- The paper introduces a novel unsupervised segmentation method that integrates diffusion models with radiomic distillation to enhance lung pathology discrimination.
- It employs HU-preserving DDPM training, contrastive InfoNCE loss, and multi-timestep feature aggregation to capture density and texture details in CT images.
- Experimental results demonstrate improved generative and segmentation metrics, including lower FID, higher SSIM, and superior Dice scores across lung tissues.
DiffSegLung: Diffusion Radiomic Distillation for Unsupervised Lung Pathology Segmentation
Introduction and Motivation
DiffSegLung addresses the unsupervised segmentation of lung pathologies in CT, targeting emphysema, fibrosis, consolidation, and cavitary lesions—challenging due to the lack of robust annotated datasets and intrinsic class imbalance. Existing approaches either utilize diffusion-based models without leveraging the Hounsfield Unit (HU) distribution vital for tissue discrimination or depend on handcrafted radiomic features without the representational capacity of deep generative networks. DiffSegLung introduces Diffusion Radiomic Distillation, integrating handcrafted radiomic descriptors as a physics-grounded teacher via a contrastive objective to regularize the bottleneck representations of a 3D diffusion U-Net, effectively transferring pathology-discriminative structure in a fully annotation-free setting.
Methodology: Diffusion Radiomic Distillation
The pipeline comprises HU-preserving DDPM training and unsupervised inference. During training, each patch's handcrafted radiomic features (GLCM, LBP, Gabor, first-order HU statistics) are projected into an embedding space and serve as the teacher. The bottleneck of the DDPM, projected via a student head, is regularized using an InfoNCE contrastive loss, aligning student and teacher embeddings for patches with high physical similarity, ensuring learned representations reflect density and texture distributions essential for pathology separation.
At inference, the teacher head is discarded. The frozen DDPM encoder outputs bottleneck embeddings at multiple reverse timesteps, which are aggregated and clustered via a Gaussian Mixture Model. Cluster means are mapped to pathology labels using HU thresholds, reflecting clinical decision rules. Sobel-Diffusion Fusion is introduced for boundary refinement, combining gradient-based edge detection with cluster boundaries and HU compatibility checks for robust contour delineation.
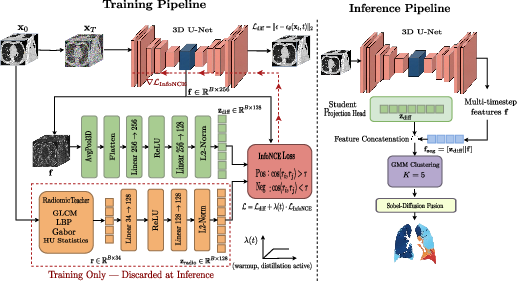
Figure 1: Training: ϵθ is trained on HU-preserved patches via L; radiomic descriptors align student embeddings by InfoNCE and are discarded during inference. Multi-timestep features are clustered and refined for segmentation.
Experimental Results
Generation Quality
DiffSegLung achieves superior performance across all generative metrics. The FID (Fréchet Inception Distance) improves from 31.7 (LungDDPM+) to 18.4. Similarly, SSIM and PSNR scores reach 0.891 and 31.8, outperforming previous methods including MedVAE, which suffers from excessive HU information loss. These results validate that radiomic distillation not only enhances discriminative capacity but also benefits generative fidelity by imposing physical structure on the latent space.
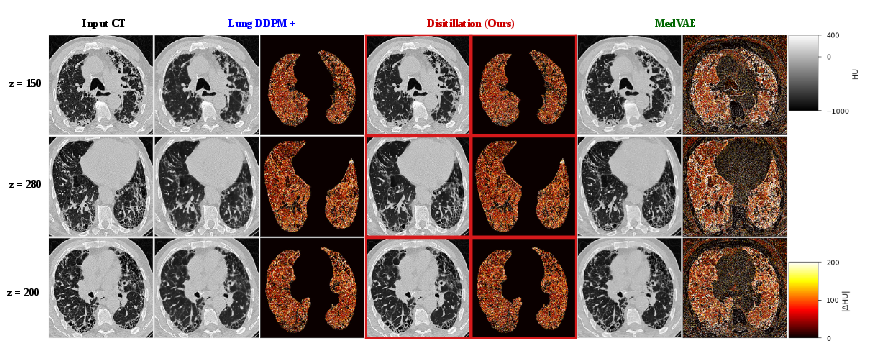
Figure 2: Qualitative generation comparison (random axial slices). DiffSegLung preserves HU density ranges and parenchymal texture more faithfully compared to LungDDPM+ and MedVAE.
