- The paper introduces GlottisNet, a real-time, scale-robust network that efficiently segments the glottis during nasal transnasal intubation.
- It innovates with a Lightweight Scale Robust Module (LightSRM) and adaptive label assignment to enhance both segmentation precision and computational efficiency.
- Experimental results show superior performance with mDice scores from 77.6% to 92.9%, >170 FPS on GPU, and robust detection of small glottal features.
Real-time Scale-Robust Glottis Segmentation for Nasal Transnasal Intubation
Introduction and Motivation
Nasotracheal intubation (NTI) is essential for airway establishment, particularly in cases of restricted oral access or specialized surgical scenarios. Machine-assisted NTI, leveraging vision-based robotic navigation, aims to standardize outcomes and minimize risks such as hypoxemia and airway trauma. However, real-time visual detection of glottal structures faces significant challenges: complex anatomical backgrounds, variable illumination, and especially drastic scale variations as the glottis transitions from small, peripheral to near full-field targets.
Existing SOTA visual detectors—both lightweight single-stage and high-precision two-stage frameworks—struggle with either segmentation accuracy or computational efficiency, making them suboptimal for portable clinical devices. The need is for a framework that is scale-robust, accurate, and deployable for real-time NTI guidance.
Methodology and Architectural Innovations
The proposed GlottisNet achieves balance between segmentation precision, scale robustness, and computational efficiency by introducing the Lightweight Scale Robust Module (LightSRM) as a central architectural unit.
GlottisNet's backbone and neck both utilize identical LightSRM modules, promoting consistent modular design and facilitating efficient feature extraction and fusion across all layers. The neck leverages a PAN-inspired bidirectional feature fusion mechanism, enhancing spatial and semantic integration between top-down and bottom-up pathways.
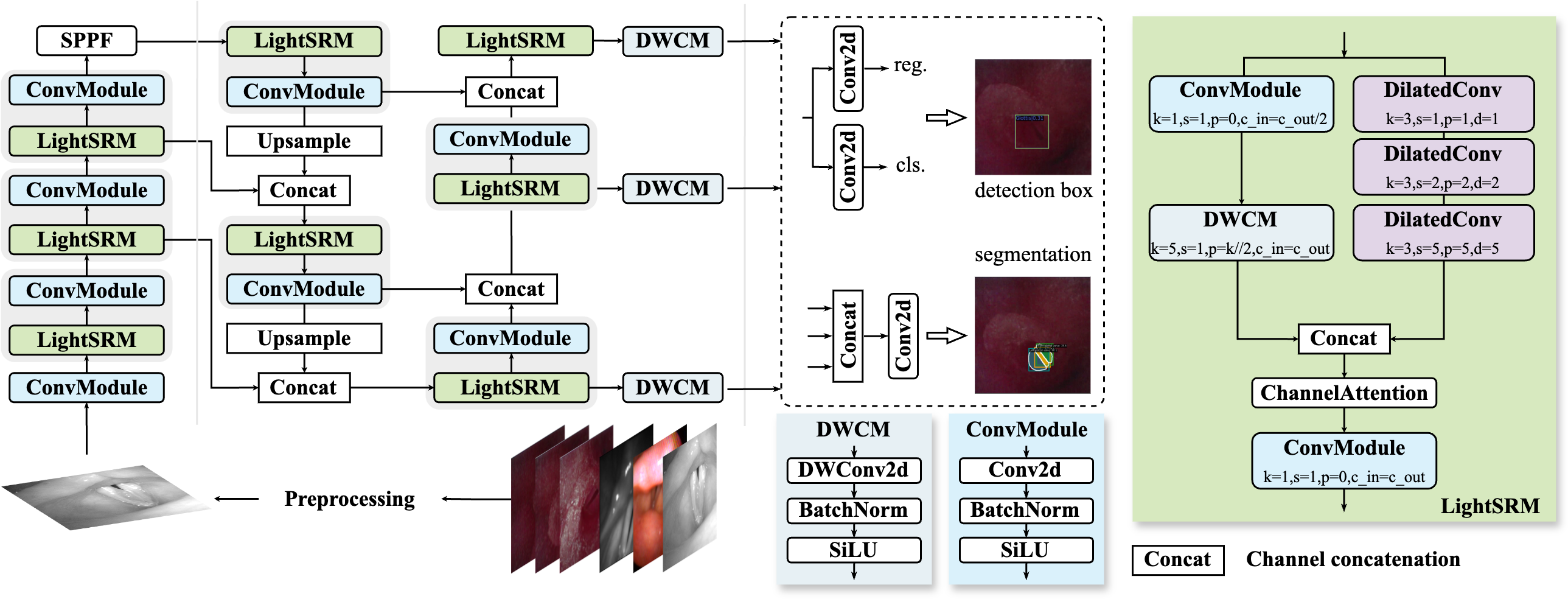
Figure 1: The architectural overview of GlottisNet, showing integration of ConvModule, LightSRM, DWCM, and auxiliary components for efficient feature processing and fusion.
