Improving Deep Learning-Based Target Volume Auto-Delineation for Adaptive MR-Guided Radiotherapy in Head and Neck Cancer: Impact of a Volume-Aware Dice Loss
Published 11 Apr 2026 in cs.CV | (2604.10130v1)
Abstract: Background: Manual delineation of target volumes in head and neck cancer (HNC) remains a significant bottleneck in radiotherapy planning, characterized by high inter-observer variability and time consumption. This study evaluates the integration of a Volume-Aware (VA) Dice loss function into a self-configuring deep learning framework to enhance the auto-segmentation of primary tumors (PT) and metastatic lymph nodes (LN) for adaptive MR-guided radiotherapy. We investigate how volume-sensitive weighting affects the detection of small, anatomically complex nodal metastases compared to conventional loss functions. Methods: Utilizing the HNTS-MRG 2024 dataset, we implemented an nnU-Net ResEnc M architecture. We conducted a multi-label segmentation task, comparing a standard Dice loss baseline against two Volume-Aware configurations: a "Dual Mask" setup (VA loss on both PT and LN) and a "Selective LN Mask" setup (VA loss on LN only). Evaluation metrics included volumetric Dice scores, surface-based metrics (SDS, MSD, HD95), and lesion-wise binary detection sensitivity and precision. Results: The Selective LN Mask configuration achieved the highest LN Volumetric Dice Score (0.758 vs. 0.734 baseline) and significantly improved LN Lesion-Wise Detection Sensitivity (84.93% vs. 81.80%). However, a critical trade-off was observed; PT detection precision declined significantly in the selective setup (63.65% vs. 81.27%). The Dual Mask configuration provided the most balanced performance across both targets, maintaining primary tumor precision at 82.04% while improving LN sensitivity to 83.46%. Conclusions: A volume-sensitive loss function mitigated the under-representation of small metastatic lesions in HNC. While selective weighting yielded the best nodal detection, a dual-mask approach is required in multi-label tasks to maintain segmentation accuracy for larger primary tumor volumes.
The paper demonstrates that incorporating a volume-aware Dice loss significantly boosts segmentation sensitivity for small nodal metastases in head and neck cancer.
It compares dual mask and selective LN mask strategies, highlighting trade-offs between increased lymph node sensitivity and primary tumor precision.
Results indicate that the dual mask approach offers a balanced improvement in segmentation performance for adaptive MR-guided radiotherapy workflows.
Volume-Aware Dice Loss for Improved Auto-Delineation in MR-Guided Radiotherapy for Head and Neck Cancer
Introduction
Manual delineation of tumor and nodal targets in head and neck cancer (HNC) radiotherapy is labor-intensive and plagued by inter-observer variability, a bottleneck for adaptive MR-guided radiotherapy (ART). Deep learning-based auto-segmentation frameworks, specifically nnU-Net, have been widely adopted to automate this task. However, they frequently underperform on small but clinically critical nodal metastases due to the class imbalance in structure volume, with large primary tumors dominating the optimization of standard loss functions. This paper investigates a Volume-Aware (VA) Dice loss, which dynamically upweights small structure voxels, within a state-of-the-art nnU-Net ResEnc M pipeline to enhance segmentation accuracy for both primary tumors (PT) and metastatic lymph nodes (LN) (2604.10130). The study rigorously evaluates standard and two volume-aware multi-label segmentation strategies: (1) Dual Mask—applying VA loss to both PT and LN, and (2) Selective LN Mask—applying VA loss only to the LN.
Methodology
Data and Pre-processing
The study leverages the HNTS-MRG 2024 challenge dataset, comprising expertly annotated and consensus-reviewed T2-weighted MR images of oropharyngeal and hypopharyngeal HNC. The nnU-Net ResEnc M architecture is employed for multi-label segmentation, integrating automated preprocessing and augmentation tailored to the input data characteristics.
Volume-Aware Dice Loss Formulation
Traditional Dice loss is suboptimal for multi-structure problems with extreme size disparity. The VA Dice loss introduces voxel-wise weighting: each voxel’s contribution to the loss is scaled inversely with the square root of the lesion's volume. For a connected component of volume Vj, the weighting factor is wi=1/Vj, making small structure misclassifications exert a greater influence during training.
