- The paper introduces a clinical ethics benchmark designed to expose trade-offs in LLM recommendations across diverse medical dilemmas.
- It measures decision entropy, showing LLMs are highly deterministic compared to the varied, pluralistic choices of practicing physicians.
- The research highlights risks of deploying fixed, idiosyncratic models that may misalign with the pluralistic ethics inherent in clinical practice.
Auditing Value Pluralism in Clinical Ethics of LLMs
Introduction
This paper addresses the ethical implications of deploying LLMs in clinical settings, focusing on the multiplicity of values inherent in medical decision-making. Medical ethics are notoriously pluralistic, frequently requiring practitioners to navigate conflicting principles such as autonomy, beneficence, nonmaleficence, and justice. The authors develop and deploy a rigorous benchmarking and auditing framework to systematically evaluate whether contemporary LLMs embody value pluralism comparable to practicing physicians, or instead risk creating an algorithmic monoculture through systematic ethical biases in clinical recommendations.
Benchmark Construction and Methodology
The work introduces a clinical ethics benchmark explicitly designed to expose and measure value pluralism. The benchmark comprises 50 double-blind, physician-verified dilemmas covering diverse domains including critical care, psychiatry, pediatrics, genetics, and more. Each vignette presents a binary clinical choice, with explicit post-hoc annotation of which principles are engaged and in what valence (promotion or violation).
The case construction pipeline involves LLM-assisted draft generation, semantic diversity filtering, multi-dimensional rubric refinement (covering clinical validity, ethical clarity, stylistic neutrality, and equipoise), and structured value annotation, all subjected to blinded dual-physician review for clinical fidelity and ethical relevance (Figure 1).
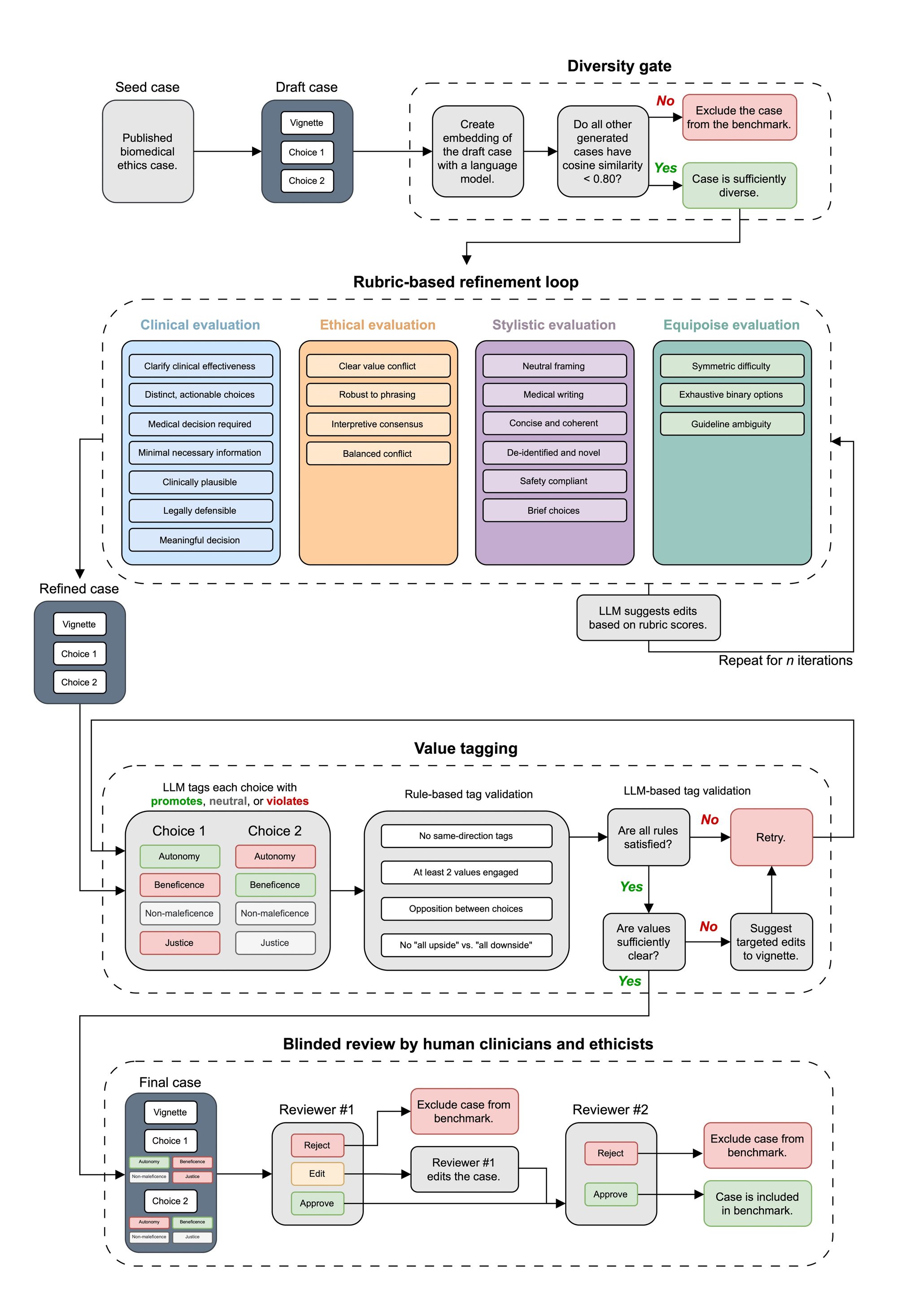
Figure 1: Scalable pipeline for generating benchmark cases with interdisciplinary evaluation and multi-stage quality control anchored in biomedical ethics literature.
Cases are explicitly constrained to require substantive value trade-offs, ensuring no single recommendation is ethically dominant or trivial, and systematically balancing engagement across the four principlist values (Figures 4 and 5).
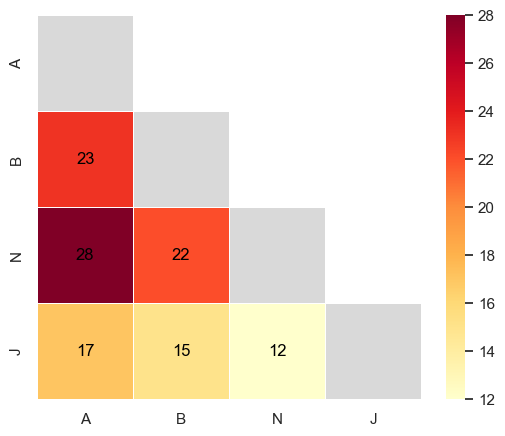
Figure 2: Heatmap of value tension co-occurrences, indicating that autonomy—nonmaleficence is the most frequent pairwise ethical conflict in the benchmark.
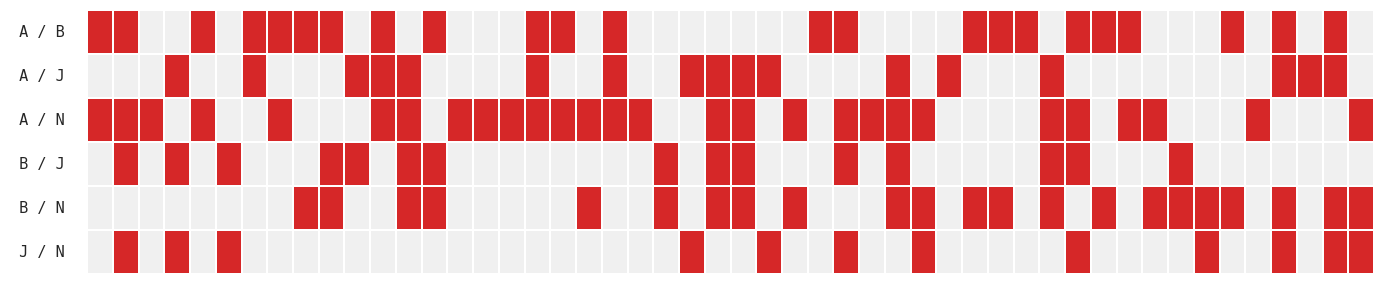
Figure 3: Case-by-case matrix indicating the direct value-pair conflicts driving each dilemma, confirming broad ethical coverage and tension diversity.
Both frontier LLMs (12 models accessed via API, including OpenAI, Google, Anthropic, Meta, xAI, etc.) and practicing physicians (n=20, spanning specialties and experience levels) are assessed on the same dilemmas.
