- The paper introduces a novel training-free framework that quantifies phonological degradation in self-supervised speech models to assess dysarthria severity.
- It leverages healthy control data to compute d' metrics across phonological subspaces, achieving robust cross-lingual performance with ROC AUC up to 0.89.
- The approach provides interpretable and clinically relevant profiles that support screening, differential diagnosis, and scalable multilingual assessment.
Training-Free Cross-Lingual Dysarthria Severity Assessment via Phonological Subspace Analysis in Self-Supervised Speech Representations
Introduction and Motivation
Dysarthria presents a significant challenge for automated speech assessment due to limited labeled data, especially in non-English contexts and rare aetiologies. Most existing systems require supervised learning with pathological speech samples, constraining cross-lingual scalability and interpretability. The paper "Training-Free Cross-Lingual Dysarthria Severity Assessment via Phonological Subspace Analysis in Self-Supervised Speech Representations" (2604.10123) addresses these limitations by proposing a training-free, cross-lingual dysarthria severity assessment framework, leveraging the representational structure of self-supervised speech models (specifically HuBERT) and quantifying the degradation of phonological feature subspaces as a proxy for articulatory precision.
Methodological Framework
The pipeline consists of five stages: phone-level alignment (via Montreal Forced Aligner, MFA), extraction of HuBERT embeddings, computation of phonological feature directions using only healthy control speech, calculation of per-speaker d′ metrics along these directions, and generation of a 12-dimensional phonological profile per speaker. Notably, the entire method requires no access to dysarthric speech during feature direction estimation and no supervised model training.
The core metric, d′, quantifies the discriminability between phone classes along articulatory-relevant axes (e.g., nasality, voicing, manner), utilizing L2-normalized class mean differences in the high-dimensional HuBERT space. Feature directions are computed per language using matched healthy controls, allowing cross-lingual extension wherever MFA models exist.
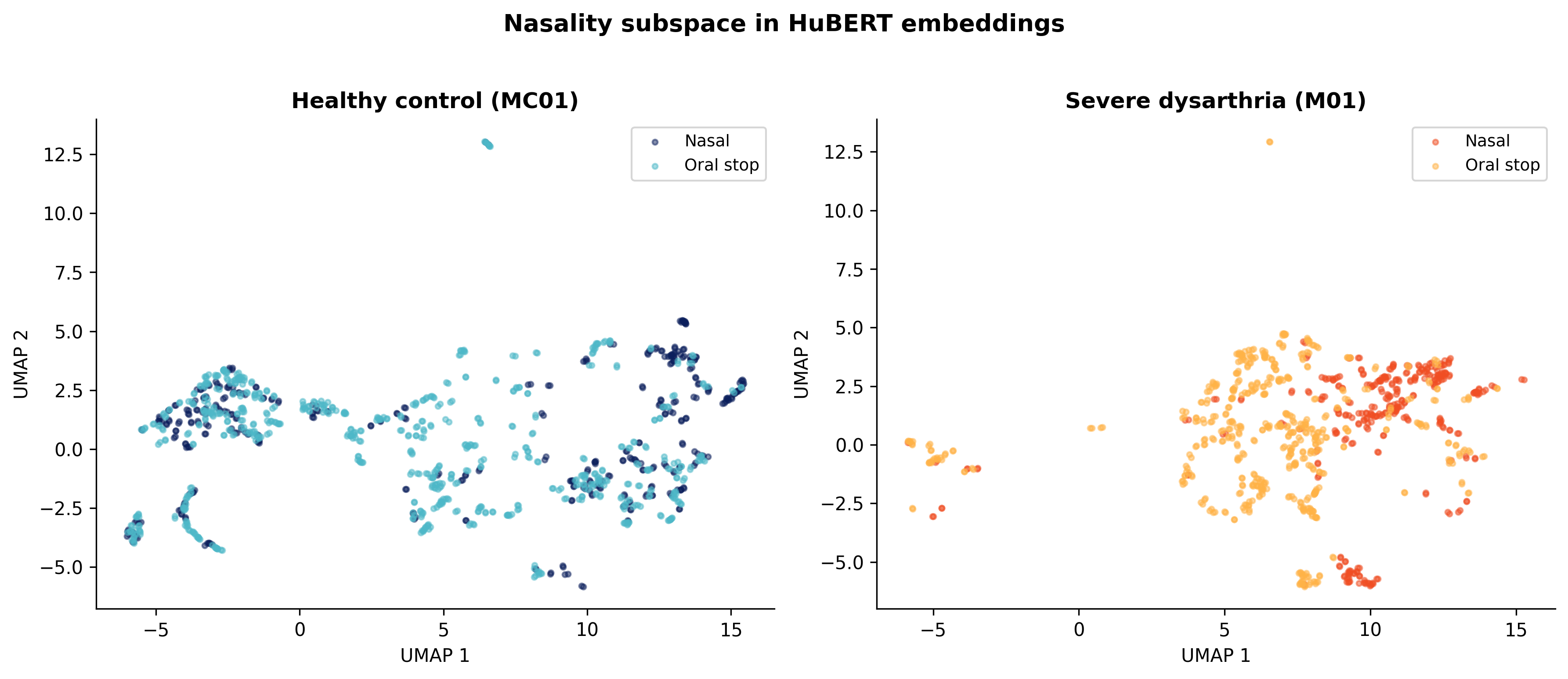
Figure 1: UMAP projections show clear clustering of nasal and oral stops in healthy speech, with substantial collapse and increased overlap in severe dysarthria; d′ quantifies this separation in full embedding space.