LightSRM Design
LightSRM comprises a dual pathway: a main path with cascaded dilated convolutions (optimal rates [1,2,5]) for large receptive fields, and a shortcut path with 5×5 depthwise separable convolution for computational savings. Outputs are concatenated and processed via channel attention to enhance inter-channel dependencies, followed by 1×1 convolution for channel adjustment.
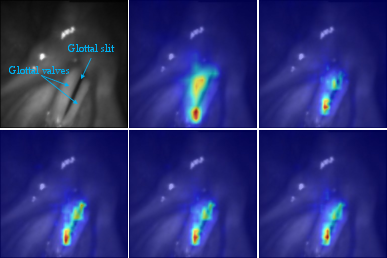
Figure 2: Grad-CAM activations through the LightSRM block, demonstrating evolving glottic feature focus and improved gap localization within complex backgrounds.
Scale Robust Feature Pyramid Network (SRFPN)
SRFPN augments FPN with bottom-up aggregation, fusing high-level semantic and low-level spatial features using LightSRM blocks. Depthwise separable convolutions ensure consistent channel representation while maintaining efficiency.
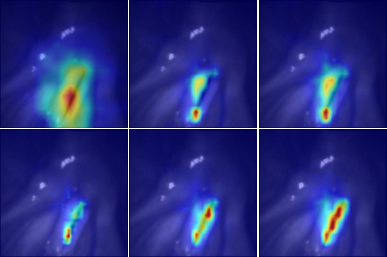
Figure 3: Grad-CAM heatmaps through GlottisNet’s hierarchical pathways, capturing progressive spatial refinement toward the glottal aperture.
Adaptive Label Assignment
A novel cost matrix governs dynamic positive-negative sample selection during training—comprising weighted IoU, classification, and center priority costs (λ1=3,λ2=1,λ3=3)—minimizing intra-class variance and improving robustness. The Euclidean-based center priority cost is rotation-invariant, crucial for NTI's non-deterministic glottis orientation.