The study contrasts three configurations:
Baseline: Standard nnU-Net using combined Dice and Cross-Entropy loss.
Dual Mask VA: VA Dice loss applied to both PT and LN.
Selective LN Mask VA: VA Dice loss only for the LN channel, with standard Dice for PT.
Evaluation spans volumetric Dice, surface Dice (1mm tolerance), mean surface distance (MSD), 95th percentile Hausdorff distance (HD95), and lesion-wise binary sensitivity and precision.
Results
Enhanced Segmentation Performance for Small Lesions
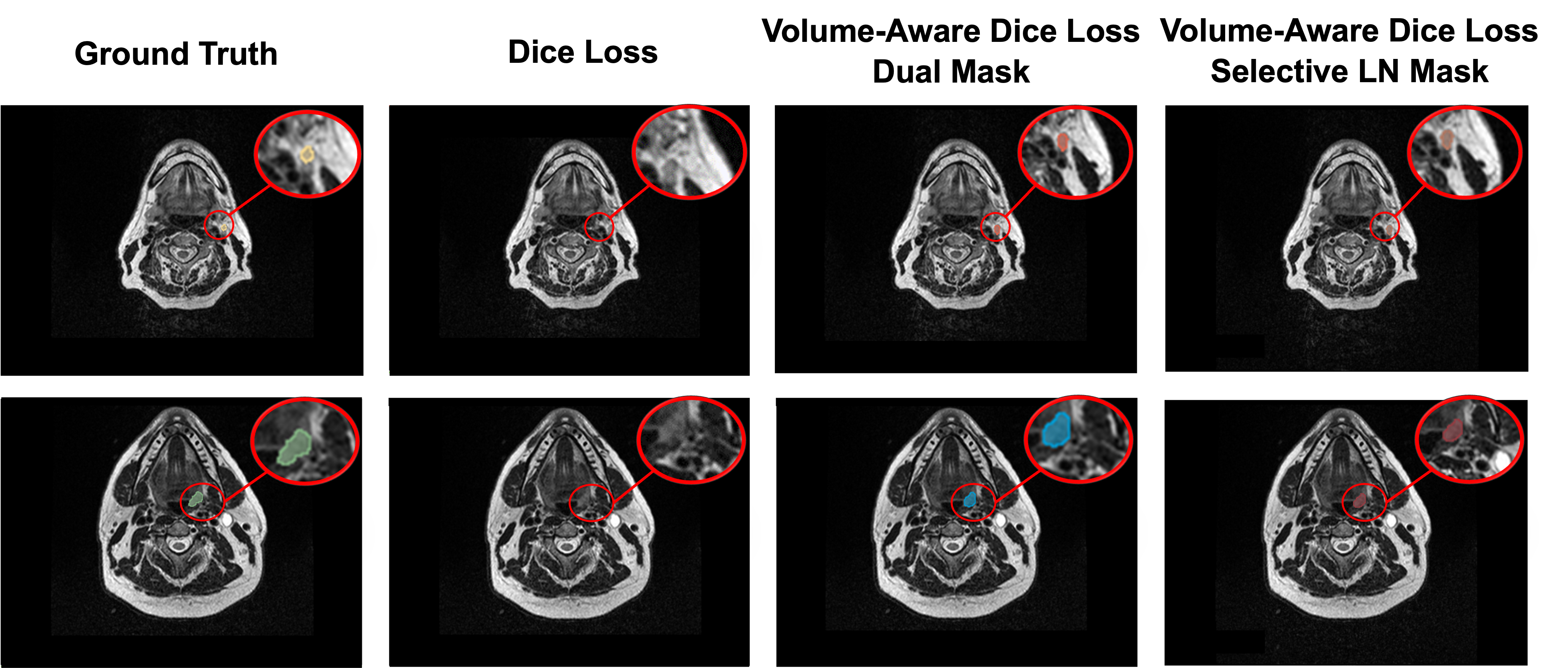
The incorporation of VA Dice loss consistently yields superior segmentation on small nodal targets compared to the baseline. Notably, the Selective LN Mask configuration achieves the highest LN Dice score (0.758 vs. 0.734 baseline) and LN lesion-wise sensitivity (84.93% vs. 81.80% baseline), at a cost of significantly reduced PT detection precision (63.65% vs. 81.27%). The Dual Mask VA offers balanced improvements, maintaining PT precision and augmenting LN sensitivity (83.46% vs. 81.80%) without sacrificing PT performance.