Evaluation Protocol and Data
The framework was rigorously validated on 890 speakers spanning 10 corpora, 5 languages (English, Spanish, Dutch, Mandarin, French), and three aetiologies (Parkinson's disease, cerebral palsy, amyotrophic lateral sclerosis). Data included both connected and read speech. Severity labels were harmonized across datasets using established intelligibility-based thresholds [Stipancic et al.].
Statistical analyses comprised pooled and within-corpus Spearman correlations, bootstrap confidence intervals, Benjamini-Hochberg FDR corrections, partial correlations to address confounds (notably, token-count bias), random-effects meta-analysis, and ROC thresholding for clinical screening evaluation.
Main Results and Empirical Validation
Across all analyses, consonant d′ features emerged as robust markers of dysarthria severity. Pooled Spearman correlations for these metrics ranged between −0.47 and −0.55 (bootstrap 95% CIs not crossing zero), with the strongest single metric being nasality d′ (ρ=−0.547) and stridency d′ excelling at severity discrimination (ROC AUC = 0.89).
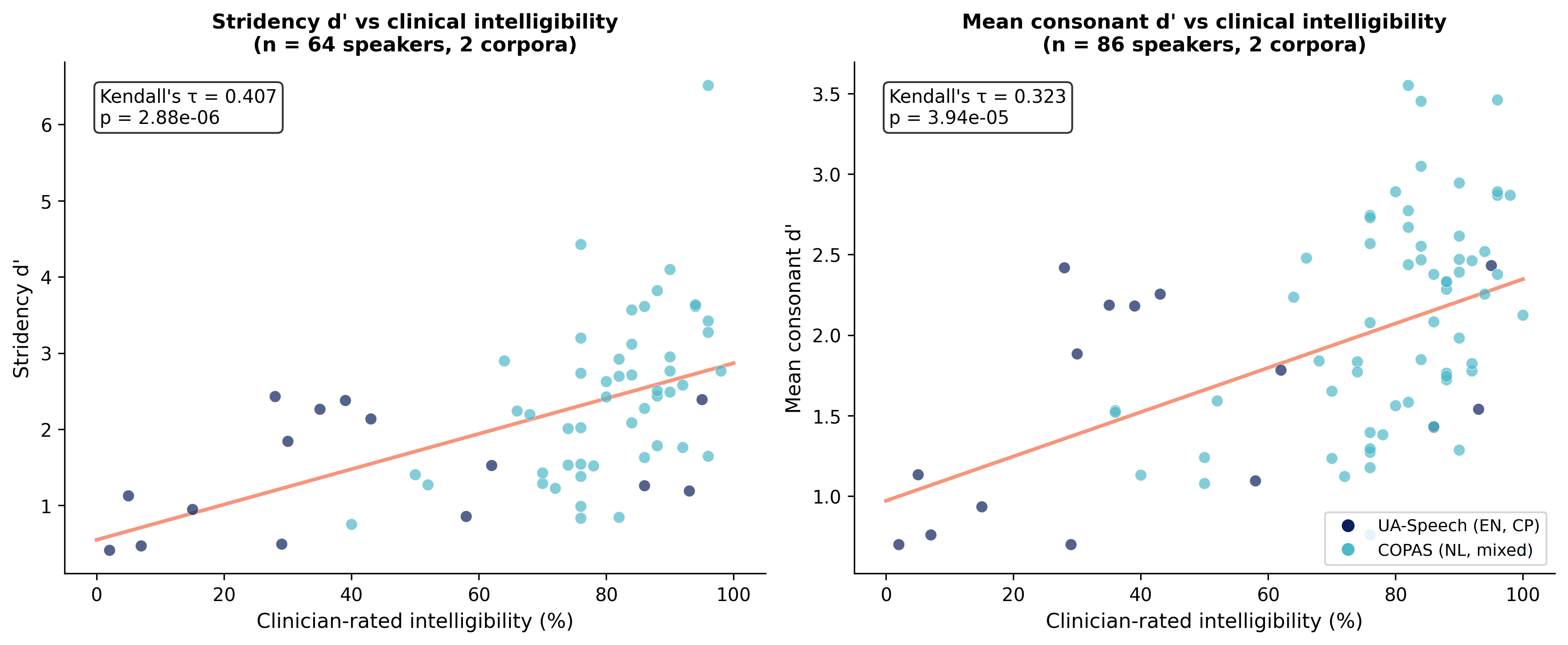
Figure 2: d′ metrics strongly correlate with clinician-rated intelligibility across languages, substantiating clinical validity.
