- The paper introduces a modular pipeline that combines a CausalVAE and Bayesian causal graphs to achieve traceable, evidence-based ECG diagnoses.
- The methodology supports counterfactual queries by identifying minimal edits to latent biomarkers, thereby reducing the risk of over-diagnosis.
- Experimental results demonstrate improved diagnostic accuracy and significantly lower hallucination rates compared to conventional ECG-LLM systems.
Causal Agent-based Reasoning for Counterfactual and Explainable ECG Interpretation
Introduction and Clinical Motivation
Automated ECG interpretation has evolved significantly with LLMs, yet clinical deployment mandates not only accuracy but also faithfulness, causal traceability, and robustness to hallucination. Existing ECG-LLM systems typically rely on weakly aligned signal-text matching and retrieval techniques that lack explicit physiological or causal modeling, leading to clinically risky over-diagnosis or unsupported mechanistic explanations (Figure 1).
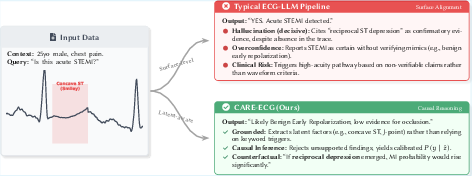
Figure 1: Typical ECG-LLMs hallucinate confirmatory evidence for diagnoses, whereas CARE-ECG mitigates this through reasoning on latent morphological biomarkers and validation via counterfactuals.
CARE-ECG Framework Architecture
CARE-ECG introduces a modular pipeline wherein multi-lead ECGs are encoded via a CausalVAE into temporally organized latent biomarkers, enabling downstream graph-based causal inference. The architecture decomposes reasoning into a Physiological Stream (feature encoding, Bayesian causal graph, and counterfactuals) and an Agentic Stream (causal retrieval-augmented generation and verifier-based explanation correction). The output is a posterior over diagnoses, an explanation grounded in evidence, and a counterfactual assessment.
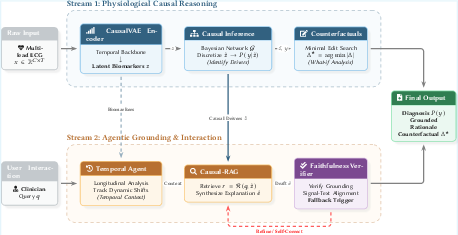
Figure 2: The CARE-ECG framework integrates a signal-wise latent encoder, causal inference, retrieval-guided explanation, and a faithfulness verifier in a modular pipeline.
The agentic reasoning workflow formalizes how temporal context (Δz) and inferred causal drivers (z~) are incorporated in the rationale generation and its verification.
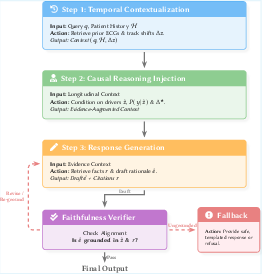
Figure 3: CARE-ECG’s agentic workflow, sequencing context integration, causal reasoning, and faithfulness-triggered self-correction.
Methodological Innovations
Latent Biomarker and Causal Graph Modeling
The core of CARE-ECG's clinical alignment lies in transforming ECG signals into a set of quantile-binned latent biomarkers (z~) via a CausalVAE backbone. These serve as explicit nodes in a Bayesian causal network encompassing both biomarkers and diagnosis labels, and the graph topology is initialized with clinical priors, then refined via data-driven structure learning. Probabilistic inference over this graph yields posterior diagnosis distributions and unveils the minimal effective subset of physiological features supporting each prediction, facilitating auditability and sensitivity analysis.
Counterfactual Reasoning
CARE-ECG supports clinical "what-if" queries by identifying minimal edits to the biomarker set (z~) that would suffice to change a diagnosis, via discrete search within the learned causal graph. Unlike black-box counterfactual generation, this process exposes the physiological axis along which a disease prediction is particularly sensitive.
Causal RAG and Faithfulness Verification
Retrieval-augmented generation is conditioned explicitly on both the latent biomarkers and diagnostic hypotheses, enriching the context with pathophysiologically relevant evidence rather than mere query matching. A fuzzy-matching faithfulness verifier estimates hallucination risk and triggers fallback to evidence-only explanations if unsupported claims are likely, thereby minimizing hallucination without degenerating into generic or shallow outputs.
