- The paper introduces a Transformer-DMM architecture that fuses multi-modal clinical data to forecast Alzheimer’s cognitive decline with a 24-month MMSE MAE of 1.619 and AUROC of 0.912.
- The methodology integrates cognitive tests, neuroimaging, biomarkers, and genetics through modality-specific embeddings and temporal dynamics to mitigate missing data impacts.
- The study demonstrates robust fairness and calibration across sex and age cohorts, underscoring its potential for personalized care planning and clinical trial enrichment.
CognitiveTwin: Multi-Modal Digital Twins for Forecasting Cognitive Decline in Alzheimer's Disease
Introduction
The paper "CognitiveTwin: Robust Multi-Modal Digital Twins for Predicting Cognitive Decline in Alzheimer's Disease" (2604.22428) introduces an advanced clinical AI framework designed for individualized forecasting of cognitive decline in AD patients. By leveraging multi-modal longitudinal clinical data and a composite Transformer-Deep Markov Model (DMM) architecture, CognitiveTwin provides robust patient-specific trajectory predictions. The approach is motivated by the limitations of classical statistical models and existing deep learning architectures in capturing nonlinear, heterogeneous, and temporally-evolving dynamics of AD progression, especially given the realities of missing data and the necessity for algorithmic fairness.
CognitiveTwin utilizes the TADPOLE subset of the ADNI dataset, covering 1,666 patients with longitudinal data across cognitive assessments, neuroimaging, biomarkers (PET/CSF), and genetics (APOE4 count). Data normalization and temporal alignment are strictly split-dependent to prevent leakage. Real-world clinical data incompleteness is acknowledged; modality-wise boolean masking strategies are employed to represent missingness. This structured multi-modality ensures the model reflects both the biological complexity and operational constraints found in AD cohorts.
Architecture
Each clinical modality (cognitive, biomarker, imaging, genetic) is projected via modality-specific MLPs into a shared latent space (dmodel=256). Source identity and temporal context are injected through learnable modality-type embeddings and standard positional encodings. Stacked Transformer encoder layers (h=8, L=4) employ cross-modal self-attention, enabling dynamic weighting and interaction among modalities per visit, effectively fusing heterogeneous signals into unified patient representations.
Deep Markov Model Dynamics
Temporal progression of disease is modeled within a DMM state-space framework, parameterizing latent state transitions and emissions via nonlinear, gated neural architectures. The DMM enables probabilistic latent inference, structured variational learning, and explicit separation between latent disease state (zt) and observable noisy measurements (xt). Posterior inference utilizes bidirectional GRUs; emission mapping is performed through three-layer MLPs, decoding fused latent states to specific clinical predictions. This design accommodates irregular sampling and missing data, as well as calibrated uncertainty propagation.
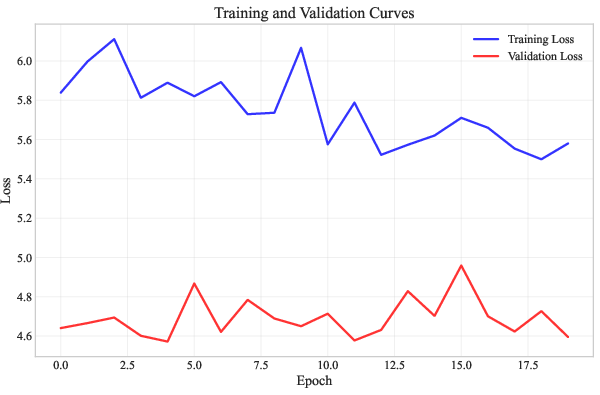
Figure 1: Training and validation loss curves over the optimization schedule, confirming effective regularization and convergence of the DMM.
Evaluation Protocol
Performance is assessed using multiple metrics: MAE and RMSE for regression (primary endpoint: 24-month MMSE), R2 for variance explanation, AUROC for binary progression classification, and Expected Calibration Error (ECE) for reliability. Robustness is evaluated via a simulated 15% MNAR scenario, masking structural MRI features in high-risk (MMSE<24) visit segments. Comprehensive fairness audits are performed across biological sex and age cohorts.
Results
CognitiveTwin achieves a 24-month MMSE MAE of 1.619, RMSE of 2.248, and R2=0.682, closely matching the test-retest variability of MMSE and indicating precise model calibration. Progression event classification yields AUROC=0.912, demonstrating strong discriminative power. Residual analysis reveals homoscedastic, zero-centered, normally distributed errors with no systematic directional bias.