Importantly, the severity-degradation relationship holds within each corpus, independent of language or recording protocol. Strongest within-corpus effects were observed in datasets with clean recording conditions and wide severity spectra (e.g., MDSC, UA-Speech).
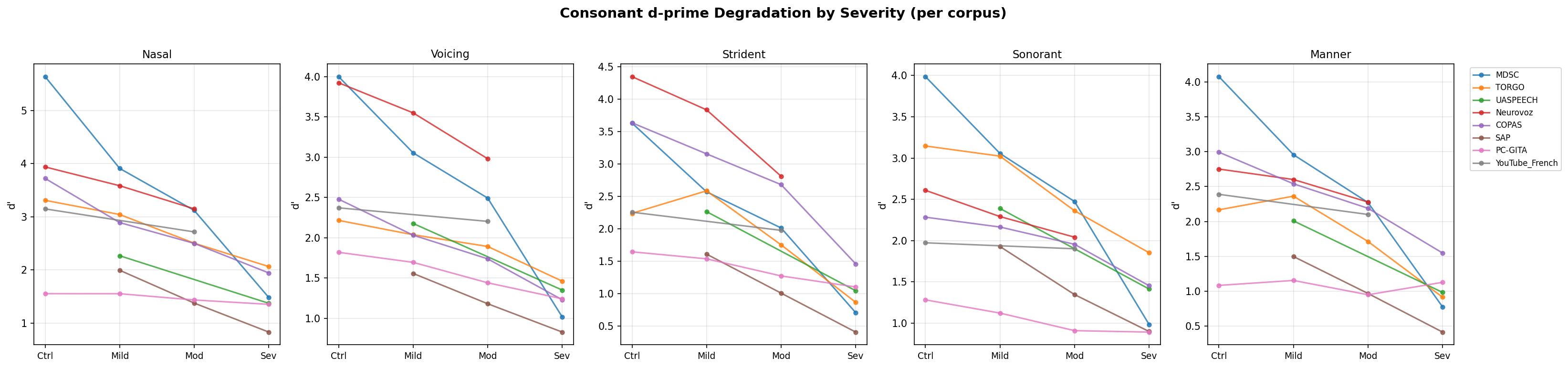
Figure 4: Consonant d′0 features demonstrate consistent, monotonic declines from healthy control to severe dysarthria across all corpora and languages.
Random-effects meta-analysis confirmed that all five consonant d′1 features remain significant (d′2), with high between-corpus heterogeneity but consistent negative effect direction (d′3 to d′4). Leave-one-corpus-out, bootstrapping, and alternate-architecture replications (WavLM, wav2vec2) further reinforced robustness.