Experimental Results
CARE-ECG is evaluated on PTB-XL (structured diagnostic code mapping), MIMIC-IV ECG (retrieval-faithfulness), and Expert-ECG-QA (interactive clinical reasoning). All comparisons control for LLM backbone (GPT-4, LLaMA 3--8B) and retrieval settings.
CARE-ECG yields superior accuracy on diagnostic QA (0.84 on Expert-ECG-QA and 0.76 on SCP-mapped PTB-XL for GPT-4 backbone), maintaining superiority across all metrics (accuracy, precision, recall, F1) and across both proprietary and open models. Causal Retrieval Coverage (CRC), groundedness, and context relevance are each highest for CARE-ECG (up to 0.96 CRC on Expert-ECG-QA).
CARE-ECG achieves the lowest hallucination rates (0.05–0.08 across datasets and backbones), without sacrificing explanation specificity, as measured by Summary Relevance Score (SRS). This simultaneous reduction in hallucination and maintenance of semantic richness is evident in the multi-metric (HR–SRS) trade-off visualization.
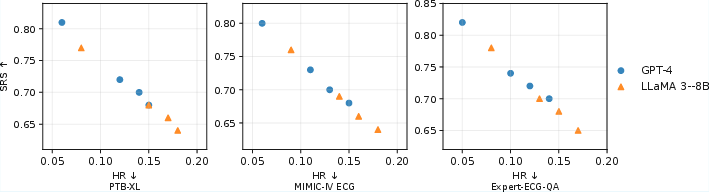
Figure 4: Each method’s faithfulness–robustness trade-off (HR vs. SRS); CARE-ECG achieves consistently favorable positioning.
A staged ablation reveals that incremental addition of causal graphs, causal RAG, and the verifier module yield monotonic improvements in causal alignment, evidence consistency, and hallucination suppression. The counterfactual module offers further small but consistent gains in mechanistic robustness.
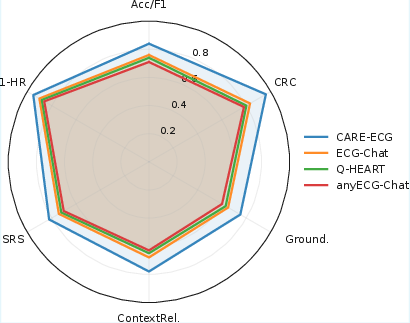
Figure 5: Radar plot summarizing CARE-ECG’s dominance across correctness, evidence alignment, and robustness axes.
Analysis and Implications
The results establish that explicit causal structuring offers unique value beyond prior LLM-based ECG systems. The CARE-ECG pipeline is not simply more accurate, but also more transparent, as explanations are anchored in traceable latent drivers and explicit evidence paths. Unlike purely generative or retrieval-augmented LLM approaches, this causal-and-agentic design constrains the space of plausible rationales, reducing hallucinations even in adversarial QA or ambiguous clinical contexts.
Nonetheless, the interpretation of causal graphs constructed from observational data remains a limitation; the edges offer predictive interpretability but cannot guarantee true interventional causality. The latent axis, while informative, may not perfectly map to hand-crafted ECG features. Further supervised alignment between latent variables and standard measurements, as well as controlled perturbation experiments, are warranted.
Practical advances include improved robustness to hallucinated waveform findings, enhanced auditability for regulatory scrutiny, and more reliable support for evidence-based clinical decisions. Theoretical implications extend to the broader design of LLM-based decision support: integrating explicit causal inference layers and evidence-verification gates is critical for safe AI deployment in any high-stakes biomedical setting.
Conclusion
CARE-ECG substantially advances explainable ECG–language reasoning through a pipeline combining causal biomarker inference, Bayesian graph-based diagnosis, minimal-edit counterfactuals, causal-conditioned retrieval, and faithfulness-verification. Empirical gains in accuracy, causal/evidence consistency, and hallucination suppression are consistently realized across both closed and open LLM backbones. Future research will seek to strengthen physiological interpretability and interventional reliability, and to generalize the causal-agentic paradigm to other medical time-series interpretation tasks.