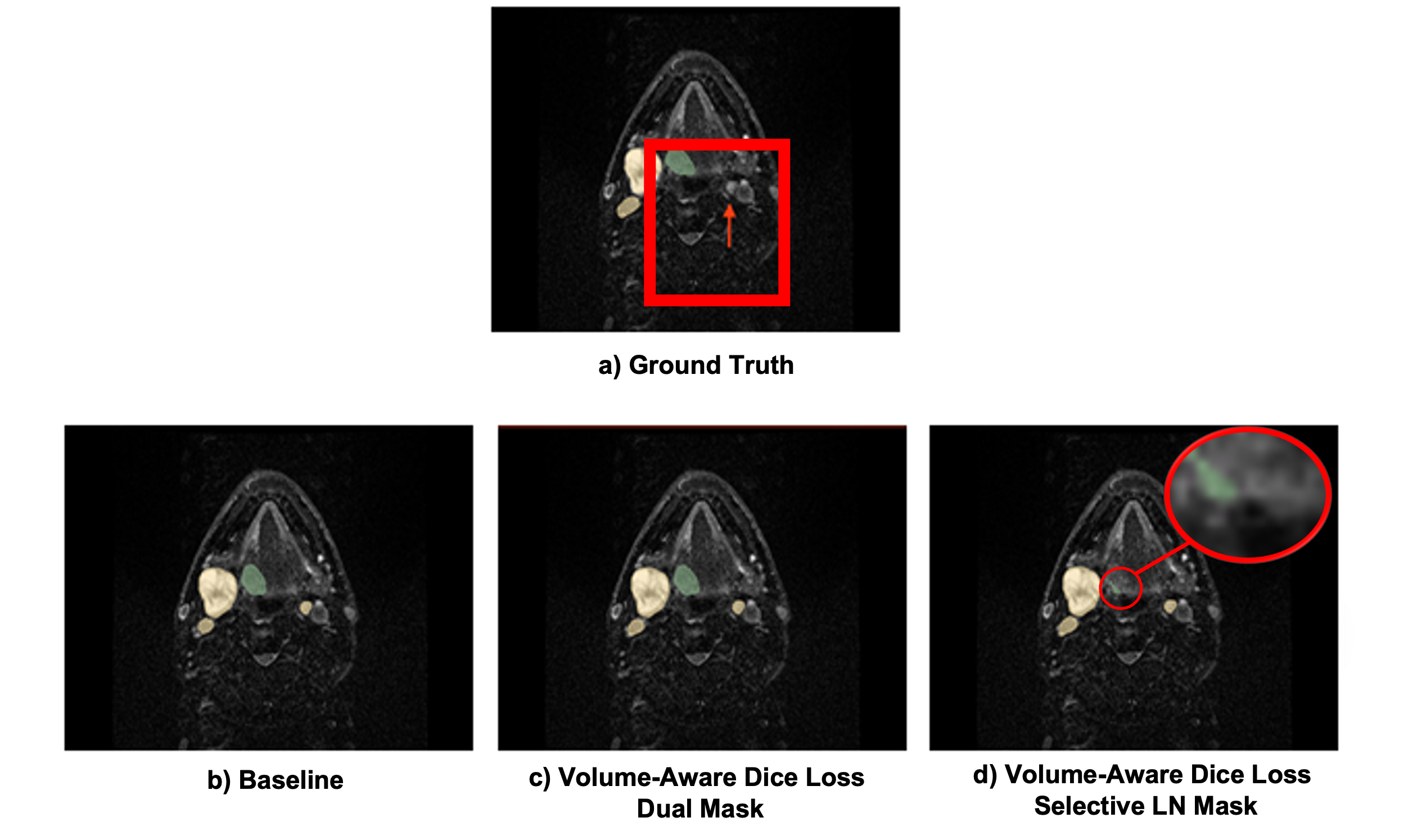
Figure 1: Examples of superior segmentation using VA Dice loss versus the baseline method.