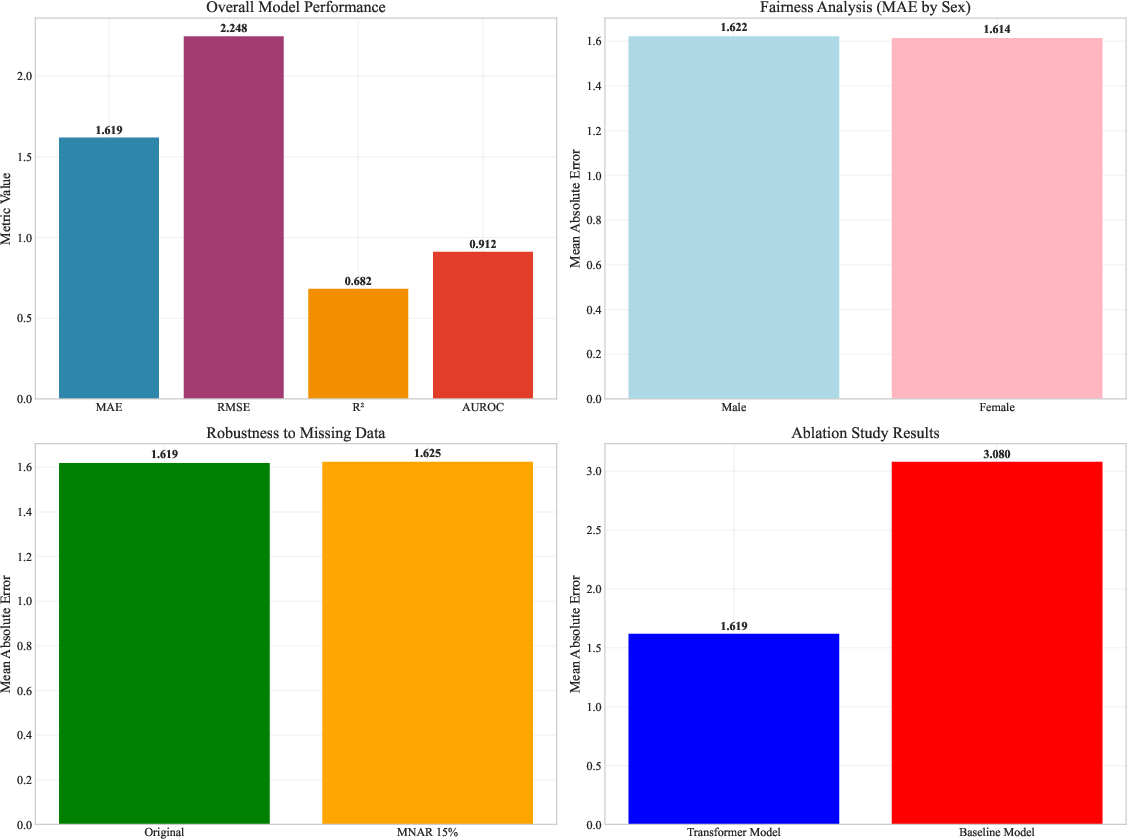
Figure 2: Comprehensive performance summary—predictive accuracy, fairness, MNAR robustness, and ablation.
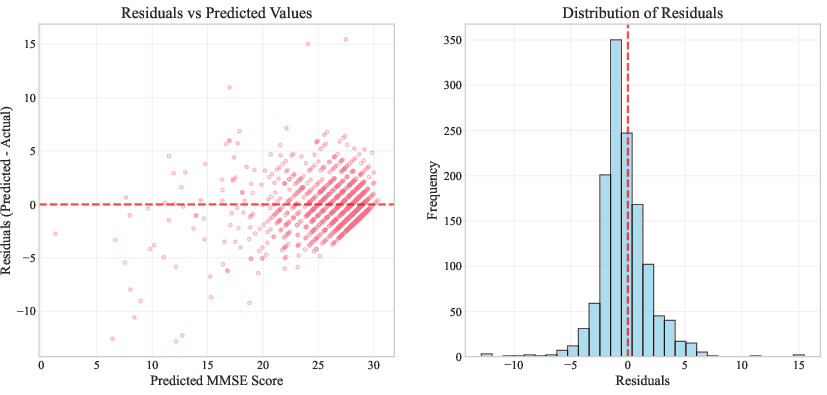
Figure 3: Predictive residuals show statistical neutrality and absence of structural bias.
