- The paper demonstrates that domain-adapted partial fine-tuning of ECG foundation models yields superior multi-label SHD detection performance.
- It compares various transfer strategies, including frozen backbones, full adaptation, and parameter-efficient methods, using a large ECG dataset paired with echocardiographic labels.
- Results highlight an efficiency–performance trade-off with macro-AUROC of 0.8509, emphasizing scalable, low-cost ECG screening for structural heart disease.
Domain-Adapted Fine-Tuning of ECG Foundation Models for Multi-Label SHD Screening
Introduction and Motivation
Structural heart disease (SHD) encompasses a spectrum of cardiac abnormalities detectable via transthoracic echocardiography (TTE), the clinical reference standard. The prohibitive cost and logistical constraints of TTE motivate the use of electrocardiography (ECG) as a scalable noninvasive screening modality. Recent advances in deep learning, particularly in self-supervised foundation models (FMs) for ECG analysis, have suggested the potential of transfer learning to improve prediction of echocardiographically confirmed SHD from routine 12-lead ECGs. However, there remains uncertainty regarding optimal transfer strategies: the balance between freezing pretrained backbones, selective fine-tuning, utilization of in-domain self-supervised adaptation, and the practical implications for discrimination performance versus adaptation cost.
The paper presents a rigorous empirical analysis of transfer strategies using open ECG foundation models, with a benchmark on the public EchoNext Mini-Model cohort. It evaluates six echocardiographically defined endpoints, comparing engineered-feature gradient boosting models, randomly initialized end-to-end DEEPNNs, and multiple transfer learning configurations including full/frozen backbone approaches, partial fine-tuning, parameter-efficient adaptations (LoRA), late-fusion with covariates, and backbone/ensemble variations. The framework is summarized below.
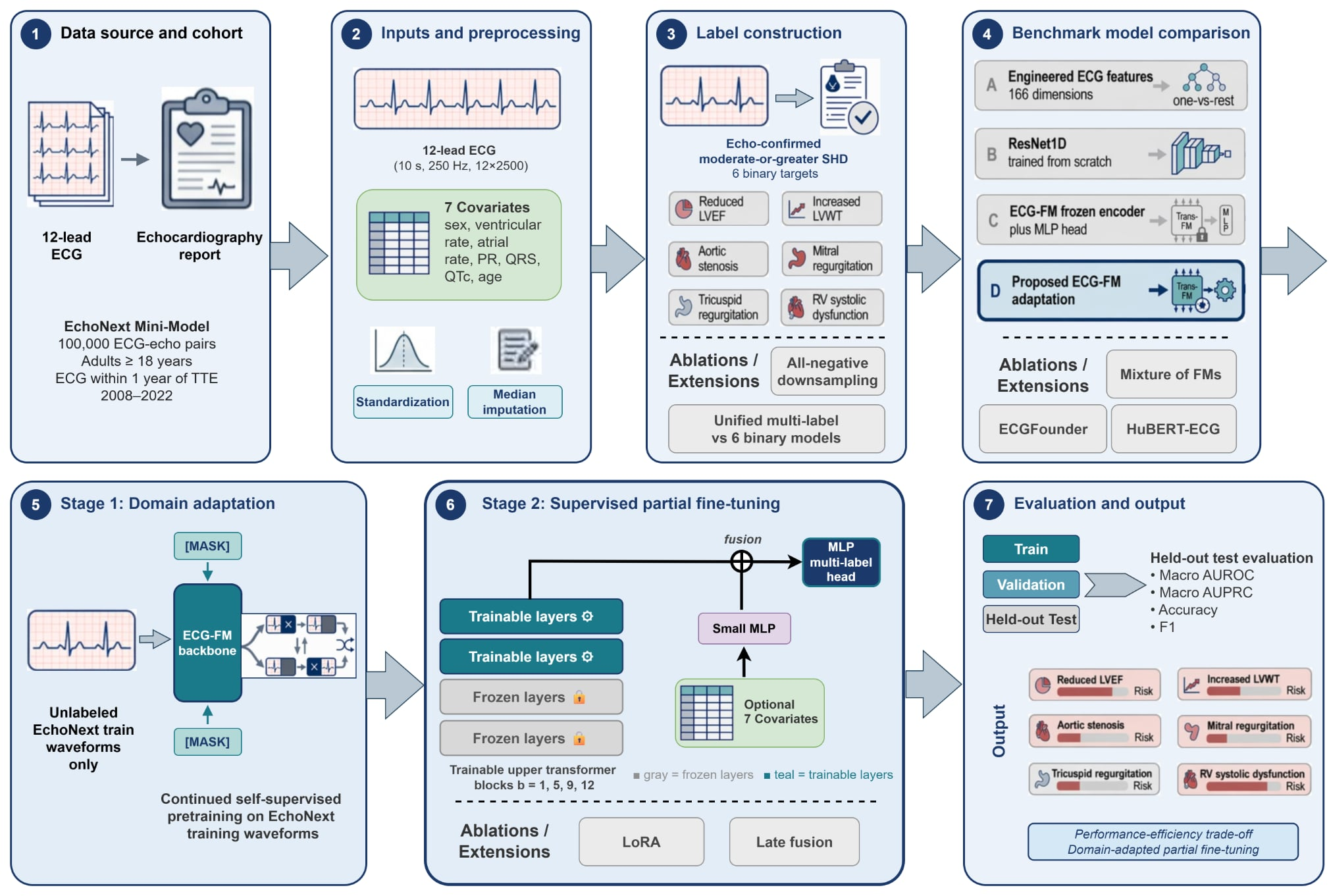
Figure 1: Methodological pipeline for multi-label SHD detection from 12-lead ECGs, delineating data provenance, endpoint derivation, model configurations, and key ablations.