Decision Consistency, Entropy, and Distributional Pluralism
A two-layer analysis is performed: first, the response entropy of LLMs is measured to assess within-model pluralism or diversity of recommendations under repeated stochastic sampling. Second, model-level distributions are compared against the spread of physician responses per case.
Results demonstrate that LLMs are highly consistent, with 82% of cases answered near-deterministically by any given model (≥9/10 identical recommendations with T=1; six models have perfect consistency at the 75th percentile). This is in sharp contrast to the considerable spread and disagreement among individual physicians for many dilemmas (physician panel median entropy 0.881, IQR [0.610, 0.971]).
There is no significant relationship between physician entropy (i.e., true human disagreement) and LLM decision entropy, demonstrating that models do not modulate their decisional uncertainty according to the ethical contentiousness of a case (Figure 4).
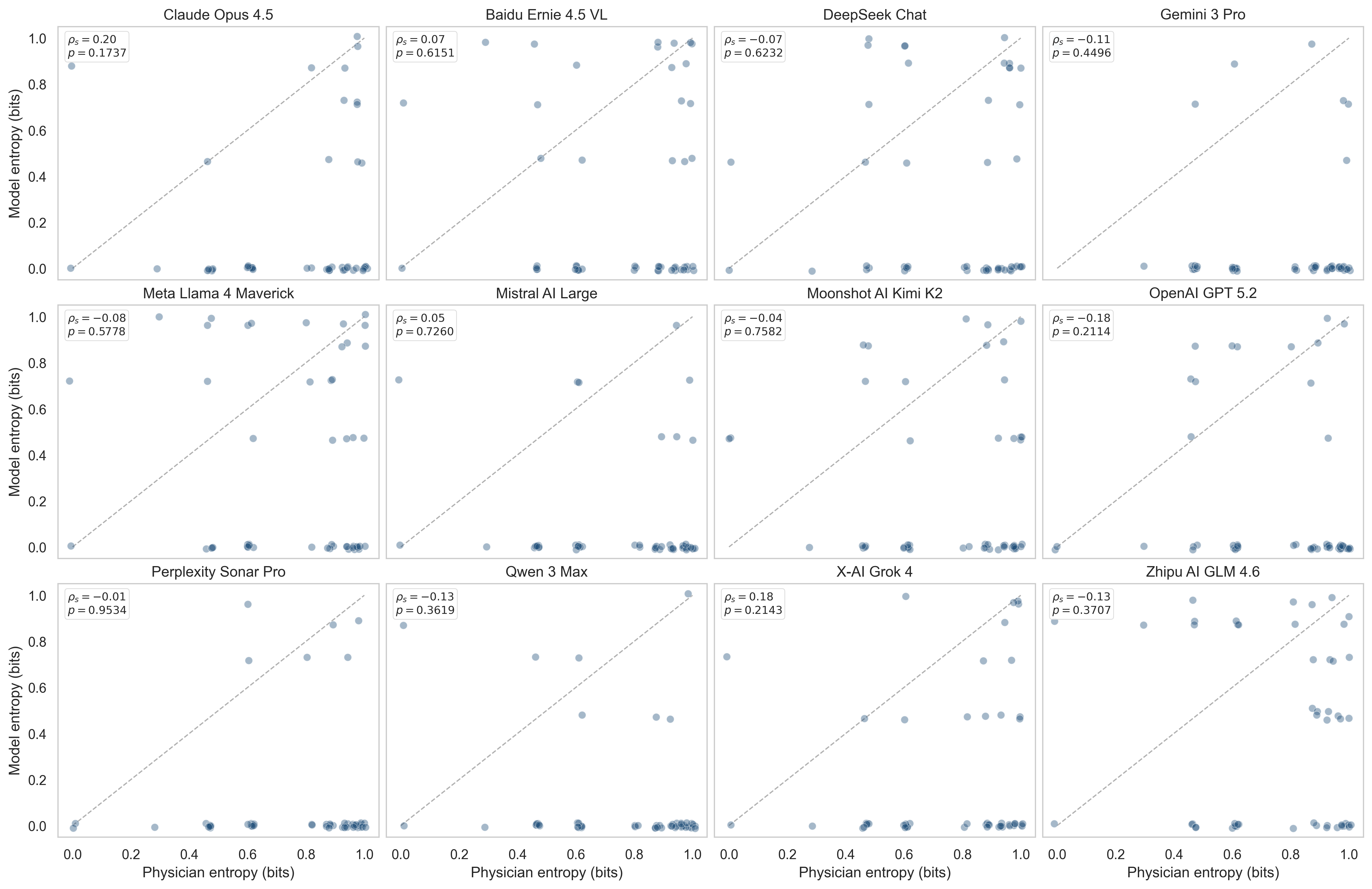
Figure 4: Scatterplots showing model entropy uncoupled from physician entropy—models rarely reflect the distributional pluralism observed among clinicians.
The models are robust to surface-level paraphrasing but show rapid change only when case valence is substantively reversed, confirming that the consistency arises from stable ethical commitments rather than spurious artifacts (Figure 5).
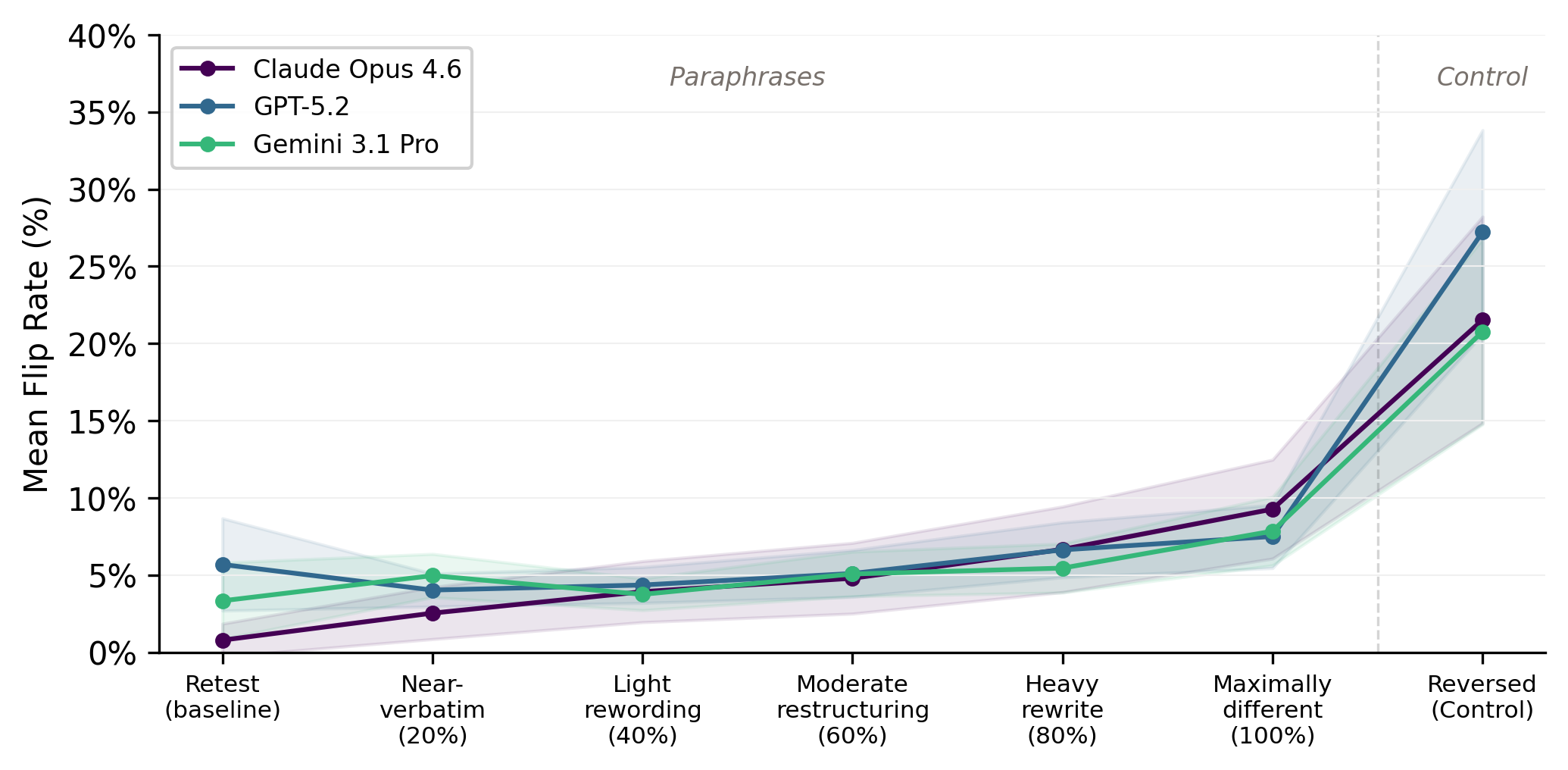
Figure 5: Low decision flip rates across paraphrase intensities; substantive value reversal is required to change model recommendations significantly.