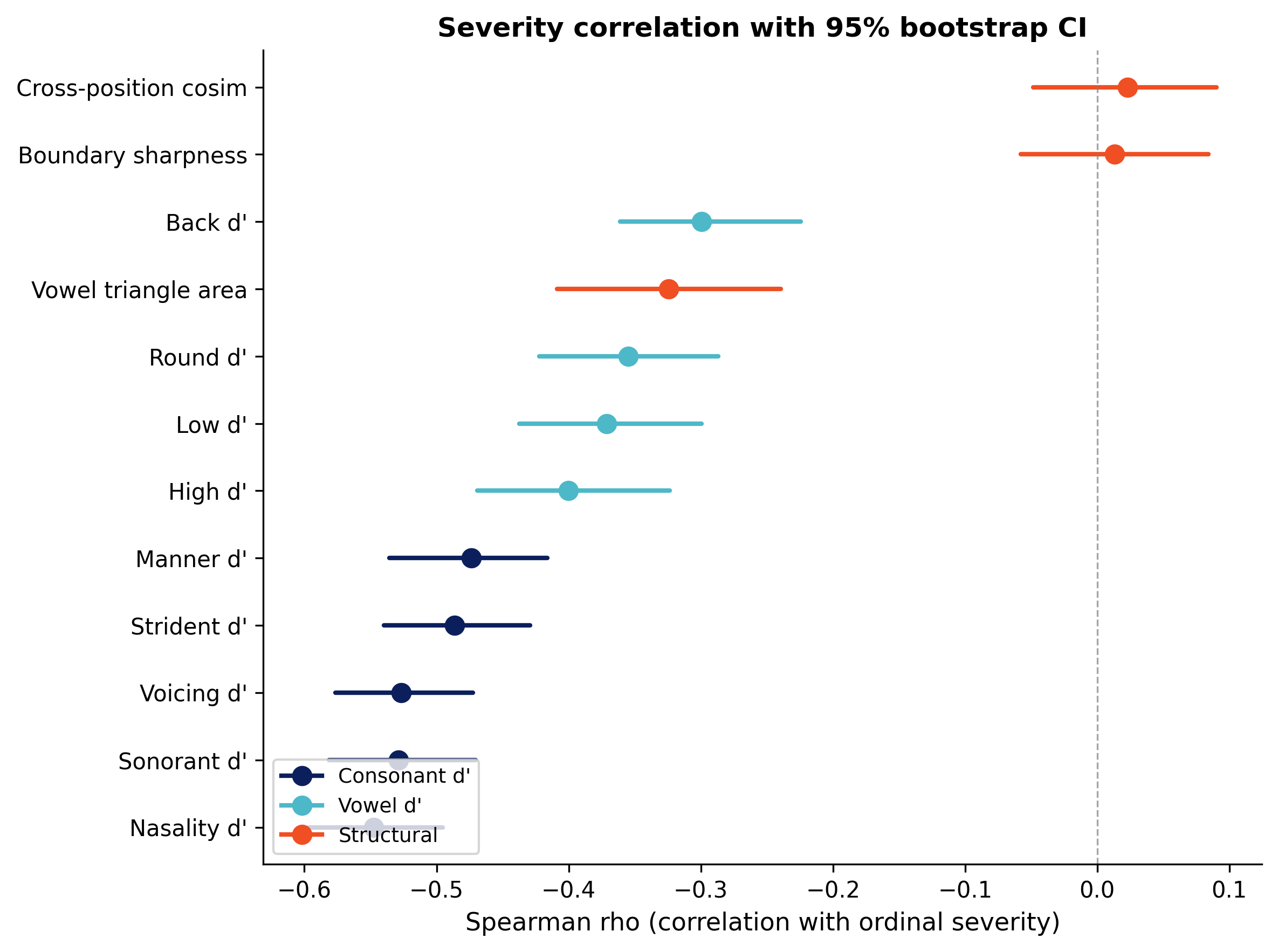
Figure 3: Bootstrap confidence intervals and forest plots for phonological features, sorted by effect size, all d′5 features maintain significant negative correlation with severity.
Phonological profile vectors enabled interpretable distinction between aetiologies, revealing, for example, uniform degradation in CP and relatively preserved voicing in ALS/PD. Discriminability for clinical screening is strong: stridency d′6 achieves 85% sensitivity and 82% specificity for severe dysarthria in cross-corpus ROC analysis.