Experimental Design and Benchmarks
Dataset and Task Definition
All experiments utilize the EchoNext Mini-Model v1.1.0 release: a large, publicly available dataset of 100,000 de-identified ECGs paired with echocardiography-derived SHD annotations. Each 12-lead, 10s ECG (sampled at 250 Hz) is preprocessed per the public benchmark, with additional tabular covariates (e.g., age, ventricular rate, PR interval) incorporated in selected fusion experiments. The six primary endpoints span ventricular systolic dysfunction, left ventricular hypertrophy, aortic stenosis, mitral regurgitation, tricuspid regurgitation, and right ventricular systolic dysfunction, all defined via standardized thresholds.
The task is cast as multi-label classification: D={(wi,ui,yi)}i=1N, with wi as waveform (12×2500 matrix), ui as covariates, and yi a $6$-dimensional binary vector.
Model Families
- Engineered Feature Baseline (A): Extraction of 166 engineered ECG descriptors with per-endpoint gradient boosting (XGBoost) classifiers.
- Random Initialization Baseline (B): 1D-ResNet18 trained end-to-end on waveforms.
- Adapted ECG-FM (C): Open ECG-FM backbone, continued self-supervised adaptation on EchoNext training data (wav2vec 2.0-style), followed by supervised probing with a frozen backbone.
- Partial Fine-Tuning: Following domain-specific SSL, upper b transformer layers (with L=12, b∈{1,5,9,12}), and in some cases convolutional stack, are fine-tuned while the rest of the model is frozen.
- Ablations: LoRA-based parameter-efficient updates, late-fusion of tabular covariates, alternative backbones (ECGFounder, HuBERT-ECG), mixture-of-experts (MoFM), and task-decomposed training.
Results
Main Performance Outcomes
Adapted ECG-FM models with partial supervised fine-tuning consistently yielded the highest discrimination metrics on held-out test sets. Maximal macro-AUROC (0.8509), macro-AUPRC (0.4297), and thresholded macro-F1 (0.3691) were achieved with only a subset (b=5 or wi0) of the transformer backbone adapted, representing a strong efficiency–performance trade-off. End-to-end randomly initialized deep models and frozen-backbone probes outperformed engineered-feature baselines, but not to the extent of selective adaptation. Updating the full model (including the convolutional frontend) provided no additional benefit, revealing redundancy in fully end-to-end adaptation. Notably, the frozen, in-domain SSL-adapted ECG-FM probe alone performed nearly as well as the ResNet1D baseline, demonstrating the strength of foundational representations.
Select ablation results demonstrated:
- Late fusion of additional covariates did not improve AUROC or AUPRC, indicating the latent waveform representation captures most predictive signal.
- LoRA parameter-efficient adaptation (rank-16) substantially reduced trainable parameter count (to wi1M) but did not match the discrimination of partial fine-tuning.
- Alternative backbones (ECGFounder, HuBERT-ECG) and mixtures-of-backbones (MoFM) did not surpass the best ECG-FM configuration and, in some metrics, slightly degraded AUROC and F1.
- Unified multi-label models outperformed ensembles of task-specific binary classifiers on macro-F1 (0.3691 vs 0.2769) and macro-AUPRC.
- All-negative label downsampling altered thresholded F1 rather than threshold-independent discrimination, primarily affecting calibration rather than overall discrimination.
