- The paper demonstrates that quantum neural networks improve sensitivity to 83.3% in predicting anastomotic leaks compared to classical methods.
- It employs a 4-qubit variational circuit with a ZZFeatureMap to project clinical features into a high-dimensional space for enhanced risk stratification.
- Quantum models using the ESU2 ansatz and gradient-free optimizers achieve competitive AUC and superior calibration under realistic NISQ noise conditions.
Quantum Machine Learning for Colorectal Cancer: Anastomotic Leak Classification and Risk Factors
Clinical Challenges and Quantum Motivation
Anastomotic leak (AL) after colorectal cancer (CRC) resection represents a critical surgical complication with high mortality. Predicting AL is fundamentally constrained by both multifactorial etiology and pronounced class imbalance: the minority (leak) class occurs in only 14% of the clinical cohort. The paper constrains its feature space to four physiologically interpretable predictors—Diabetes Mellitus (DM), smoking history, intraoperative NoCoil drain insertion, and left colic artery preservation (ACSP)—reflecting established clinical evidence on microvascular compromise and mechanical risk factors.
Classical ML surrogates (logistic regression, AdaBoost, MLP) consistently fail to reach adequate sensitivity, plateauing at 66.7%. Given the severe penalty for false negatives in clinical practice, this motivates the exploration of Quantum Neural Networks (QNNs) as a route to high-dimensional feature spaces that may resolve minority class boundaries otherwise missed by classical hyperplanes.
Quantum Framework: Circuit Design and Optimization
The QML approach utilizes a 4-qubit parameterized variational circuit. Data is encoded using the ZZFeatureMap, which imposes second-order expansions and multi-qubit entanglement, thereby enabling projection into a 2n dimensional Hilbert space. Two circuit ansatze are benchmarked:
- RealAmplitudes (RA): Shallow real-domain parameterization via Ry rotations and CNOTs.
- EfficientSU2 (ESU2): Enhanced expressivity with additional Rz rotations.
The classification output is extracted via the expectation value of a Pauli-Z operator on the first qubit, mapped to probability space using a classical sigmoid function. All experiments are simulated under realistic NISQ noise conditions (depolarizing channel, gate error pgate=0.05, 1024 measurement shots).
Classical and metaheuristic optimizers are evaluated: SLSQP, BFGS (gradient-based), and CMA-ES, COBYLA, SPSA (gradient-free). Each configuration is statistically validated across 10 independent runs.
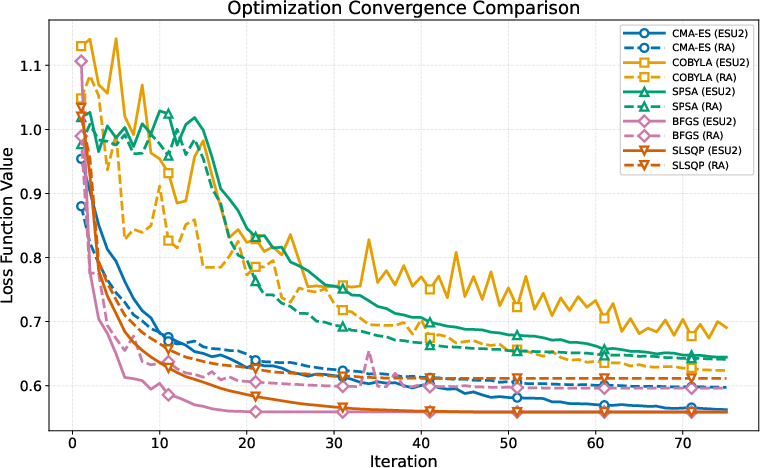
Figure 1: Mean convergence for RA and ESU2 circuits under varied optimizers, highlighting optimizer stability amidst quantum noise.
Quantum models using ESU2 paired with BFGS achieved AUC parity (0.809) with the classical upper bound (Gaussian Naive Bayes), but importantly rebalanced sensitivity-specificity. All QNN variants demonstrated a consistent sensitivity of 83.3%—a robust 16.6% margin over classical methods—while maintaining reasonable specificity (79.4%). Classical models, in contrast, displayed specificity biases (≥88.2%) and stagnated sensitivity.
The ESU2 feature map also yielded lower Brier Scores (0.111) and Log Loss (0.372), providing superior calibration compared to classical MLP miscalibration. Population-based optimizers such as CMA-ES outperformed gradient descent in the presence of noise, circumventing local minima and enhancing minority class Average Precision.