Robustness and Ablation
Simulated MNAR drops MRI for 15% of low-MMSE visits; MAE increases minimally (%Δ=0.3), validating the DMM's latent resilience. Removal of temporal dynamics (static baseline) results in catastrophic degradation (MAE=3.08, degradation=90.2%). Exclusion of genetics (APOE4) or multi-modality leads to measurable, though less severe, performance loss, confirming their contribution. Temporal modeling and multi-modal fusion are necessary for state-of-the-art accuracy and discriminative capacity.
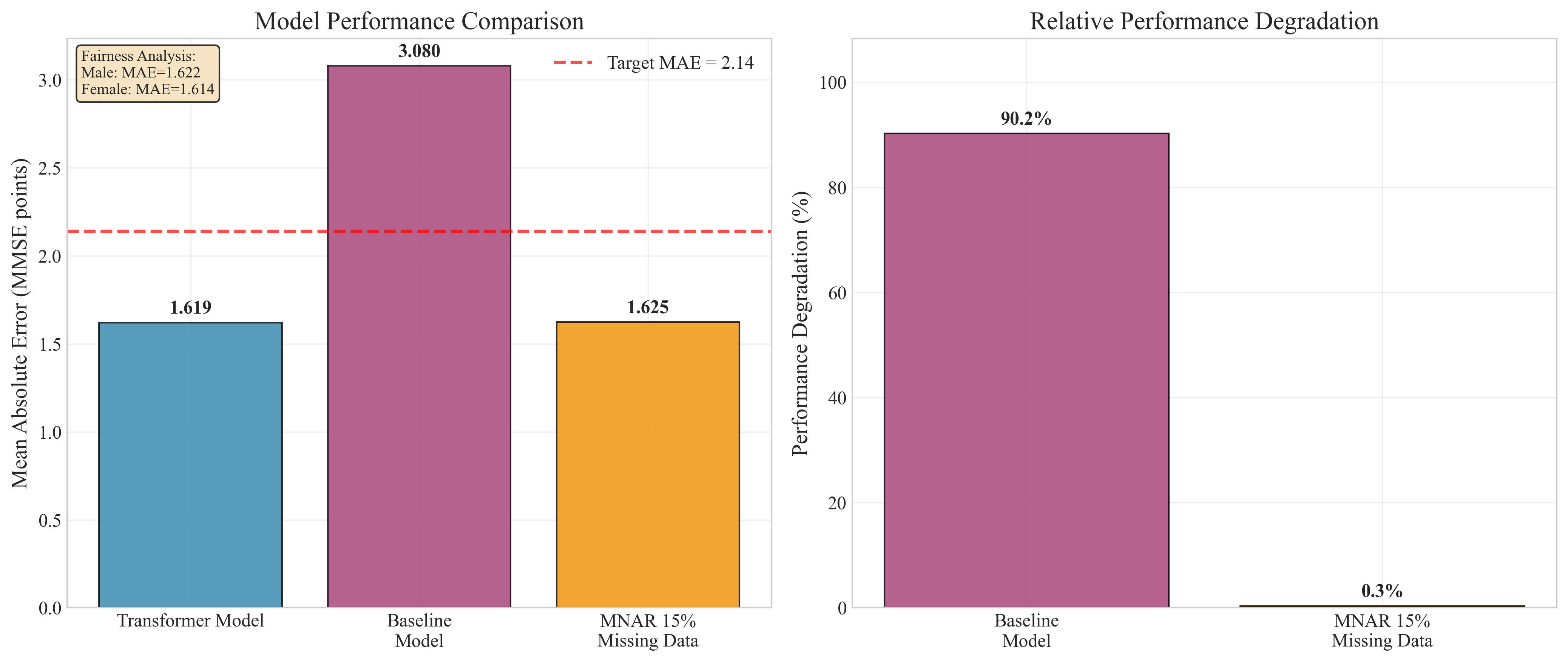
Figure 4: Ablation and MNAR robustness—MAE and relative degradation under architectural modifications and data loss.
Fairness and Calibration
Strict demographic parity is demonstrated: male MAE=1.622, female MAE=1.614 (difference=0.008); age stratification shows maximum gap of 0.027. Uniform calibration (ECE=0.054) is maintained across all subgroups. Reliability diagrams display tight adherence to ideal calibration.
