- The paper introduces a topology-driven fusion method that integrates nnU-Net and MedNeXt to correct topological errors and enhance boundary precision in glioma segmentation.
- The study demonstrates that ensemble modeling with a universal topology refinement module improves NSD metrics while slightly trading off Dice scores, ensuring robust performance on low-field MRI data.
- The research validates the method on the BraTS-Africa dataset, proving its effectiveness in resource-limited settings with diverse imaging protocols and imaging artifacts.
Topology-Driven Fusion of nnU-Net and MedNeXt for Robust Brain Tumor Segmentation in Sub-Saharan Africa
Introduction
The segmentation of gliomas in brain MRI data is a fundamental task in neuro-oncology, enabling precise surgical planning, treatment monitoring, and assessment of tumor progression. In resource-limited settings such as Sub-Saharan Africa (SSA), the challenge is exacerbated by variable imaging protocols, low-field MRI scanners, and distinctive image artifacts, as reflected in the BraTS-Africa dataset. Traditional architectures—while successful in high-quality, standardized datasets—encounter barriers to generalization and boundary accuracy on these heterogeneous clinical datasets.
This paper proposes a topology-driven fusion approach by ensembling nnU-Net and MedNeXt, further augmented by a universal topology refinement module, to mitigate topological errors and improve segmentation accuracy for gliomas in the BraTS-Africa dataset (2604.15964). The methodology addresses both pixel-wise overlap and boundary-level consistency, showcasing measurable improvements in region-wise segmentation and topological correctness across challenging modalities.
Methodology
Dataset and Preprocessing
The BraTS-Africa dataset encompasses pre-operative glioma cases with volumetric MRI spanning T1-weighted, T2-weighted, post-contrast T1-weighted (T1c), and T2-FLAIR sequences. Tumor subregions are annotated as enhancing tumor (ET), non-enhancing tumor core (NETC), and surrounding non-enhancing FLAIR hyperintensity (SNFH). Standard BraTS protocols are employed for preprocessing.
Model Architectures
Baseline nnU-Net
3D full-resolution nnU-Net is configured with six encoder-decoder levels (32–320 features) and uniform 3×3×3 kernel sizes. Deep supervision and batch normalization are incorporated given the limited batch size.
Baseline MedNeXt
MedNeXt, inspired by ConvNeXt and 3D U-Net, is employed with six residual stages, depthwise convolution, channel-wise normalization, and GELU activation. Deep supervision stabilizes training and enhances gradient flow.
Ensemble and Topology Refinement
Softmax outputs from nnU-Net and MedNeXt are combined via soft-voting. A universal topology refinement module, as proposed by Liu et al., synthesizes topology-perturbation masks using orthogonal polynomial bases, introducing structural perturbations for robust post-processing and error correction.
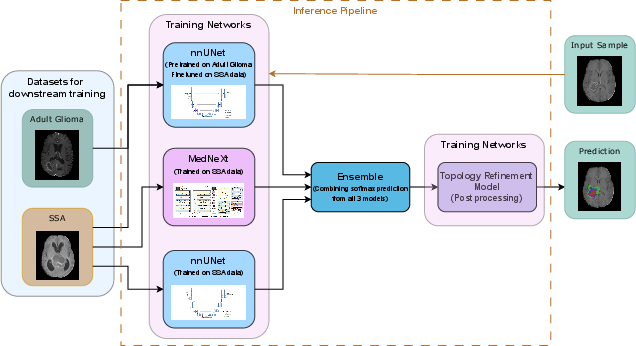
Figure 1: Proposed segmentation pipeline combining an ensemble of nnU-Net and MedNeXt with topology-aware post-processing refinement.
Training and Fine-tuning
Models are pre-trained on BraTS2025 adult glioma (Task 1) and fine-tuned on the BraTS-Africa dataset. Training is conducted on both 2D slice-based and 3D volumetric inputs for 500 epochs, leveraging data augmentation and standard preprocessing.