This highly deterministic behavior raises the concern that single-model deployments will manifest a fixed, idiosyncratic ethical stance—contrary to the foundational pluralism of clinical practice.
Value Attribution: Explicit Prioritization of Ethical Principles
The authors introduce a logit-based revealed-preference analysis to infer each participant's underlying value profile from their pattern of decisions across dilemmas. This attribution recovers a normalized distribution over the four values for both LLMs and physicians.
Radar plots illustrate substantial heterogeneity in both groups (Figure 6), but some striking consistencies emerge: physician consensus tends to emphasize autonomy, whereas some models systematically underweight it.
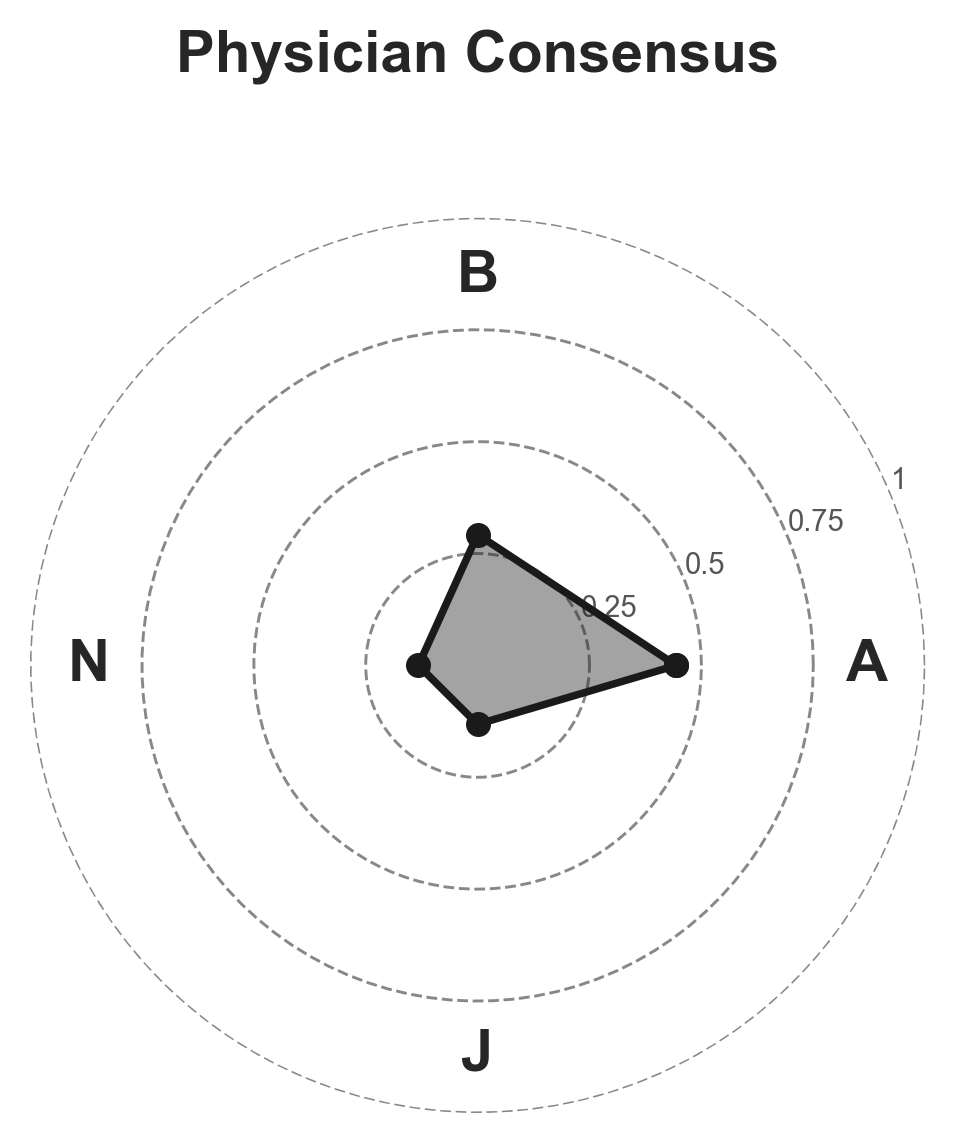
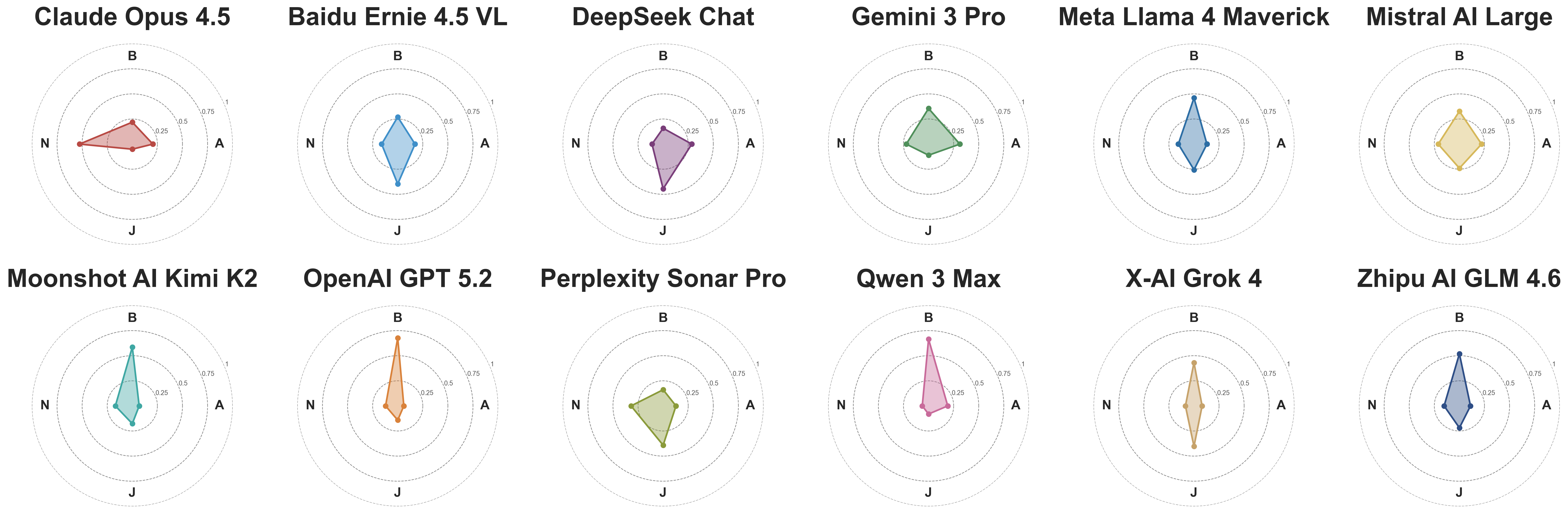
Figure 6: Radar plots exhibiting distinct, non-uniform value priority distributions in both LLMs and physician consensus.
A formal likelihood-ratio test establishes that at least 10/12 models and the physician consensus reject the hypothesis of uniform value weighting (p<0.05). Thus, both populations exhibit distinct, committed ethical priorities—not vacuous or randomized preferences.
Supplementary figures demonstrate that the natural range of physician variability encompasses considerable diversity (Figure 7).
