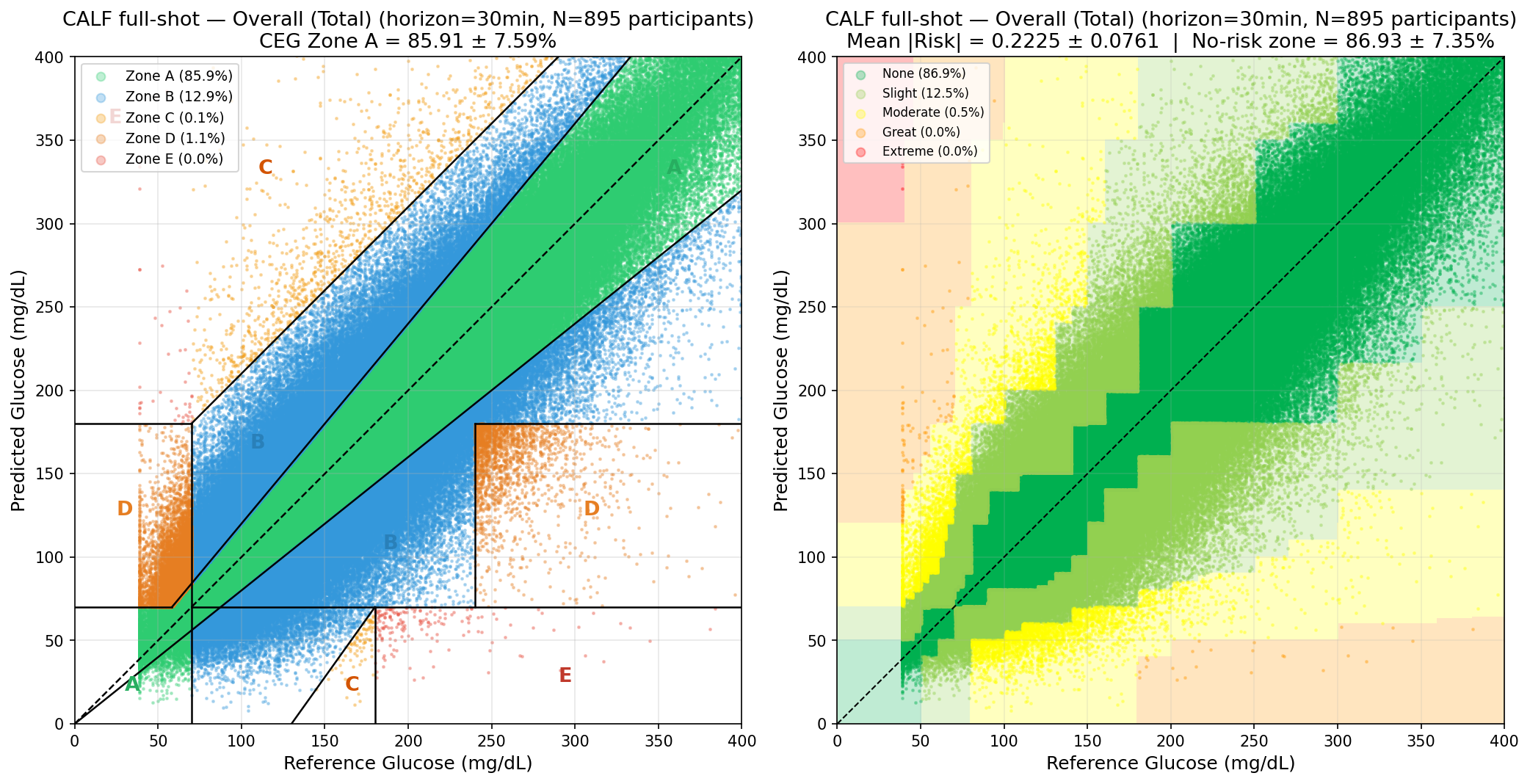
Figure 3: LSTM performance is strongest under full-shot (high-data) regimes.