Segmentation evaluation on 190 expert-annotated axial slices from four CT cohorts demonstrates strong mean Dice scores over all pathology classes. The Dice coefficient for healthy tissue, GGO, fibrosis, and emphysema reaches 89.3, 84.1, 86.4, and 76.2 respectively, with the best mean DSC and lowest HD95 error across unsupervised baselines.
The emphysema segmentation remains most challenging due to significant HU overlap with healthy parenchyma. The radiomic distillation framework, incorporating four highly discriminative descriptor families, yields robust class separation for fibrosis and consolidation but limited gains in regions of HU ambiguity, suggesting future extensions with more sophisticated texture descriptors and HU-aware clustering.
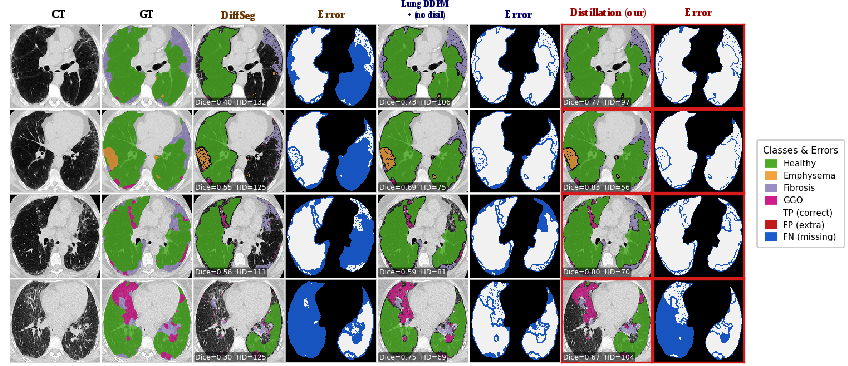
Figure 3: Qualitative segmentation comparison on representative axial slices. DiffSegLung delivers sharper and more physiologically accurate boundaries than previous unsupervised approaches.
Ablation studies reveal that HU-preserving training is the most impactful component (+3.5 DSC), underscoring the necessity of retaining physical density information. Distillation alone (without warmup) causes bottleneck collapse, but the warmup schedule recovers and exceeds the HU-only baseline. Multi-timestep aggregation and Sobel-Diffusion Fusion further enhance boundary localization, while fast ODE-solver sampling maintains accuracy with significant speedups in inference.
Practical and Theoretical Implications
DiffSegLung's teacher-student radiomic distillation introduces a paradigm for unsupervised segmentation, leveraging domain-specific handcrafted descriptors as powerful contrastive signals without any annotations. The integration of HU-preserving DDPM training bridges classical radiomics and modern diffusion generative modeling. Practically, this enables scalable, annotation-free segmentation across heterogeneous CT datasets, applicable to clinical and research workflows where labeling is infeasible.
Theoretically, the framework shifts unsupervised medical image analysis toward physically-informed representation learning. By enforcing radiomic structure in latent spaces, DiffSegLung demonstrates pathology separation emerges without explicit supervision. The workflow's reliance on domain knowledge for cluster assignment (HU thresholds) but not for training paves the way for further advances in combining physics-driven and data-driven unsupervised learning.
Future developments may target improved class separation for pathologies with overlapping HU distributions using higher-order texture descriptors or learned clustering algorithms. Extensions to broader modalities and pathology types could generalize the distillation scheme across medical imaging domains.
Conclusion
DiffSegLung presents a robust annotation-free segmentation method that outperforms prior baselines in both generation fidelity and segmentation accuracy by leveraging radiomic distillation with HU-preserving diffusion models. The radiomic teacher-student scheme integrates handcrafted physics-aware descriptors as a contrastive signal, shaping DDPM bottleneck representations for unsupervised pathology separation. Its practical efficacy and theoretical innovation mark a substantial advancement in physically-grounded unsupervised segmentation pipelines for medical imaging (2605.11758).