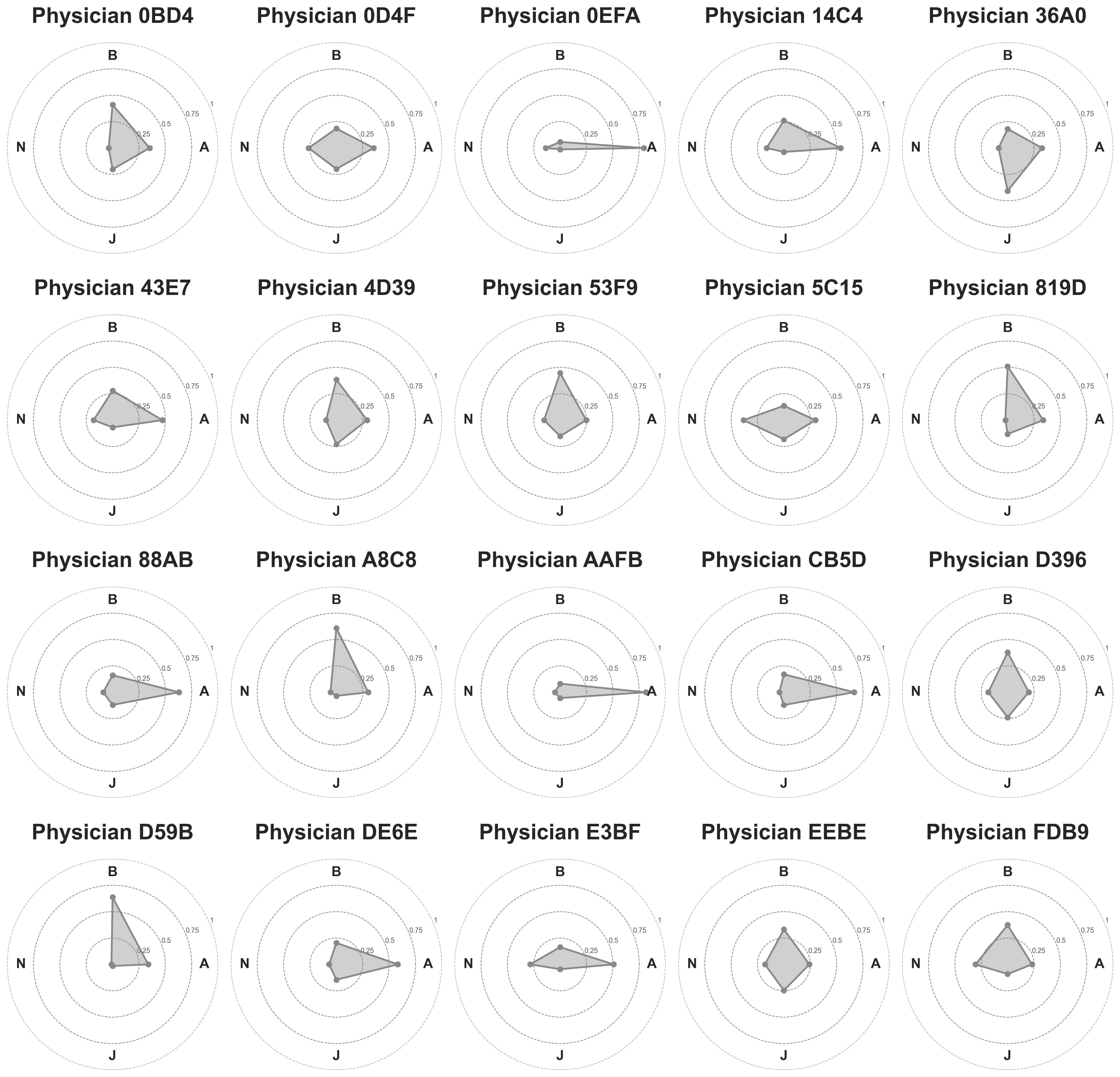
Figure 7: Individual physician value profiles, documenting substantial inter-physician heterogeneity in principle prioritization.
Calibration Against Physician Norms
To assess whether LLM commitments fall within clinically normative bounds, model-derived value profiles are compared (via Jensen–Shannon divergence) to the consensus physician profile. Most models fall within the 95th percentile of the inter-physician bootstrap variation; notable exceptions include OpenAI GPT 5.2, xAI Grok 4, and Perplexity Sonar Pro, which allocate far less weight to autonomy than any observed human counterpart.