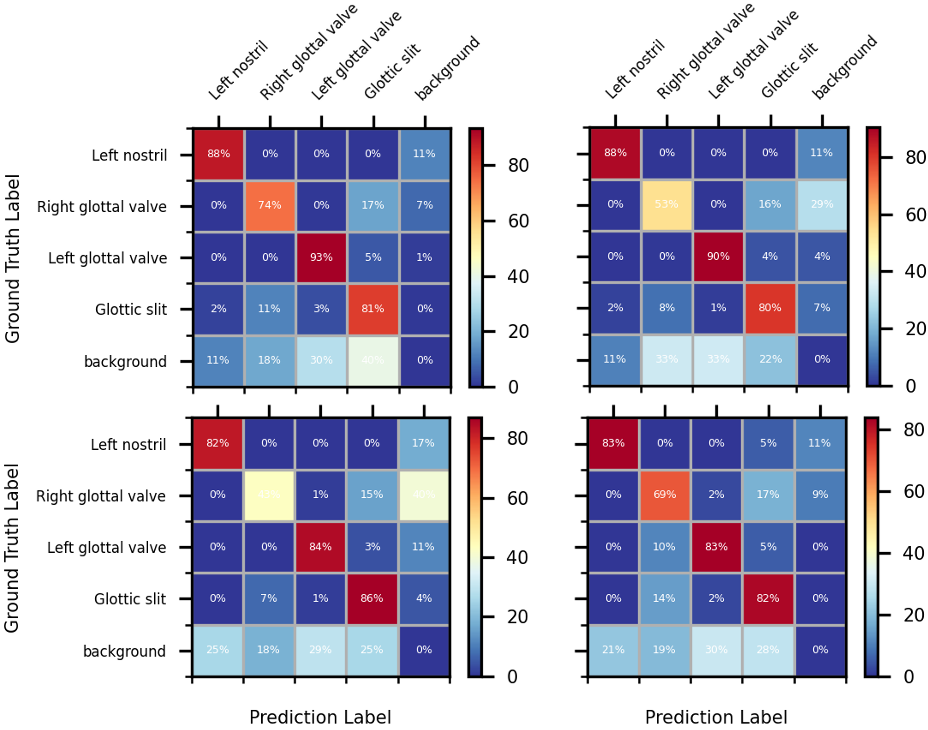
Figure 4: Confusion matrices for cost matrix ablations, showing strong intra-class discrimination with the [3,1,3] configuration, especially for hard samples.
Experimental Validation
Hardware and Datasets
GlottisNet was validated on a nasotracheal intubation robotic platform (Figure 5), utilizing PID (phantom), BAGLS (multi-device, multi-clinician), and clinical datasets (real-world endoscopic NTI).
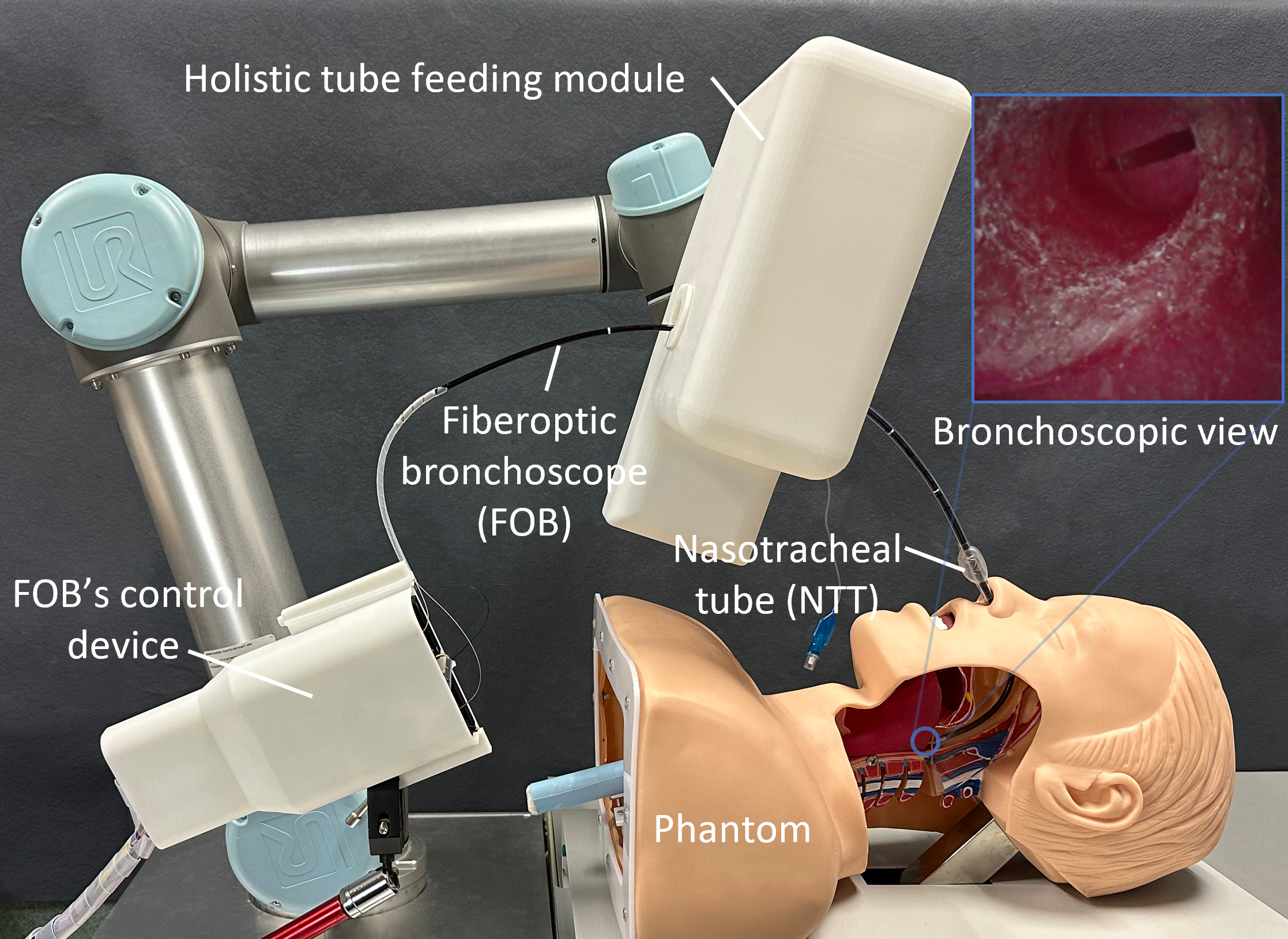
Figure 5: Robotic NTI system—robotic arm manipulates the FOB, guided by GlottisNet detection outputs.
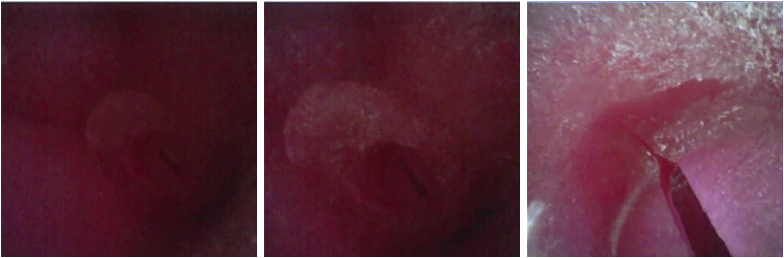
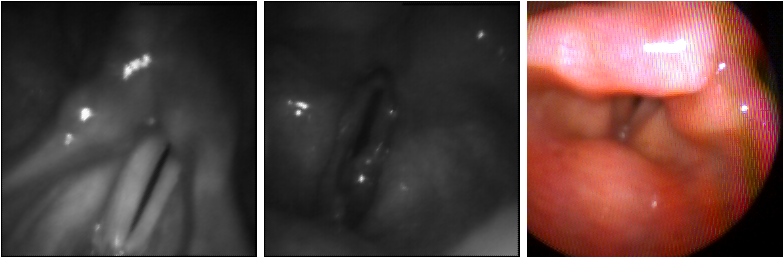
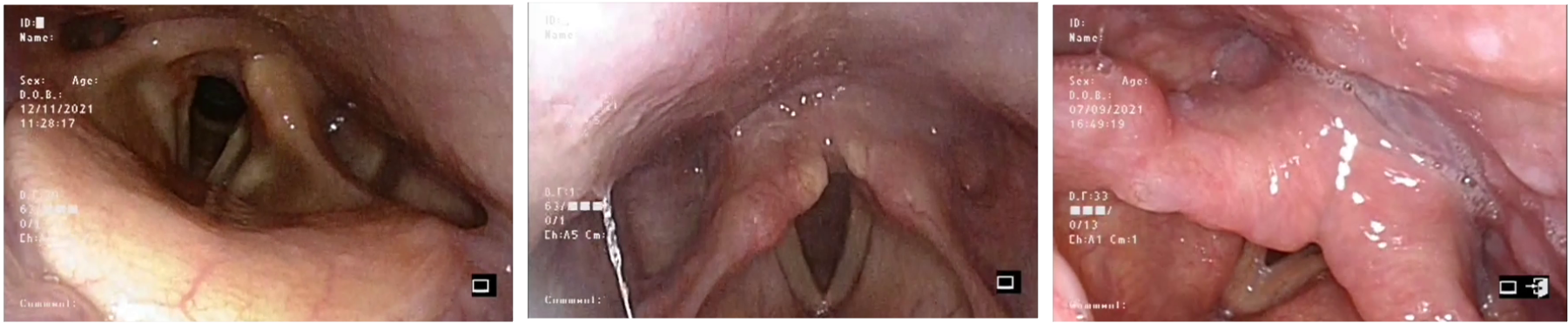