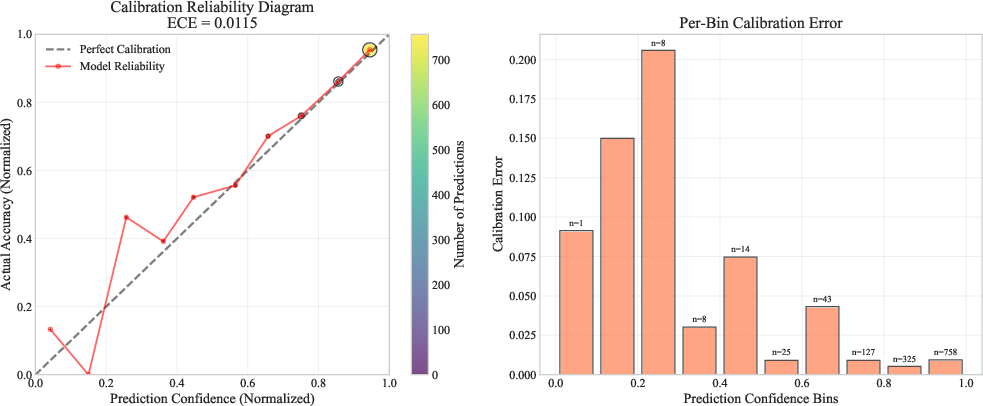
Figure 5: Calibration reliability—predicted risk closely tracks empirical accuracy across bins.
Individualized Forecasting
Patient-level forecasts illustrate the model's clinical value: steep 22-point MMSE declines are anticipated and encapsulated within well-calibrated 95% uncertainty intervals. Trajectory-level accuracy, with appropriate risk quantification, addresses key requirements for both clinical care planning and trial enrichment.
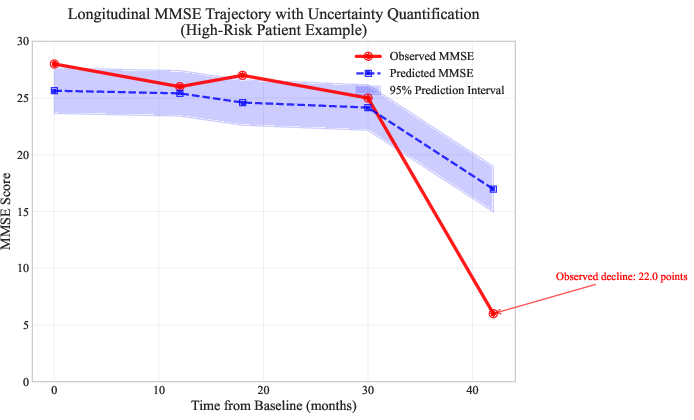
Figure 6: Trajectory forecast for a high-risk patient shows precise tracking and uncertainty quantification.
Implications and Limitations
Clinical Utility
CognitiveTwin shifts neurodegenerative prognosis from cross-sectional, population-level averages to dynamic, individualized forecasting. The generative latent state modeling allows the framework to operate robustly in the presence of MNAR missingness, a critical requirement in longitudinal AD studies. Algorithmic fairness and calibration enhance its utility as a clinical support tool, ensuring safe deployment across diverse populations.
Architectural Impact
The combined Transformer-DMM architecture delivers substantial advantages over classical statistical approaches, LSTM baselines, and late-fusion networks. Explicit state-space modeling, cross-modal attention, and latent uncertainty quantification enable accurate multi-year forecasts and actionable risk stratification.
Limitations
Biases inherent in the ADNI cohort (overrepresentation of highly-educated, less diverse subjects) limit generalizability. Computational demands are nontrivial, especially during model training and fine-tuning. The model's reliance on standardized clinical features (e.g., MRI volumetrics, CSF assays) may require harmonization for heterogeneous, real-world EHR data. Prospective, multi-site validation remains necessary.
Future Directions
Integration with EHR systems, automated clinical pipeline adaptation, and real-time multimodal extraction are critical for transitioning to clinical practice. Further work should explore cross-site, real-world deployment and investigate the impact of AI-driven forecasting on therapeutic decision-making and patient outcomes. Advanced harmonization techniques and meta-learning approaches may mitigate cohort bias and measurement drift.
Conclusion
CognitiveTwin demonstrates robust, fair, and precise forecasting of cognitive decline in Alzheimer's disease. The model achieves MAE=1.619 and AUROC=0.912, maintains parity and calibration across demographics, and resists performance loss under MNAR missingness (0.3% degradation). The state-space digital twin paradigm, integrating Transformer fusion and DMM latent dynamics, enables personalized clinical trajectory simulation and supports individualized care planning and trial design. This work signals a practical step toward precision medicine in neurodegenerative diseases.