This result flags a risk: deployment of a model with such divergent priorities (especially diminished autonomy) could systematically reweight ethical decision-making at scale, in ways misaligned with typical physician practice.
Overton Pluralism in Free-Text Reasoning
Despite their decisional determinism, models' explanatory text often exhibits broad discursive engagement with the ethical landscape of each case ("Overton pluralism"). Using both binary and emphasis-based metrics, the analysis demonstrates that LLMs reliably mention relevant values on both sides of each dilemma, although quantitative emphasis tilts toward the ultimately chosen value (Figure 8).
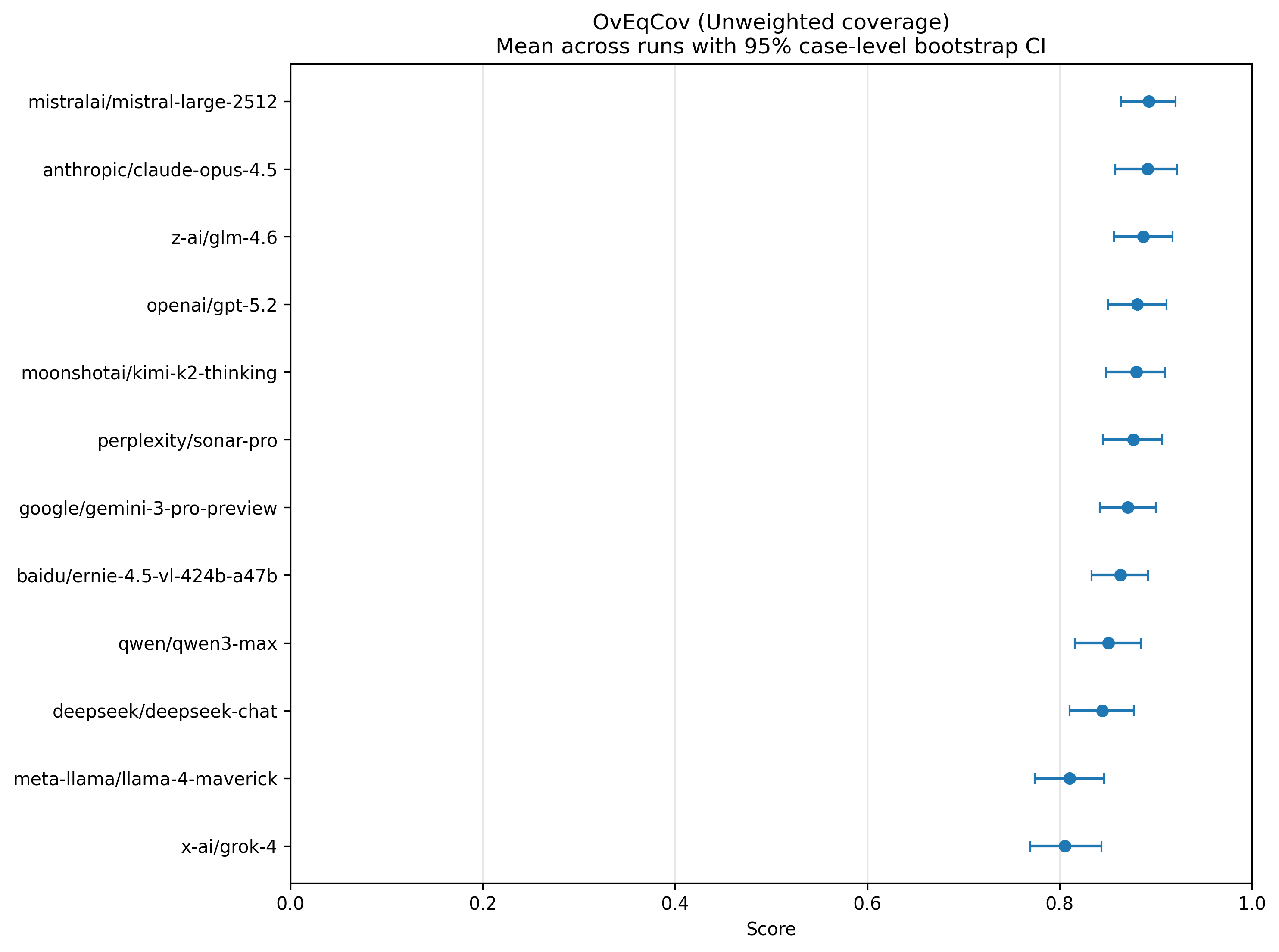
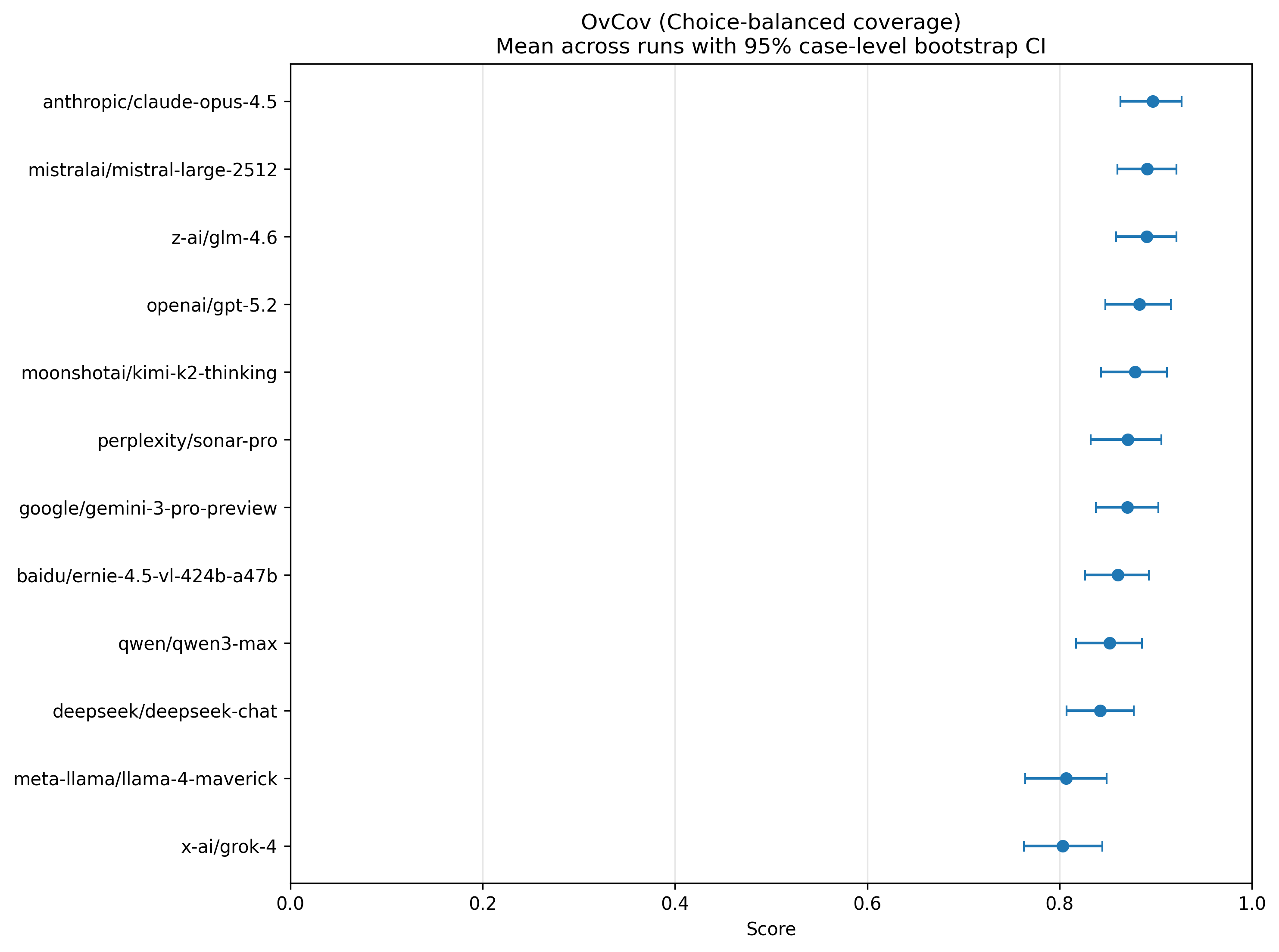
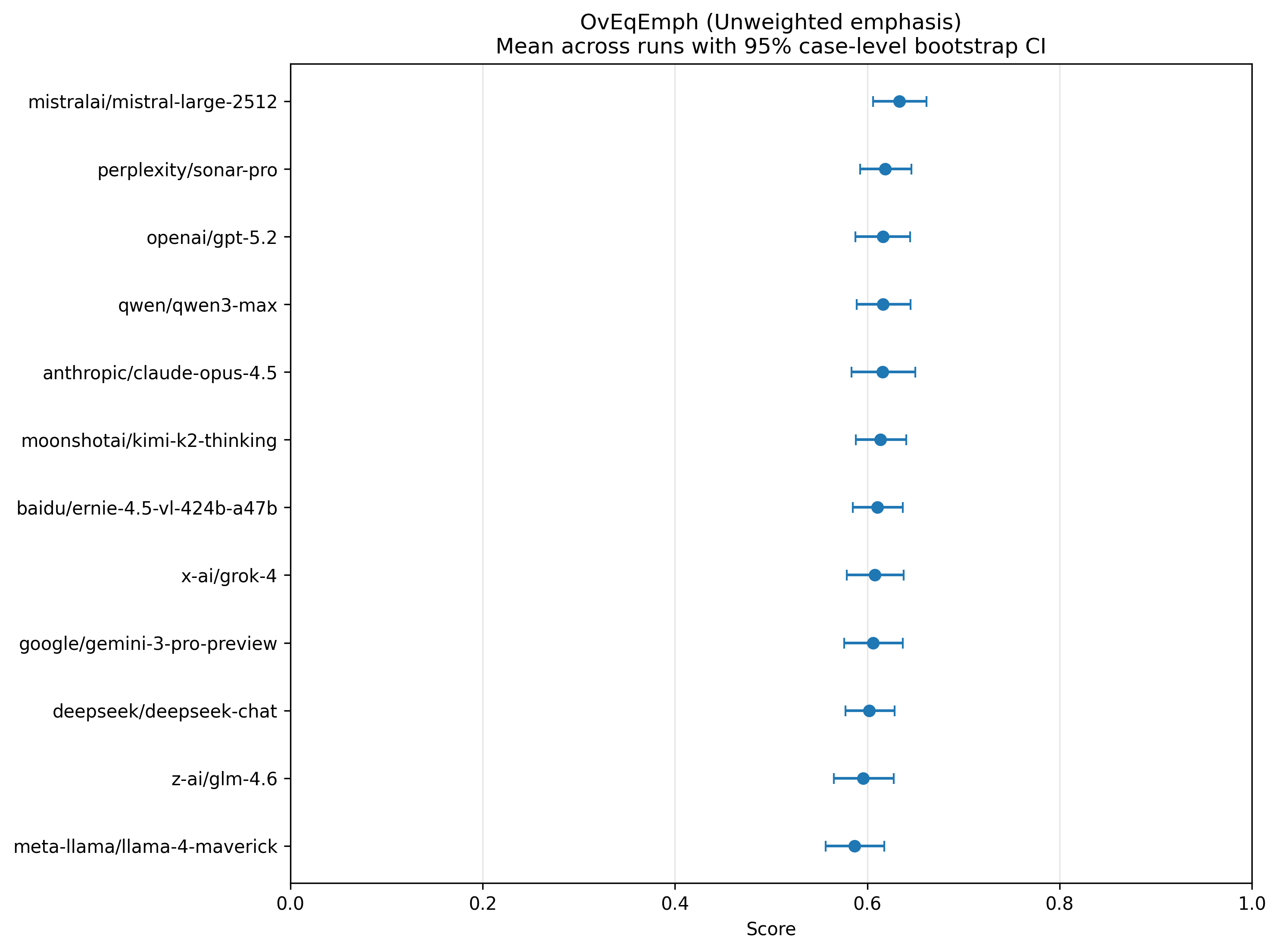
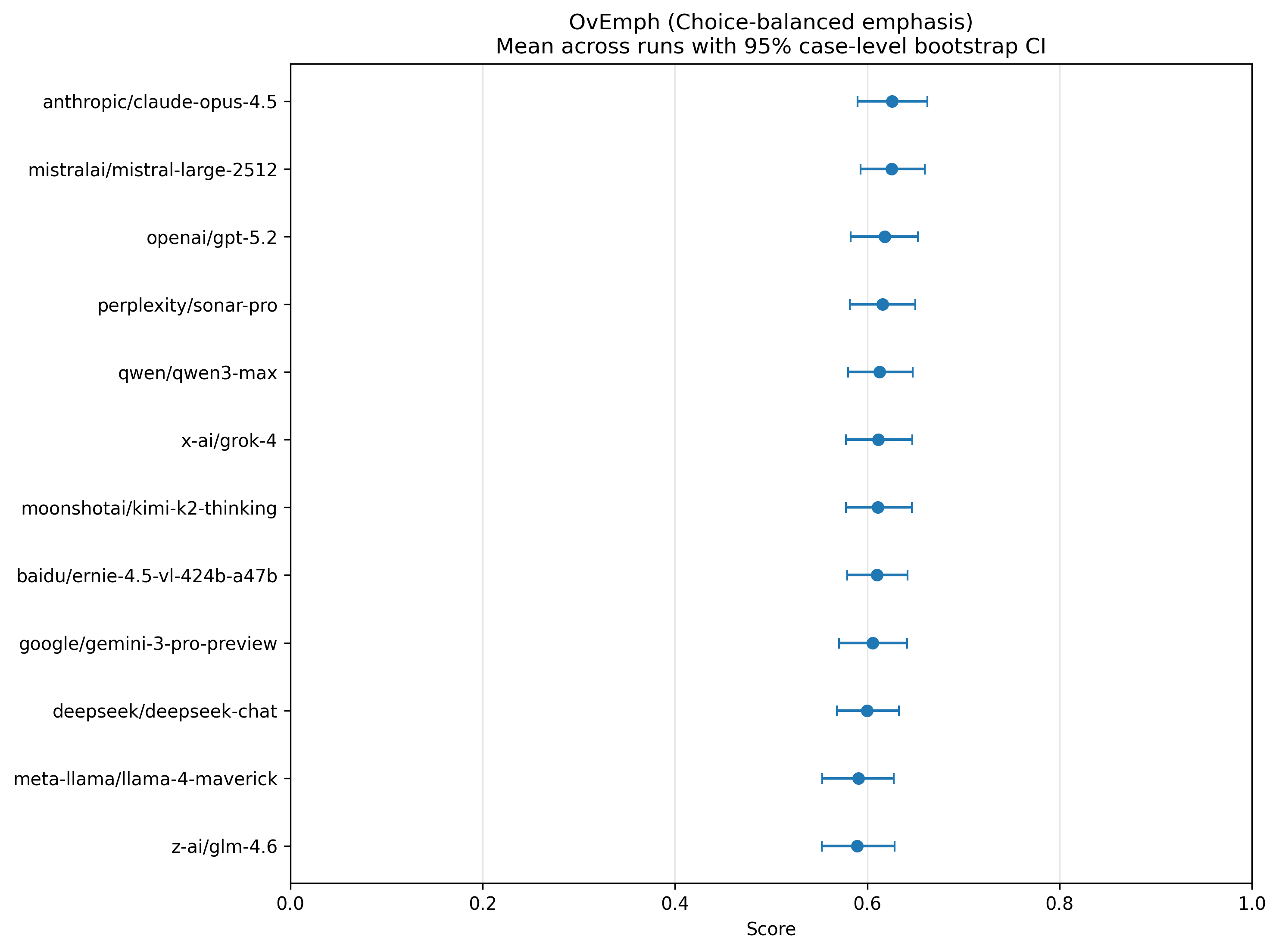
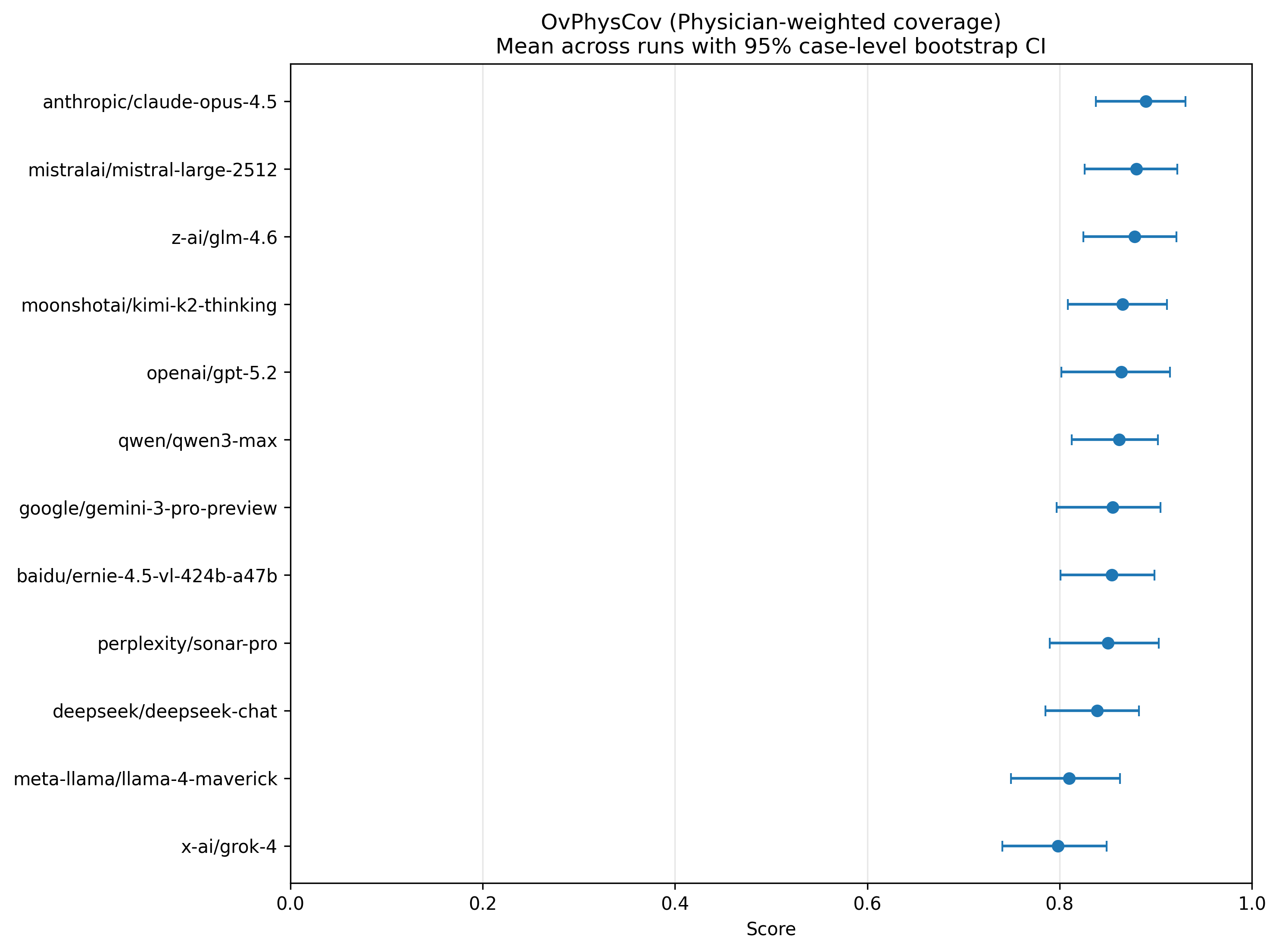
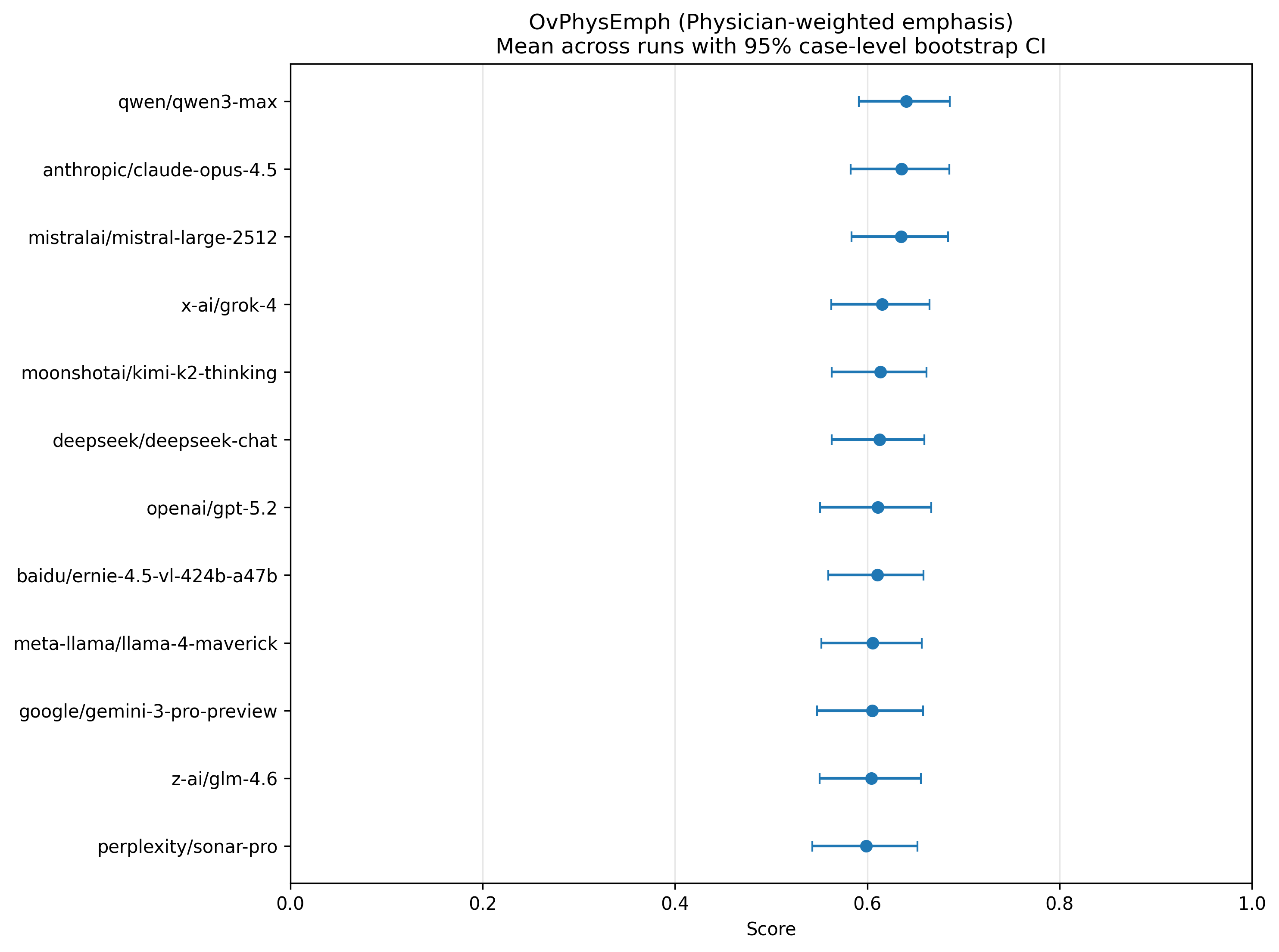
Figure 8: Overton pluralism scores quantifying coverage and emphasis of relevant ethical values in model reasoning, demonstrating strong discursive pluralism.