Figure 6: Representative samples highlighting the challenge of scale, illumination, and anatomical complexity in glottis segmentation.
Ablation Studies
Comprehensive experiments dissected the impact of LightSRM components, cost matrix weights, dilation rates, and positive sample count. LightSRM integration delivered more than 1.1-fold improvements in AP50 and mDice; channel attention was critical for maintaining discriminative feature propagation. Optimal dilation rates ([1,2,5]) maximized receptive field without computational redundancy.
Reducing positive sample TopK from 13 to 3 improved performance (mAP=↑57.2%; mDice=↑91.7%), demonstrating that high-quality discriminative samples are more beneficial than quantity.
Numerical Results and Comparative Analysis
GlottisNet achieved maximal performance across all datasets:
- Segmentation mDice: 92.9% (PID), 89.6% (BAGLS), 77.6% (Clinical)
- Model size: 19 MB
- Inference speed: >170 FPS (RTX 3090; 44.4 FPS on CPU)
- Small-object accuracy: PID APS=22.2% vs RTMDet-s 12.2%
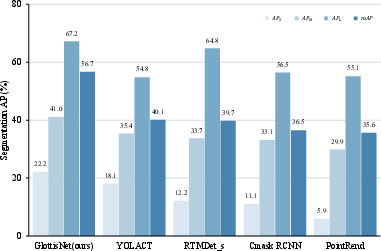
Figure 7: GlottisNet outperforms SOTA methods for small-object detection (5×50), validating LightSRM’s scale robustness.
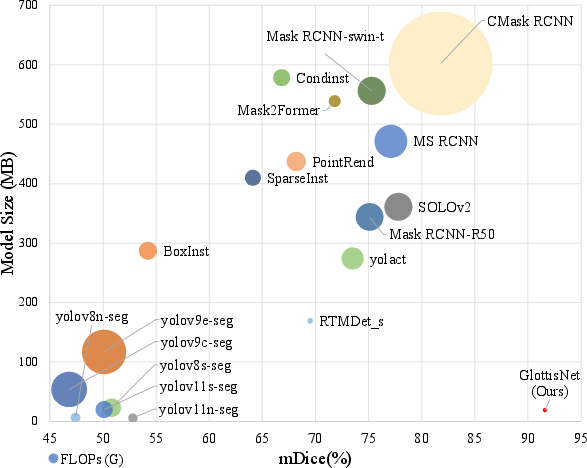
Figure 8: Pareto comparison of model accuracy (mDice), computational cost (FLOPs), and size, situating GlottisNet as both the highest accuracy and most efficient.