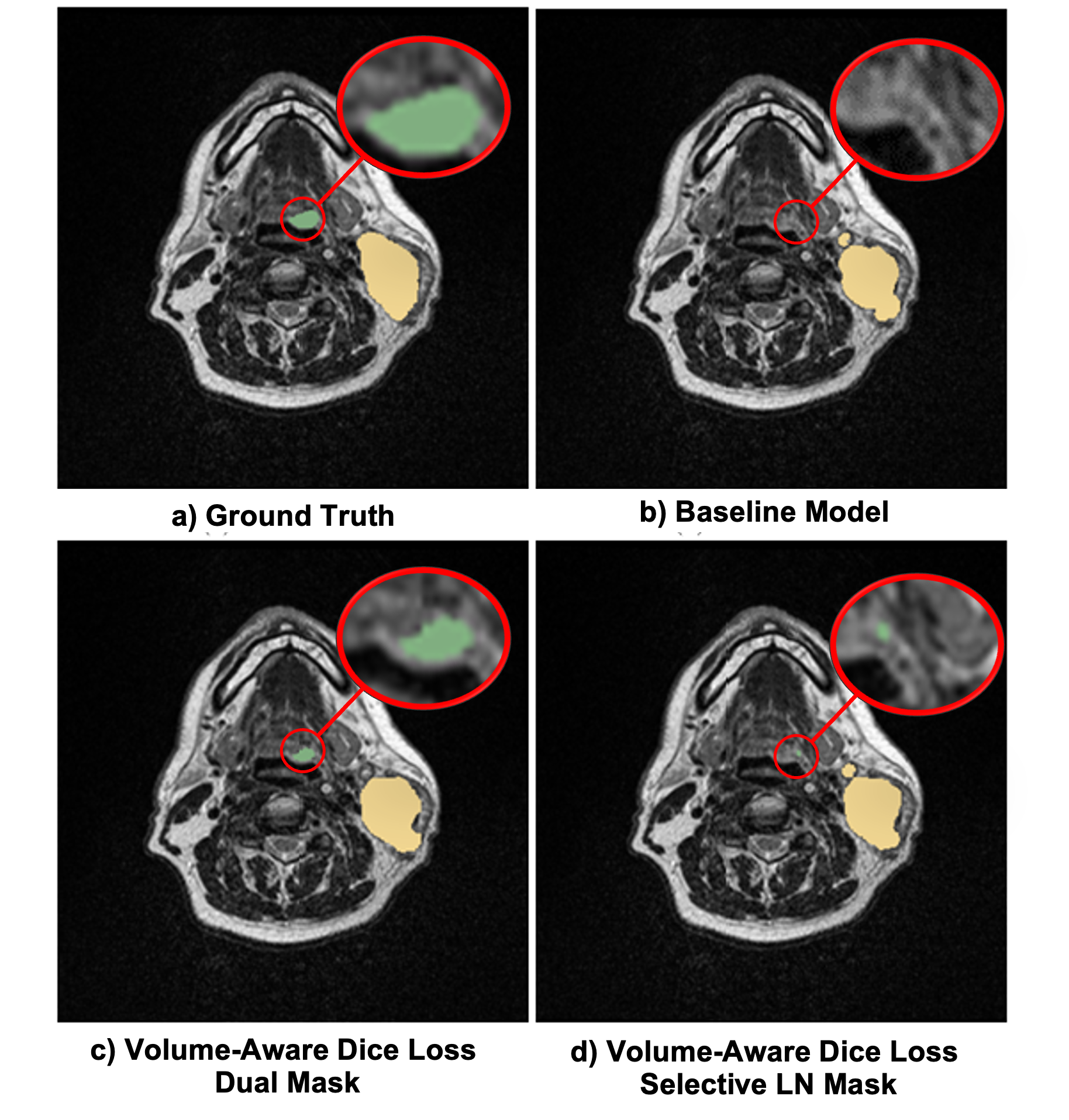
Figure 2: Effects of different VA Dice loss strategies on multi-label segmentation masks, highlighting PT (green) and LN (yellow).