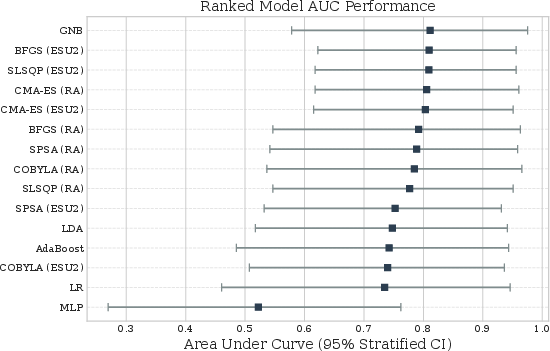
Figure 2: Bootstrapped AUC confidence intervals for all model variants, with QNNs matching classical benchmarks in discrimination power.
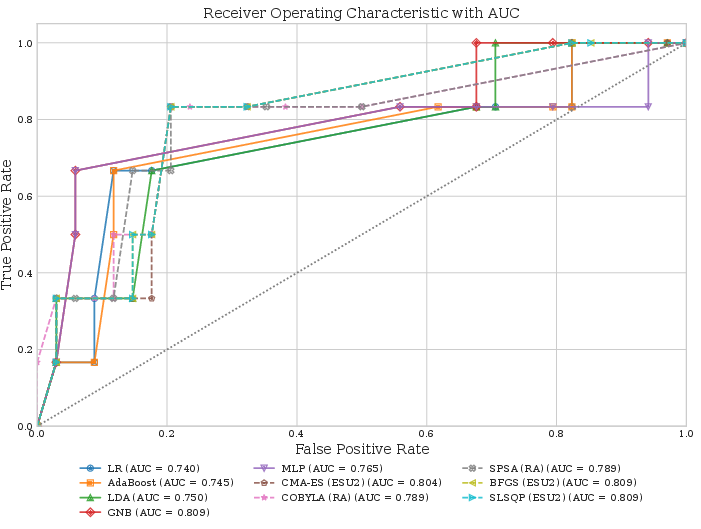
Figure 3: ROC comparison of classical baselines versus QNN configurations, underscoring sensitivity gains in quantum models.
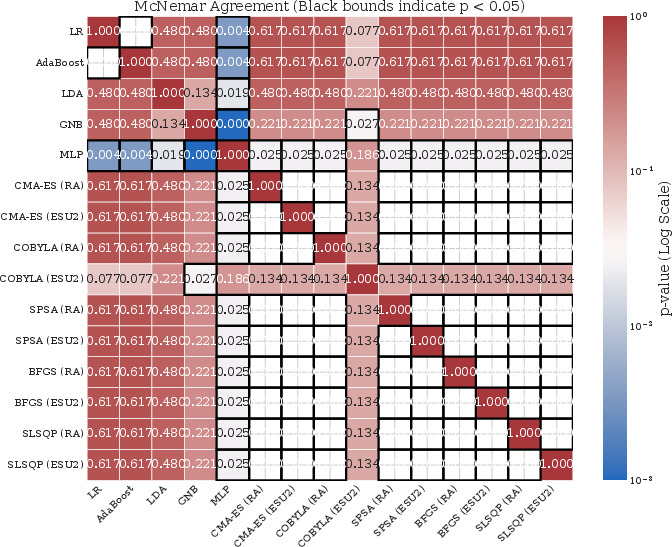
Figure 4: McNemar matrix for classifier agreement; statistically significant divergence in QNN output patterns relative to classical surrogates.
Methodological Implications and Future Directions
The findings fundamentally reposition quantum variational circuits as competitive classifiers for rare-event biomedical risk prediction in noisy regimes. The observed sensitivity shift is attributed to the high-dimensional quantum feature space, which augments class separability, and to the robustness of gradient-free optimization in decohered environments.
Practical deployment will require advancements in quantum hardware error mitigation (to address loss landscapes and barren plateaus), and post-hoc probability calibration (Platt scaling, isotonic regression). Theoretical work should focus on characterizing quantum inductive bias and contextuality, exploring whether quantum contextuality and group-invariant encoding can yield topological advantages for overlapping risk factors.
Further, quantum expressivity and generalization must be analytically bounded as qubit count increases to avoid over-orthogonal feature mappings and poor extrapolation. Integrating calibration-aware loss objectives and rigorous hardware benchmarking is essential for translational impact.
Conclusion
This study demonstrates that quantum machine learning architectures, specifically QNNs with expressive feature maps, can outperform classical ML surrogates in sensitivity-driven clinical classification tasks, especially for highly imbalanced data. Despite parity in global discrimination metrics, quantum models fundamentally alter the probability landscape, enabling more accurate resolution of minority class events. The work establishes a computational pilot for quantum-enhanced risk stratification in clinical settings, identifying critical optimization and architectural trade-offs that will guide future hardware deployment and algorithmic development (2604.13951).