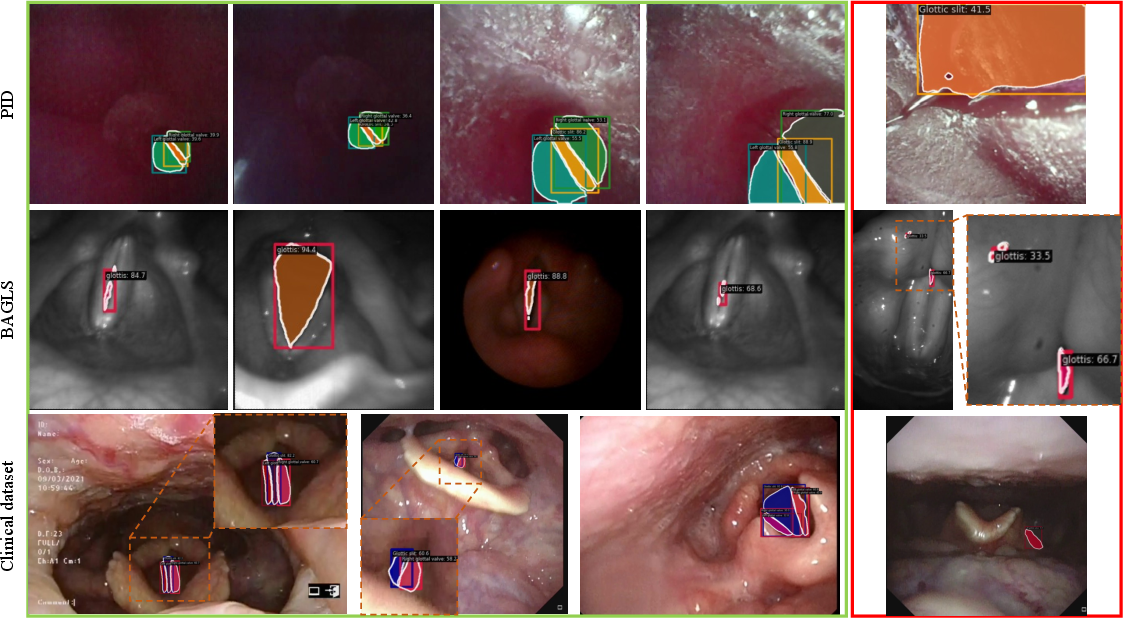
Figure 9: Qualitative segmentation results—correct detections dominate, failures occur only under extreme occlusion or imaging artifacts.
GlottisNet consistently surpasses SOTA Mask R-CNN, YOLACT, YOLOv8-seg, and other baselines both in accuracy and computational footprint, demonstrating superior scale and illumination robustness.
Practical and Theoretical Implications
GlottisNet’s architectural coupling of scale robustness and lightweight computation establishes new benchmarks for real-time, edge deployment in NTI and broader endoscopic navigation settings. Its redundancy (bounding box, segmentation mask) increases procedural safety in the event of transient anatomical occlusion. The methodology—modular design, adaptive cost-based sample assignment, and multi-receptive field fusion—can generalize to other medical visual segmentation problems with extreme morphological variability.
Future developments will focus on embedded systems (e.g., NVIDIA Jetson Nano), occlusion-resistant feature learning, system-level calibration, and closed-loop robotic integration for autonomous NTI beyond visual guidance. This paves the way for universal, portable NTI systems suitable for both clinical and out-of-hospital emergency contexts.
Conclusion
GlottisNet achieves state-of-the-art glottis segmentation and detection in NTI by synergizing multi-scale receptive field extraction, adaptive label assignment, and efficient, modular architecture. Its real-time operation and minimal computational requirements enable practical deployment on portable medical devices, directly addressing the clinical trade-off between precision and speed. The demonstrated efficacy across diverse, challenging datasets positions GlottisNet as a pivotal advance in vision-assisted airway management, with consequence for both clinical safety and wider AI-driven medical navigation.