Feature Importance in Engineered Baseline
Engineered features prioritizing morphology, multi-lead statistical relationships, and beat-to-beat variability contributed most to downstream discrimination (see Figure 2). However, performance plateaued after wi260 features, with diminishing returns from expanding feature sets.
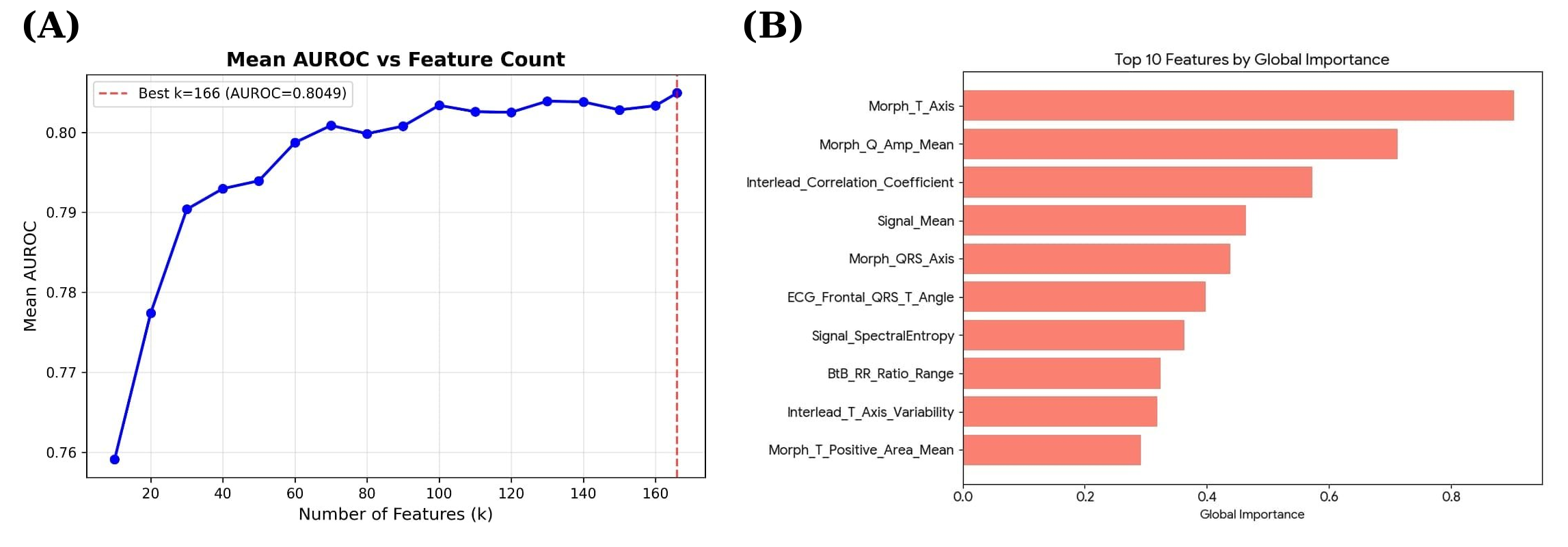
Figure 2: AUROC as a function of incremental feature count (left), and top 10 engineered feature importances (right) highlighting morphology, multi-lead, and beat-to-beat descriptors.
Latent Representation Analysis
Qualitative t-SNE visualization of foundation model embeddings (Figure 3) revealed considerable class mixing: false positives and false negatives from all SHD endpoints scattered widely with no clear cluster boundaries. This confirms the inherent difficulty of ECG-based SHD detection at an individual-instance level and the lack of simple separability in foundation model latent spaces, even post-adaptation.