Context Length Sensitivity and Output Horizons
Analysis of context window length reveals robust TSFM zero-shot performance across 1–24h contexts, optimal at 12h (Figure 4), balancing accuracy and data efficiency. Across all models, RMSE increases with prediction horizon, reflecting the intrinsic stochasticity of glycemic trends outside short intervals.
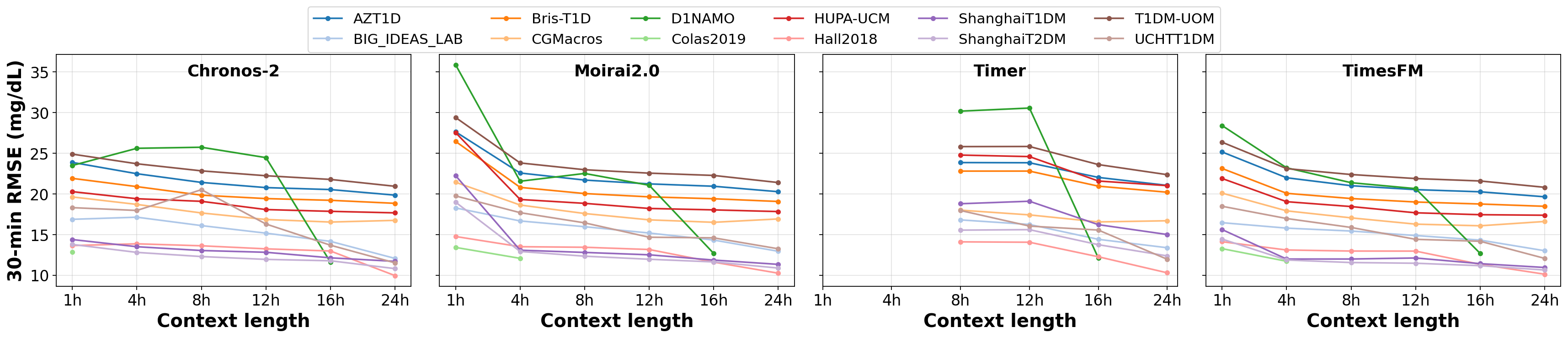
Figure 4: Zero-shot evaluation of pre-trained TSFMs on different context lengths.
Stratified Analyses: Glycemic Range and Cohort Effects
Model performance degrades significantly in hypoglycemic (<70 mg/dL) and hyperglycemic (>180 mg/dL) ranges compared to euglycemic values, with TSFMs outperforming others in sparsely represented hypoglycemic ranges (Figure 3 below). T1D subjects consistently show higher RMSE due to increased underlying glycemic variability. Data imbalance (hypoglycemic points <2.5% of records) accentuates these challenges and highlights the need for focused adaptation and uncertainty quantification in critical ranges.
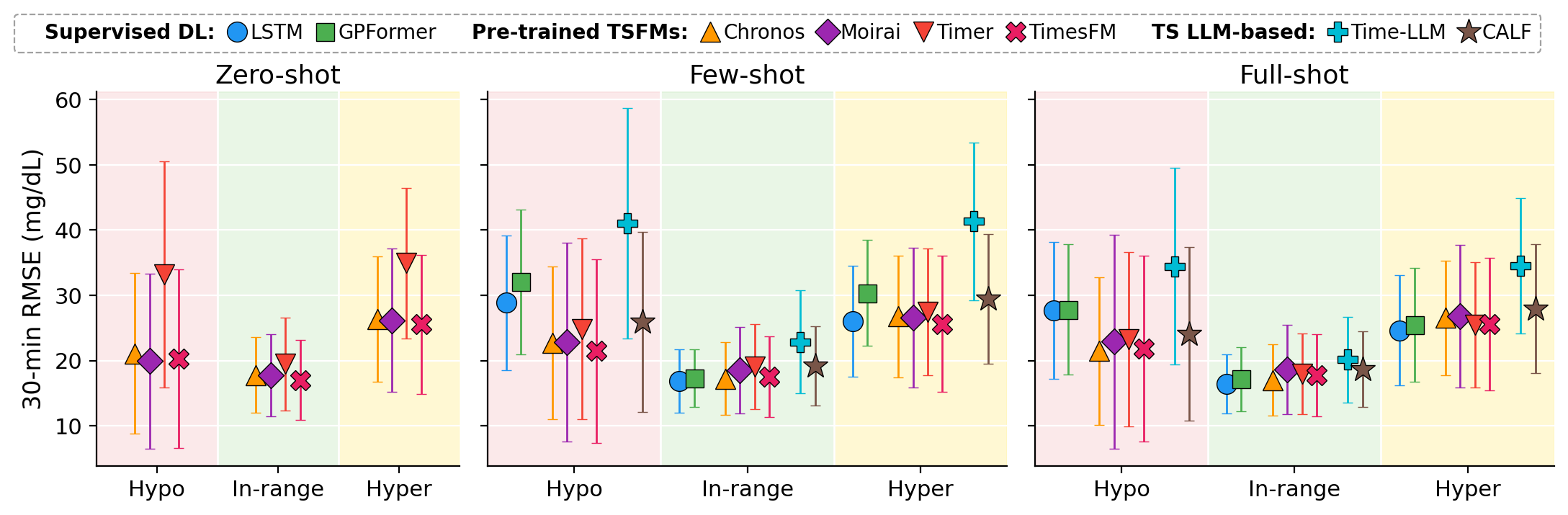
Figure 3: Glycemic-stratified 30-minute RMSE for zero-, few-, and full-shot protocols, showing persistent challenges in clinical extremes.
Model Calibration and Probabilistic Forecasting
TSFMs supporting probabilistic prediction (Chronos-2, Moirai2.0, TimesFM) demonstrate stable interval coverage in zero-shot mode (PI80 close to nominal 80%), but calibration degrades for Moirai2.0 and TimesFM post-fine-tuning—a potential consequence of catastrophic forgetting in high-capacity, sparsely updated models, as suggested in [gupta2024].
Limitations
GlucoFM-Bench exclusively evaluates univariate glucose prediction; multivariate forecasting with auxiliary signals (insulin, carbs, physical activity) awaits broader public dataset availability and increased TSFM multivariate support. Benchmark coverage is not exhaustive of all TSFM/LLM variants, but incorporates representative architectural families, settings, and metrics.
Practical and Theoretical Implications