Volumetric and Surface Metric Analysis
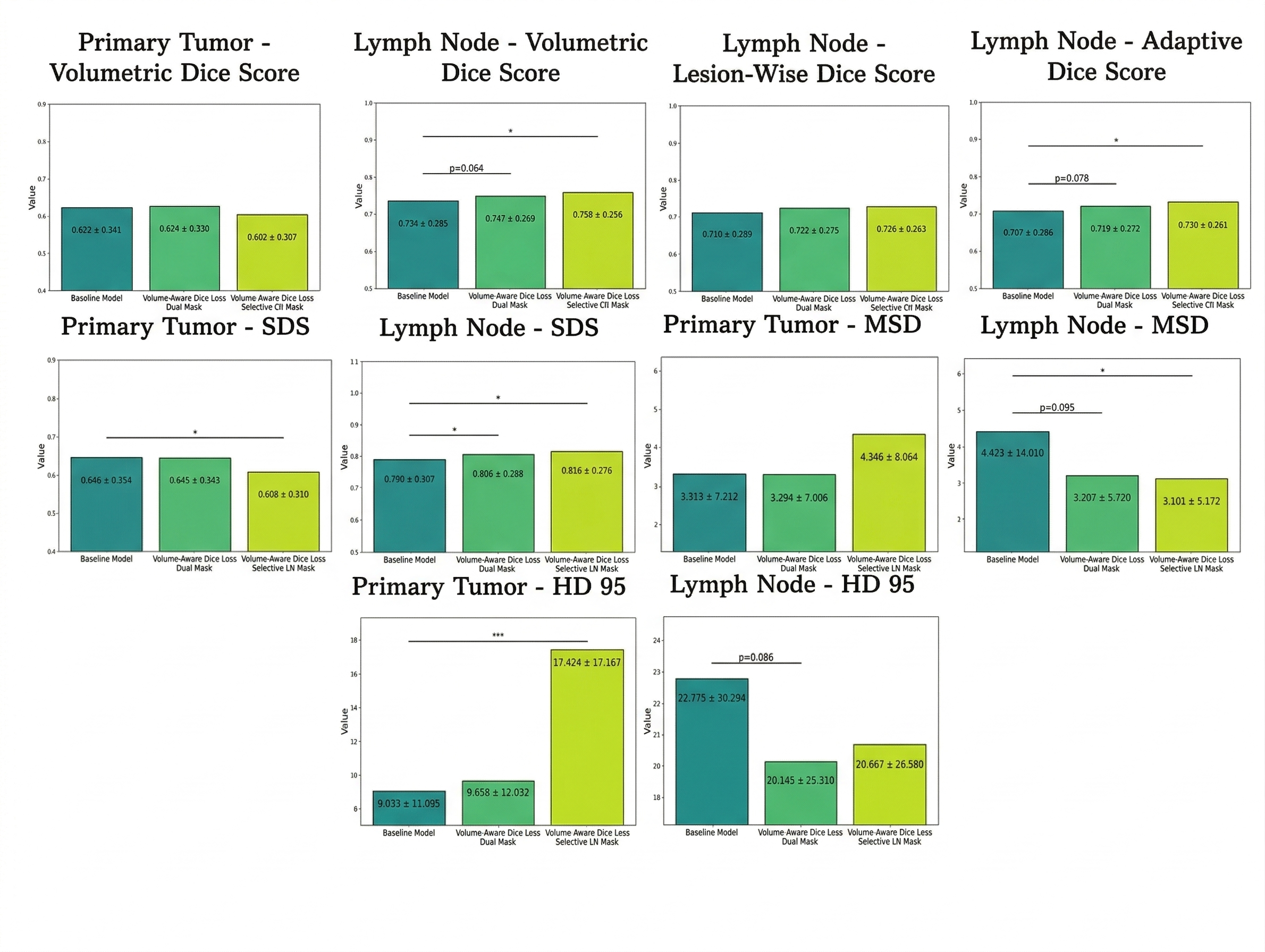
Volumetric Dice and surface-based metrics further underscore VA Dice loss efficacy. The Selective LN Mask setup provides statistically significant enhancements in LN Dice, Adaptive Dice, surface Dice, and MSD metrics. Improvement in boundary alignment, especially for LNs, highlights the VA loss’s ability to enhance geometric fidelity for small targets.