Results
Topological and Boundary Error Analysis
The study demonstrates the prevalence of topological errors in boundary regions when using baseline models, particularly on low-quality images. The topology refinement module visibly corrects these artifacts, improving boundary alignment.
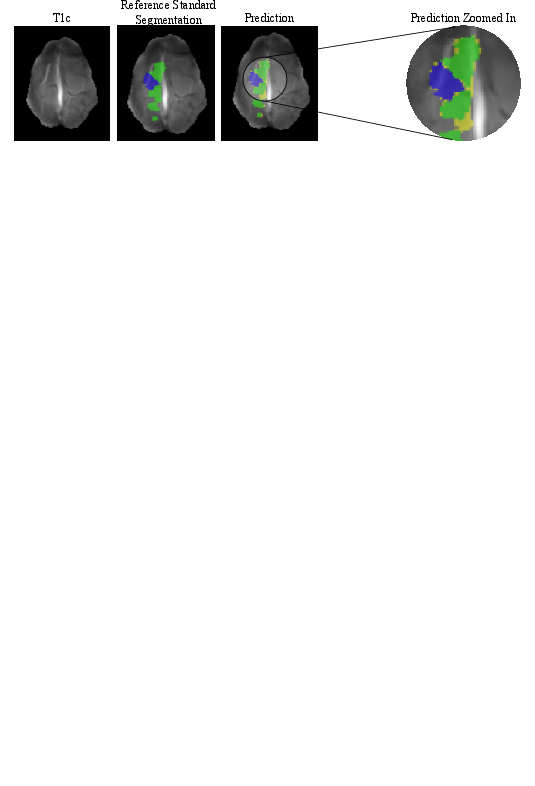
Figure 2: Visualization of segmentation topological error: yellow denotes prediction error, highlighting mismatches at boundaries prior to refinement.
Quantitative Evaluation
The best-performing configuration achieves Dice scores of 0.930 (SNFH), 0.906 (NETC), and 0.906 (ET) on nnU-Net 3D full-resolution. Fine-tuning with BraTS2025 increases legacy Dice scores to 0.936 (SNFH), 0.907 (NETC), 0.907 (ET). The topology-aware module yields NSD@1.0 values of 0.810 (SNFH), 0.829 (NETC), 0.895 (ET). Notably, improvements in NSD reflect enhanced boundary accuracy and topological consistency at the cost of slightly lower dice scores, suggesting a trade-off.
Visual Validation
Segmentation overlays on multimodal MRI input display close alignment between predictions and ground truth, validating the methodology across multiple cases.
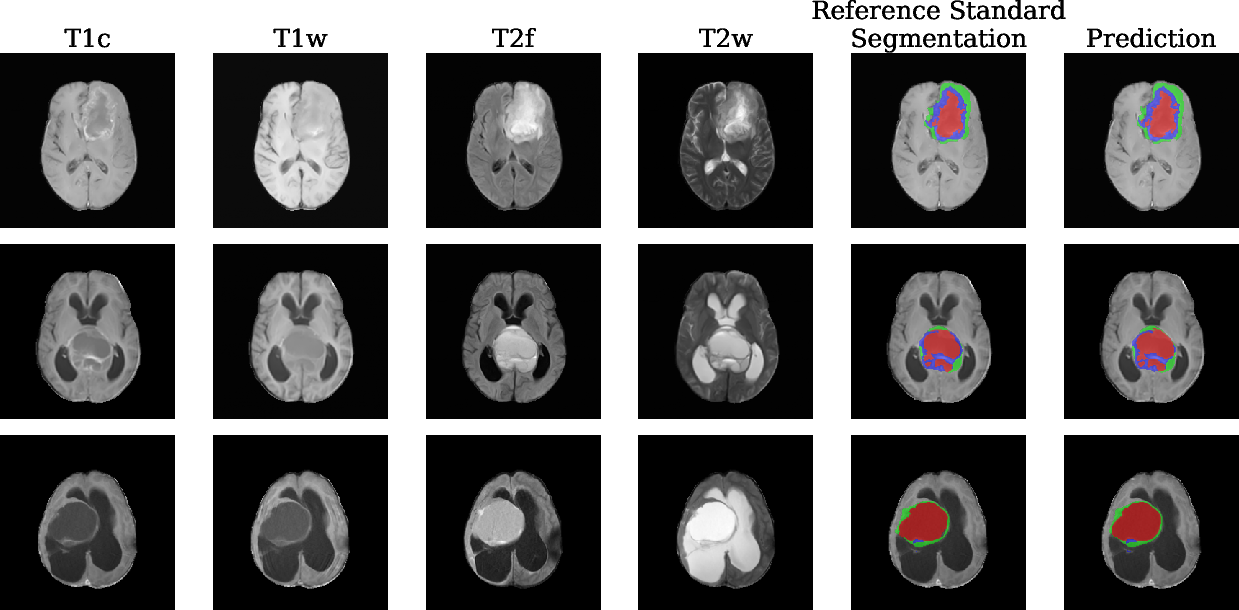
Figure 3: Side-by-side visualization of multimodal MRI and segmentation overlays; model predictions closely match reference standard annotations in multiple tumor subregions.