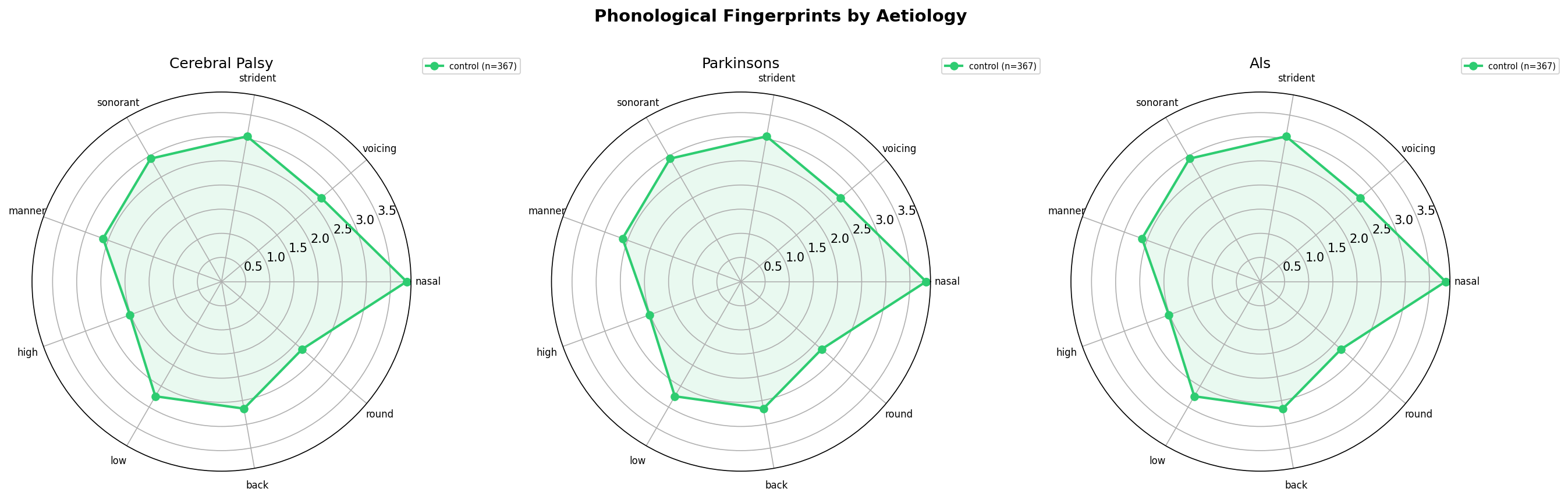
Figure 5: Radar plots show distinct aetiology-specific phonological fingerprints, allowing fine-grained subtypification.
Analysis of Limitations
Token Count Confound: d′7 increases with the number of observed phone tokens even in healthy controls, driven by reduced estimation variance. This artifact restricts cross-corpus comparison of absolute d′8 values but does not affect within-protocol severity ranking, as confirmed by partial correlation and token-count stratification. Fixed-token subsampling strengthens correlations, supporting robustness.
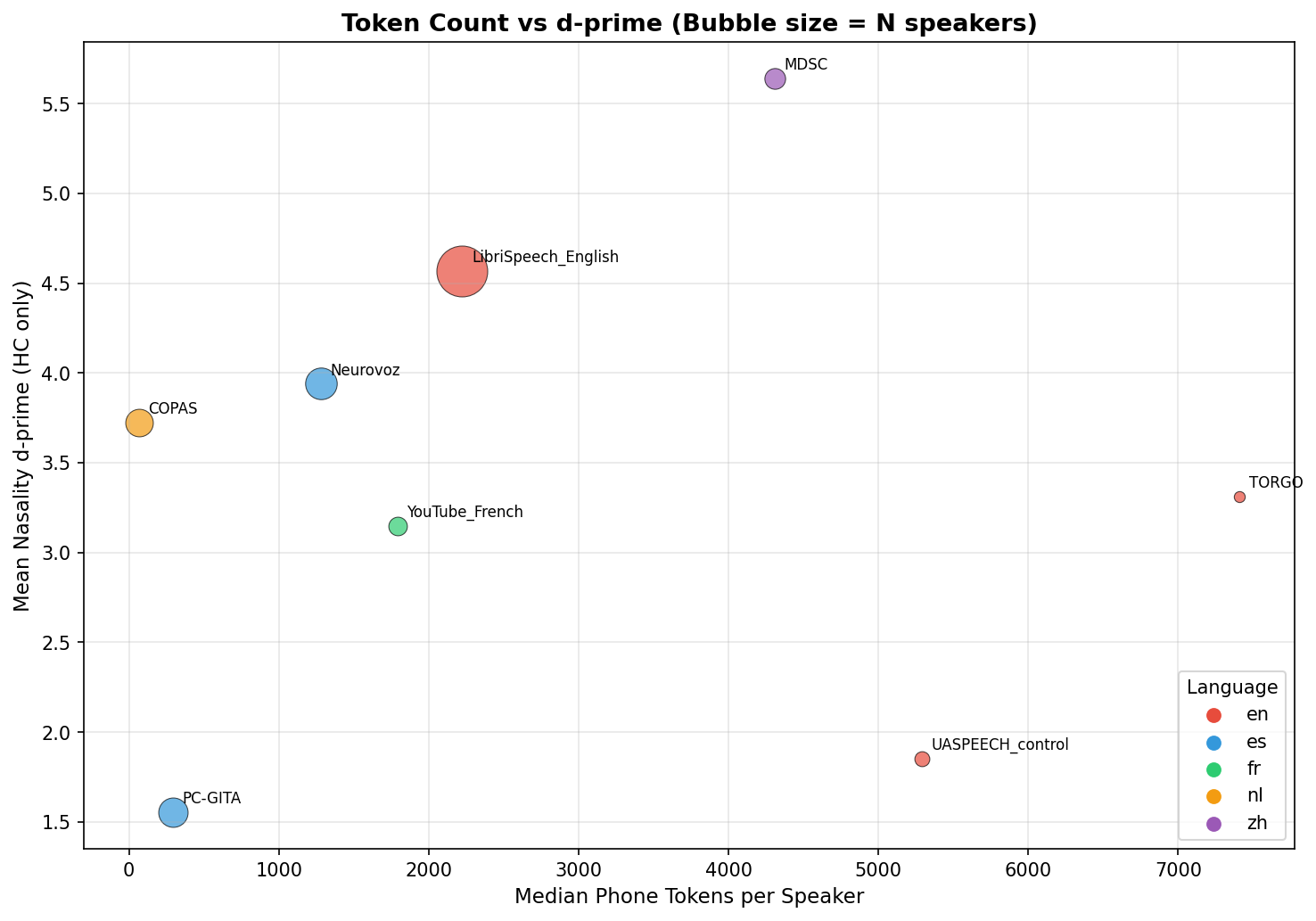
Figure 8: Positive relationship between phone token count and d′9 in healthy controls exposes the necessity for within-protocol or token-normalized comparisons.
Alignment Quality: MFA quality degrades with severe dysarthria; however, restricting to high-quality alignments and partialling alignment metrics produces only minimal changes in core findings.
Speech Type Effects: Structural metrics such as boundary sharpness reflect both articulatory degradation and compensatory hyperarticulation in read speech; these features must be interpreted with task stratification.
Cross-Lingual Calibration: Absolute d′0 thresholds are not directly portable between languages or corpora due to varying phone inventories, recording protocols, and healthy reference distributions. Within-language and within-site ranking is reliable provided matched healthy controls are used for feature direction computation.
Theoretical and Practical Implications
The proposed framework demonstrates that self-supervised models encode articulatory-phonological structure rich enough to support objective, interpretable, and cross-lingual severity assessment without supervised adaptation. This advances clinical utility in several respects:
- Scalability: Deployment is feasible in any language with MFA coverage, requiring only healthy control data and no pathological training data.
- Interpretability: Subsystem-level degradation vectors align with clinical intuition and guide differential diagnosis and therapy planning.
- Robustness: Results generalize across architectures, languages, and both connected/read speech, subject to adequate token count and matched healthy controls.
- Screening Utility: d′1 features, especially stridency and nasality, operate as effective clinical screening tools; ROC analysis suggests practical operational cutoffs for automated triage.
- Integration Potential: The phonological profile provides a low-dimensional, interpretable feature-set suitable for downstream supervised systems, combining interpretability and prediction accuracy.
The findings also empirically validate the linearly decodable subspace structure of self-supervised speech models identified in prior work (e.g., Choi et al. (Choi et al., 13 Mar 2026)), revealing its degradation as a biomarker for motor speech impairment.
Open Directions and Future Work
Key domains for extension include:
- Longitudinal Tracking: Validation of d′2 change trajectories as early, sensitive progression markers in longitudinal dysarthria cohorts, particularly ALS.
- Multilingual and Multimodal Expansion: Application to additional languages, multilingual SSL pretraining, and incorporation of suprasegmental/prosodic subspaces.
- Protocol Harmonization: Developing normalization or domain adaptation methods for absolute severity scoring across sites and conditions.
- Integration with Supervised Learning: Using interpretable profiles as diagnostic features in multi-modal clinical decision support systems.