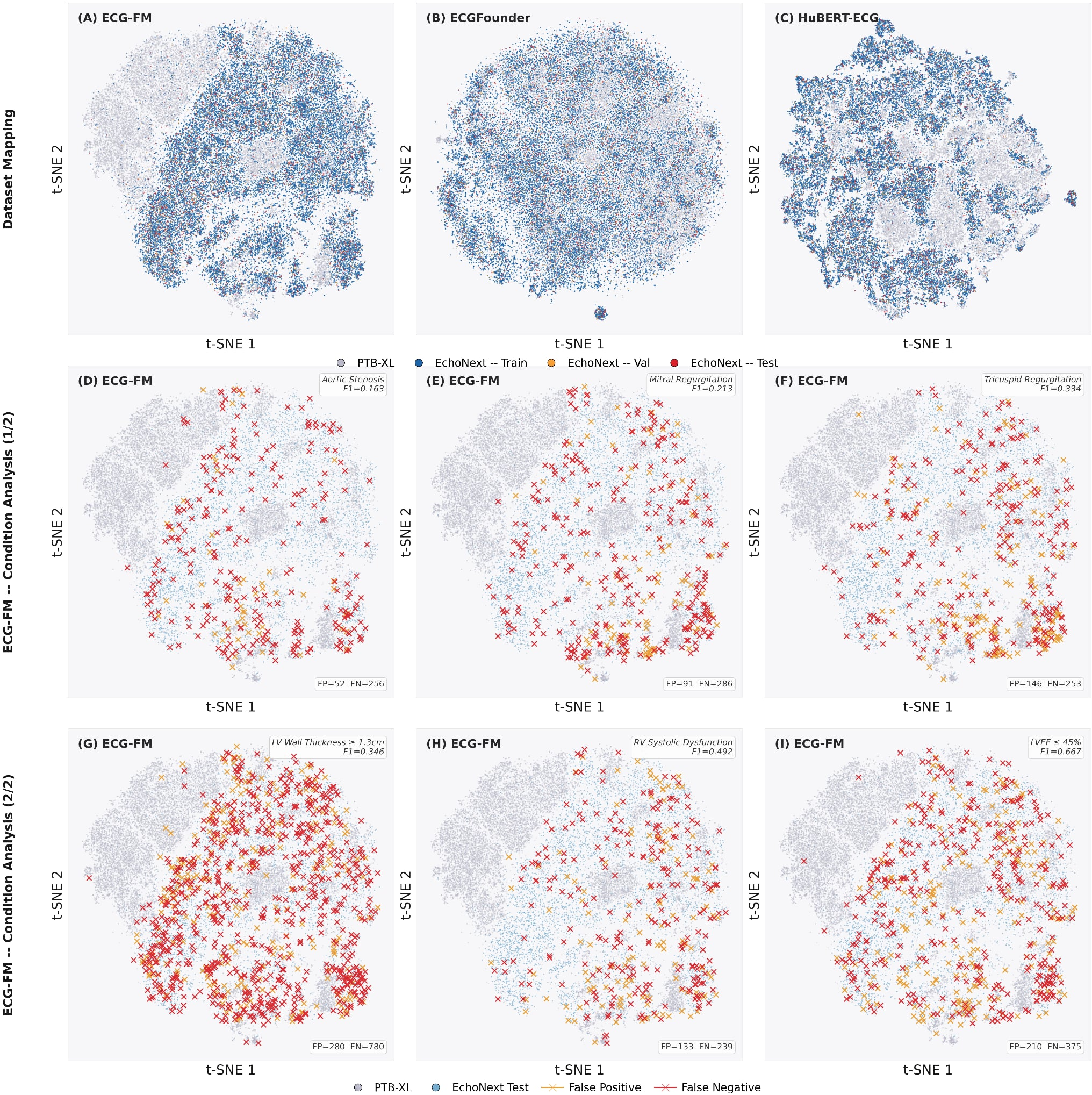
Figure 3: t-SNE projection of foundation model embeddings, with false positive/negative errors (colored) showing no clear segregation, reflecting the challenge of SHD detection from ECG alone.
Implications and Future Directions
This controlled analysis provides evidence that domain-adapted partial fine-tuning of open ECG foundation models is the most effective and resource-efficient strategy for multi-label SHD detection from routine ECGs, at least under current data and benchmark constraints. The marginal benefit of parameter-efficient adapters, auxiliary clinical covariates, and ensemble/mixed-backbone architectures is limited, emphasizing the primacy of waveform-based foundation models coupled with in-domain adaptation.
While these results highlight efficient transfer strategies for benchmarking, several clinical and methodological limitations persist:
- The dataset derives from a single health system without broad external validation.
- Labels are generated by structured report abstraction and imposed linkage rules, introducing possible misalignment between ECG and disease manifestation.
- Multi-label tasks outperform purely binary ensembles, but endpoint-specific calibration, subgroup performance, and thresholding for deployment remain outstanding clinical challenges.
Continued research should focus on expanded, multi-institutional external validation, assessment of calibration and subgroup invariance, and workflow integration to understand real-world impact. There is substantial opportunity for comparative analysis of additional open-source ECG FMs and domain-agnostic self-supervised adaptation techniques, especially as public datasets with paired echocardiography and ECG expand.
Conclusion
Domain-adapted selective supervised fine-tuning of pretrained ECG foundation models provides superior performance for multi-label detection of moderate-or-greater SHD from standard 12-lead ECGs when compared to both classical machine learning and full or frozen backbone approaches. These findings establish a best-practice protocol for foundation model utilization in clinically relevant cardiac screening benchmarks and inform future multi-modal and multi-center research aimed at enhancing accessible, low-cost SHD triage systems (2604.23385).