Moreover, multiplanar visualization (axial, coronal, sagittal) facilitates cross-model comparison, illustrating the superior delineation and consistency achieved by the ensemble and topology-aware refinements.
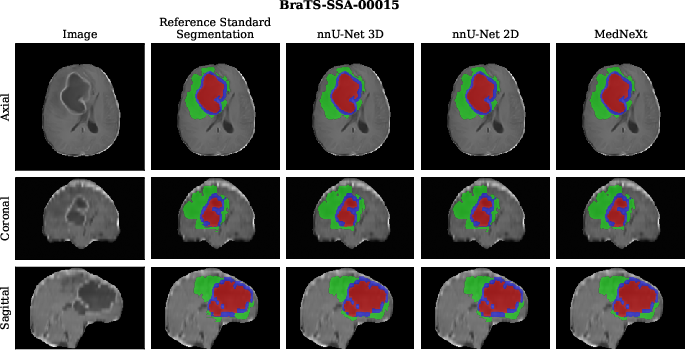
Figure 4: Multiplanar view comparing predictions from nnU-Net 3D, nnU-Net 2D, and MedNeXt; overlays highlight differences in tumor boundary delineation.
Discussion
The results indicate that the nnU-Net baseline exhibits robust performance across tumor subregions, with MedNeXt providing competitive region-wise metrics. Ensemble modeling and topology refinement enhance boundary alignment and surface consistency, as measured by NSD, but may slightly compromise volumetric Dice scores. This outcome underscores the trade-off between topological preservation and conventional overlap metrics, raising critical questions regarding segmentation quality evaluation in clinical practice.
The universal topology refinement method demonstrates utility in correcting model errors otherwise persistent in heterogeneous, low-field MRI data. However, further architectural enhancement and loss function optimization could yield more balanced improvements across both dice and NSD metrics. The methodology provides a scalable pipeline for future segmentation models targeting resource-constrained clinical datasets.
Implications and Future Directions
The practical impact of this approach is evident in improved segmentation accuracy for underrepresented populations and imaging environments, facilitating automated workflows in LMICs where clinical resources are limited. Theoretically, the integration of topology-aware refinements paves the way for broader adoption of robust segmentation pipelines that optimize not only pixel-wise overlap but also boundary topological correctness.
Future work should focus on advanced topology-aware loss functions, exploration of hybrid architectures, and expansion of model validation across larger, diverse clinical populations. Additionally, the trade-offs elucidated between dice metrics and NSD incentivize the adoption of multi-metric performance evaluation standards in medical image segmentation.
Conclusion
The topology-driven fusion approach combining nnU-Net, MedNeXt, and universal topology refinement addresses critical segmentation challenges in the BraTS-Africa dataset. The methodology improves boundary precision and topological correctness, with measurable gains on NSD metrics, albeit with modest trade-offs in volumetric Dice scores. Continued refinement of topology-aware models and evaluation metrics will be essential for advancing automated brain tumor segmentation in resource-constrained clinical settings.