Figure 3: Volumetric and surface similarity metrics for PT and LN across evaluated configurations.
Detection Sensitivity and Precision Trade-offs
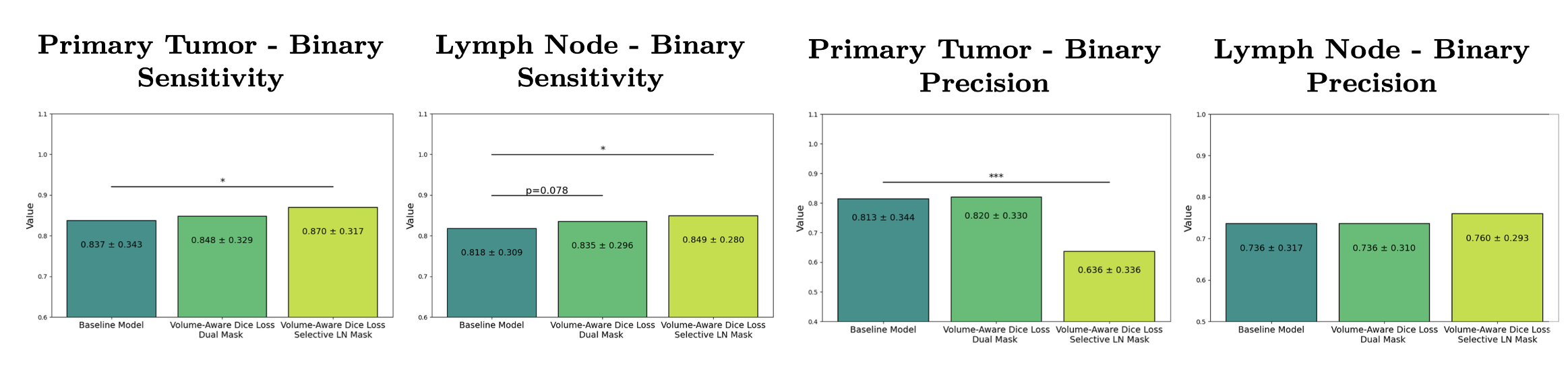
A marked trade-off emerges between structure sensitivity and precision with selective application of VA Dice loss. While LN sensitivity is maximized in the Selective LN Mask configuration, PT precision deteriorates—emphasizing a competitive relationship in network optimization between large and small targets. The Dual Mask VA mitigates this by providing a balanced compromise, avoiding a sharp decline in PT performance.
Figure 4: Binary detection sensitivity and precision metrics for PT and LN across all segmentation strategies.
Figure 5: Segmentation visualizations for an example patient, comparing all model configurations and highlighting the superior overall performance of the Dual Mask VA Dice approach.
Discussion
The results decisively demonstrate that class-agnostic loss functions confer a bias favoring large structures, inadequately penalizing missed small targets and yielding clinical risk for nodal under-coverage. The volume-aware approach, especially the class-specific application to LNs, directly addresses this bias. However, the inherent gradient competition in multi-label segmentation mandates judicious loss weighting; optimizing for small lesions can induce model over-sensitivity and increased false positives for the larger PT. The Dual Mask VA Dice strikes the optimal balance in many clinical contexts, safeguarding both LN detection sensitivity and PT geometric precision.
The dual-label segmentation paradigm closely mirrors clinical workflow, where PT and LN delineation are not independent, but rather spatially and pathophysiologically coupled. Leveraging shared anatomical and imaging signals in simultaneous optimization appears beneficial for overall target delineation robustness.
Conclusion
Application of a Volume-Aware Dice loss within a self-adapting nnU-Net framework enhances the detection and segmentation of small, clinically important lymph node metastases in HNC, addressing significant limitations of traditional losses in high-class-imbalance regimes. While selective upweighting maximizes nodal detection, a dual-mask application in multi-label tasks is necessary to prevent a detrimental trade-off in primary tumor precision. This work supports adoption of volume-normalized objective functions for MR-guided adaptive radiotherapy workflows, with the potential to increase automation, reduce expert workload, and improve treatment accuracy. Future research may focus on adaptive or dynamic weighting strategies and integration with uncertainty quantification to further stabilize the precision-sensitivity balance in clinical deployment.