Conclusion
The paper establishes that phonological subspace degradation in HuBERT and other self-supervised models yields a reliable, interpretable, and training-free marker of dysarthria severity. Across a comprehensive multi-corpus, multi-lingual evaluation, all consonant d′3 features exhibited statistically robust negative correlations with clinical severity, replicating across corpora, aetiologies, and SSL architectures. Absolute d′4 values require protocol calibration, but within-protocol ranking is robust. The work lays the groundwork for practical, scalable, and interpretable speech monitoring tools for neurological disorders, with a clear path towards cross-lingual clinical deployment and further research integrating segmental and suprasegmental analyses.
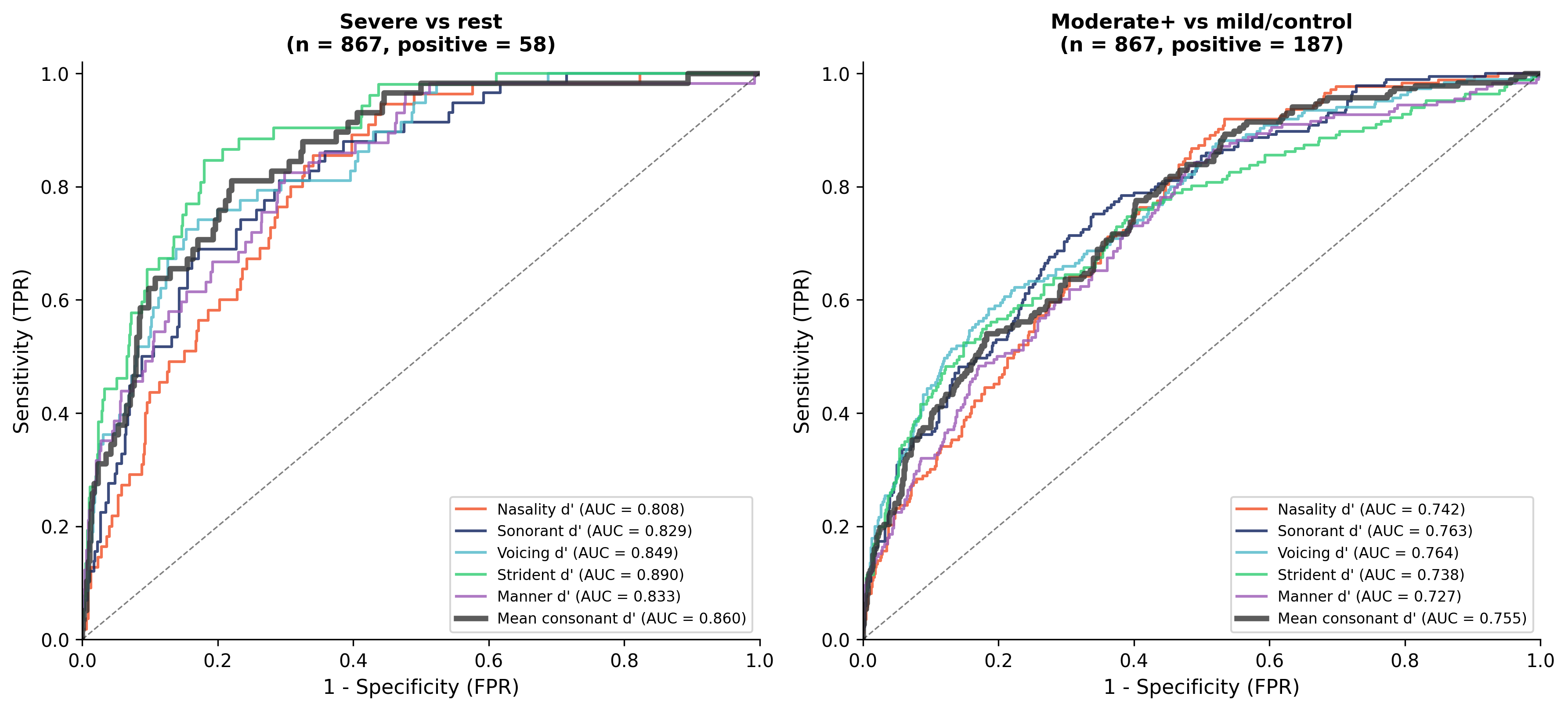
Figure 6: ROC curves demonstrate excellent screening performance for severe and moderate-or-worse dysarthria using stridency and mean consonant d′5.