Transferability and Clinical Deployment: The strong zero-/few-shot transfer of general-purpose TSFMs demonstrates practical readiness for rapid deployment to new cohorts and centers—particularly where task-specific data is sparse, a prevalent scenario in clinical rollouts and rare phenotypes. However, the domain-specific LSTMs still dominate in accuracy when task-specific data is ample and variability is high.
Scaling Law Limitation: Unlike NLP and vision foundation models, parameter count scaling does not guarantee improved adaptation in TSFMs for physiological time series. Architectural choices, patching strategies, in-context learning, and adaptation protocols matter greatly, consistent with recent findings questioning transferable gains from large TSFM pretraining on out-of-domain biomedical data [Karaouli2025].
Uncertainty Quantification: Calibration drift under fine-tuning signals the need for more robust probabilistic adaptation methods for clinical deployment, especially for hypoglycemic/hyperglycemic events.
Equity, Generalization, and the Future: Population heterogeneity in diabetes care emphasizes the need for sustained investment in benchmarks capturing subgroup variability and clinical risk, beyond aggregate error minimization.
Conclusion
GlucoFM-Bench provides the first standardized benchmark for blood glucose forecasting with TSFMs, systematically probing model generalization, adaptation, and clinical relevance across heterogeneous real-world populations. The results establish the viability of zero-/few-shot transfer in TSFMs, but reaffirm the competitiveness of lightweight, domain-specific supervised models in high-data settings. Persistent challenges in extreme glycemic ranges and transfer across phenotypes motivate further research in focused adaptation, robust calibration, and multivariate foundation modeling.
The benchmark’s open dataset and pipeline offer a reproducible testbed for methodological advances and facilitate equitable improvement of glucometric forecasting technology, directly supporting the next generation of adaptive, patient-centric diabetes management tools.