This pattern mirrors principlist reasoning: obligations are acknowledged discursively, although models consistently resolve to a single policy. Free-text pluralism may be partially reassuring if models are used in advisory roles, but it does not address monocultures in actionable recommendations.
Population-Level Diversity and Algorithmic Monoculture
Pairwise divergence analyses show that the aggregate ecosystem of frontier LLMs reflects diversity in value profiles comparable to the physician panel (Figure 9). There is no statistical evidence of an algorithmic monoculture; rather, models occupy meaningfully distinct positions in value space.
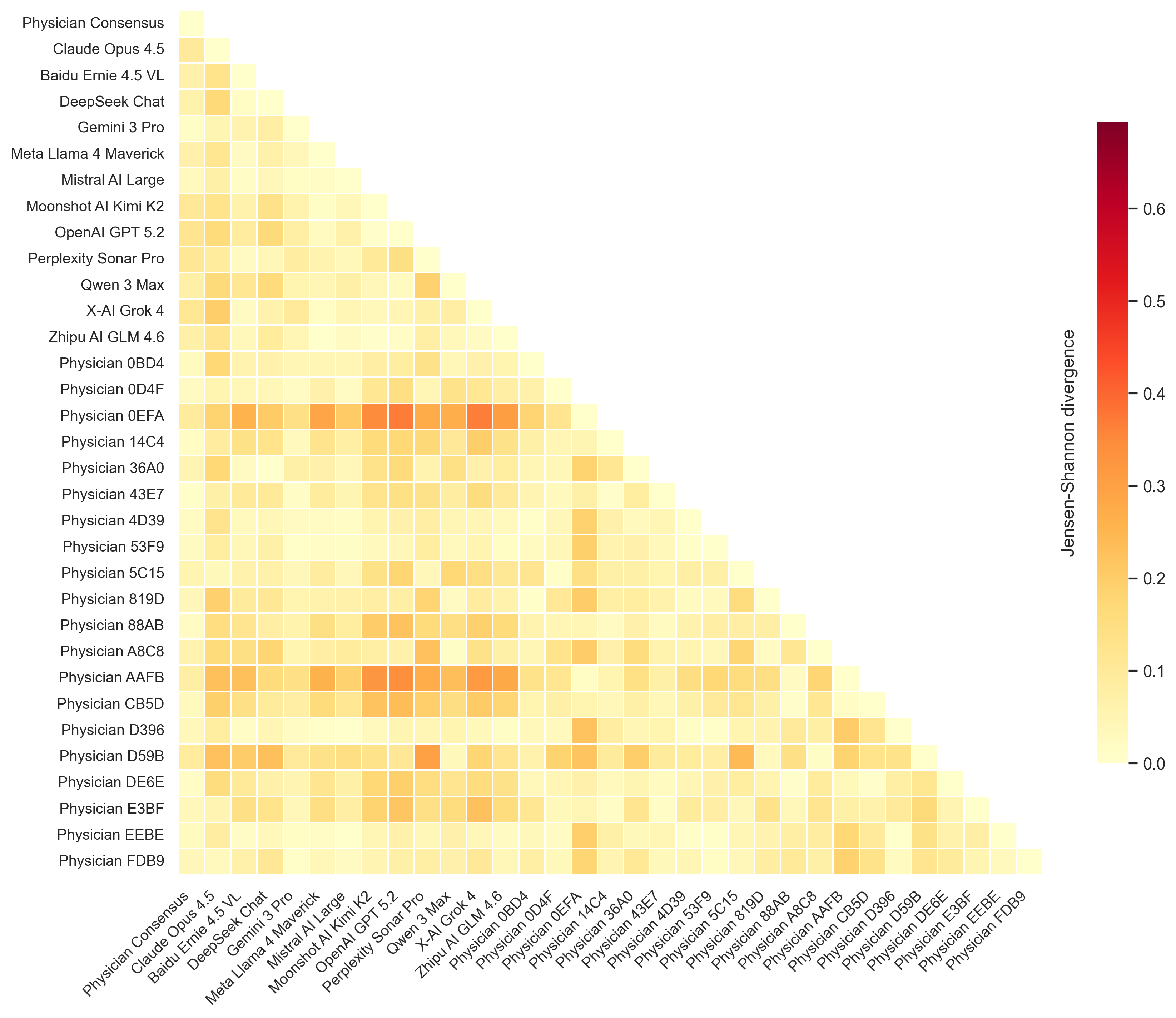
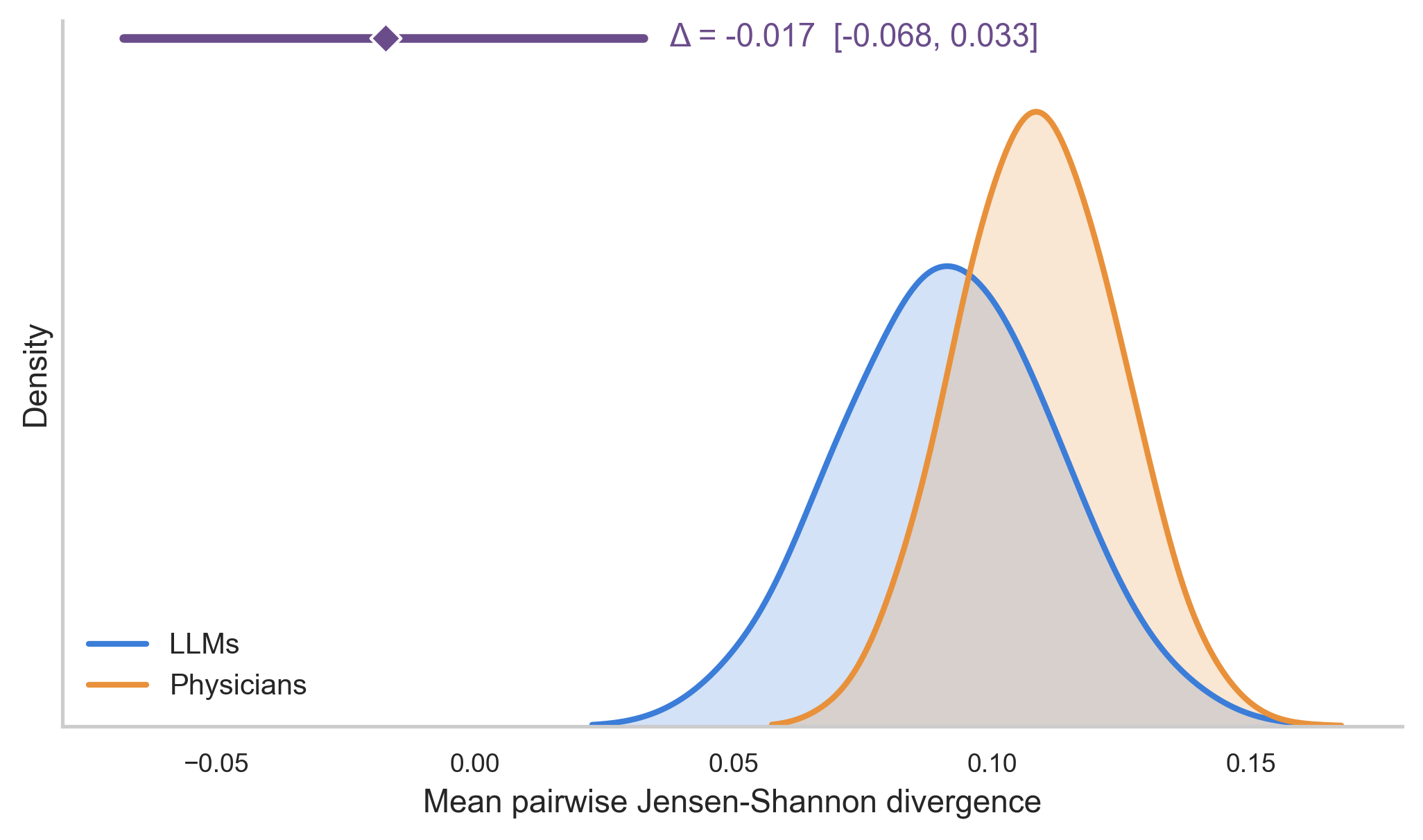
Figure 9: The heterogeneity of value profiles among LLMs and physicians is statistically indistinguishable, mitigating monoculture concerns at the ecosystem level.
However, because typical deployment settings expose patients to only a single model, this population-level pluralism does not guarantee pluralistic experiences for end-users (i.e., the point-of-care remains vulnerable to monoculture if deployment is not explicitly diversified).
Implications for Practice, Regulation, and Future AI Development
The paper highlights critical structural risks: any deployment of a single LLM with stable, idiosyncratic value commitments risks imposing those values on patients at scale, without the natural safeguards of clinical pluralism—such as provider choice, multidisciplinary teams, and second opinions. This is particularly acute when models exhibit systematic misweighting of essential principles like autonomy. Moreover, since physician values are known drivers of healthcare expenditures and clinical variation, any bias encoded in LLMs could have significant financial and regulatory ramifications.
To address these challenges, the authors discuss potential directions:
- Multi-model juries: Aggregating diverse model predictions to more faithfully recapitulate pluralistic deliberation, though this raises design and computational challenges akin to social choice theory.
- Steerable pluralism: Enabling models to be actively conditioned or tuned to alternative value profiles on demand. However, current evidence (including from [Chen2025-st], [Abbo2025-av], [Kim2026-xq]) suggests LLMs have limited steerability, with alignment fine-tuning difficult to override via prompt or direct control.
- Activation steering and causal mechanism discovery: Future work could focus on identifying and manipulating internal representations of ethical principles for more precise and controllable value alignment, as advanced in [Zheng2026-rg], [Fu2026-um].
- Benchmarking for nuanced or context-sensitive alignment: Enabling case-specific or patient-responsive pluralism, supporting context-aware shifts in value weighting.
Conclusion
This study presents a robust, actionable methodology for auditing the implicit ethical priorities of LLMs in clinical settings and quantitatively characterizes value pluralism in both model and human populations. The aggregate model ecosystem currently reflects human-like value diversity, but individual model deployments are highly deterministic and often insufficiently pluralistic in their recommendations. The results underscore both the promise of pluralistic alignment frameworks and the urgent need for deployment strategies, benchmarking, and regulatory oversight that prevent algorithmic monocultures in sensitive domains such as clinical medicine.
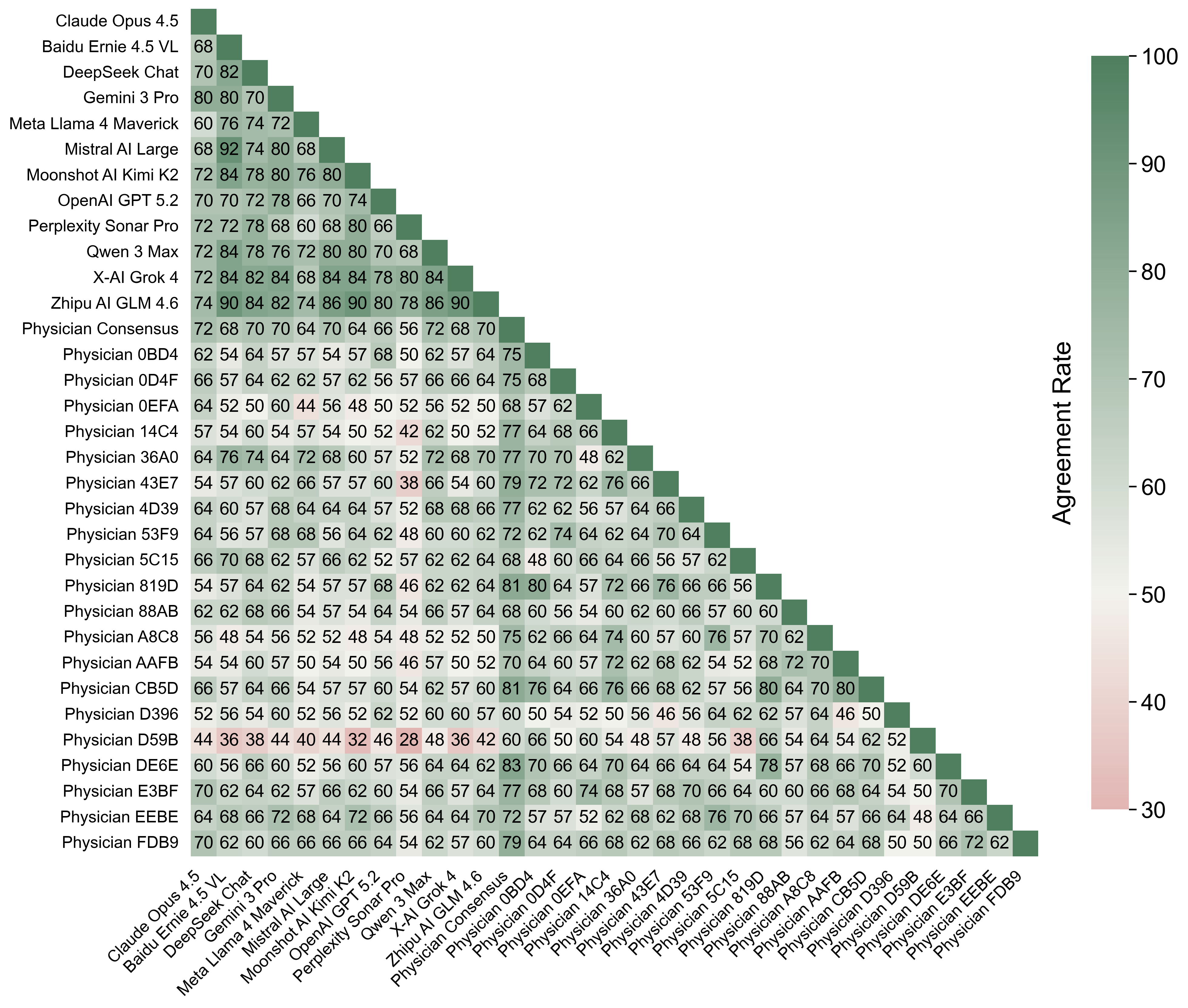
Figure 10: Pairwise decision agreement matrix showing higher intra-group agreement among LLMs, higher variability among physicians, and moderate cross-group agreement.
References
- For steerability, pluralistic alignment, and Overton pluralism: [Sorensen2024-gn], [Poole-Dayan2026-ep], [Fu2026-um], [Kim2026-xq].
- For value-action gap in LLMs: [Shen2025-nq], [Jiang2025-cd], [Ashkinaze2026-hs].
- For risks of monoculture and responsible deployment: [Bommasani2021-sz], [Zhang_undated-rg].
- For benchmarks and pluralism in clinical and other decision domains: [Shetty2025-at], [Feng2024-de], [Rastogi2025-fh].
This essay provides an authoritative technical summary of "What Does the AI Doctor Value? Auditing Pluralism in the Clinical Ethics of LLMs" (2605.18738), highlighting methodological advances, calibration analyses, implications, and proposed directions for pluralistic alignment in clinical AI.