- The paper demonstrates that wireless ECG devices, with proper filtering and normalization, yield RR interval and HRV metrics comparable to clinical systems.
- It employs rigorous statistical tests and controlled preprocessing, ensuring device-induced biases are minimized during various physical activities.
- Results support the use of wireless ECGs in remote monitoring by reliably capturing activity-induced changes in autonomic balance.
Statistical Reliability of Wireless ECG Data Collected in Non-Clinical Environments
Introduction
The proliferation of wireless electrocardiogram (ECG) systems has generated immense interest for their potential application in continuous cardiac monitoring outside clinical settings. However, the reliability and statistical equivalence of data acquired in uncontrolled environments—often with layperson placement and operation—must be thoroughly validated before such devices are entrusted with diagnostic or prognostic tasks. This paper ("Statistical Analysis of the Reliability of Data Collected with Wireless Electrocardiograms Outside Clinical Settings" (2604.06992)) addresses this research gap by conducting a rigorous comparative statistical analysis of RR interval and heart rate variability (HRV) features across three heterogeneous datasets: wirelessly collected ECG from 54 healthy subjects performing multiple activities, clinically acquired 12-lead ECG from the PTB-XL database (2,493 subjects), and ambulatory Holter ECGs (29 subjects).
Dataset Construction and Preprocessing
The proprietary dataset utilizes the Shimmer3 wireless ECG platform, deployed unsupervised by healthy participants in protocol-driven activity sessions (sitting, standing, stair climbing, walking). The clinical reference datasets include PTB-XL’s normal ECGs and Holter-based RR interval time-series. All ECG signals underwent bandpass filtering (0.5–40 Hz) and notch filtering to suppress baseline and power-line interference, followed by Min-Max normalization. R-peak detection used NeuroKit2's algorithm, ensuring methodological consistency across datasets. This preprocessing pipeline mitigates device-specific artifacts and facilitates feature comparability.
Statistical Comparison of ECG Features
The statistical distributions of RR intervals and heart rate (HR) were central to the reliability assessment. Empirical histograms for Shimmer3, 12-lead, and Holter ECG datasets demonstrated substantial overlap in RR interval (mean differences ≤ 0.07 s; SD differences ≤ 0.01 s) and HR features (mean differences ≤ 8.54 bpm; SD differences ≤ 2.46 bpm). These findings indicate minimal device-induced bias after calibration.

Figure 1: RR interval and HR histograms for Shimmer3 and 12-lead illustrate strong agreement in both mean and variance.
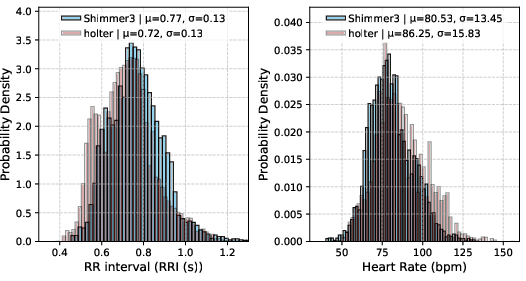
Figure 2: RR interval and HR comparison between Shimmer3 and Holter ECG signals, reinforcing cross-device reliability.
The statistical equivalence was further quantified by p-values derived from four distinct confidence interval estimation protocols: (1) known clinical variance, unknown mean; (2) unknown variance and mean; (3) known clinical mean, unknown variance; (4) non-referenced estimation. Across RR interval and HRV, p-values (RR: 0.23–0.26, HRV: 0.10–0.11) consistently exceeded standard significance thresholds, substantiating the null hypothesis of statistical agreement. These results support the claim that wireless ECG features can serve as reliable surrogates for clinical-grade metrics given proper preprocessing.
Activity-Induced Cardiac Feature Variability
Heart rate variability (HRV) was analyzed in the context of physical activity, leveraging time-domain, nonlinear, and frequency-domain measures. RR interval and HR varied predictably with activity intensity: sitting yielded longer RR intervals and higher variability, whereas stair ascent caused marked reductions in HRV, indicative of sympathetic dominance.
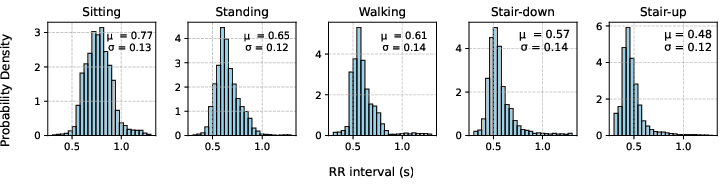
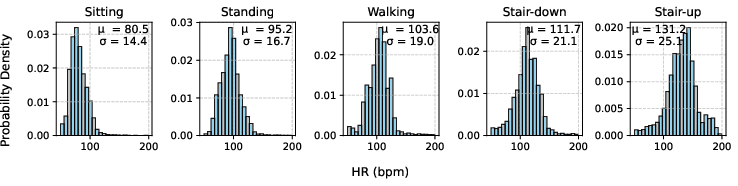
Figure 3: RR-interval and HRV statistics stratified by activity, showing a decrease in RR-interval and HRV with increasing exertion.
Nonlinear analysis using Poincaré plots revealed activity-dependent modulation in sympathovagal balance. During rest, the plots exhibited broader ellipses (SD1/SD2 ratio: 0.41), signifying high parasympathetic activity. As exertion intensified, the ellipses narrowed (ratio as low as 0.16 during stair climbing), signifying enhanced sympathetic influence.
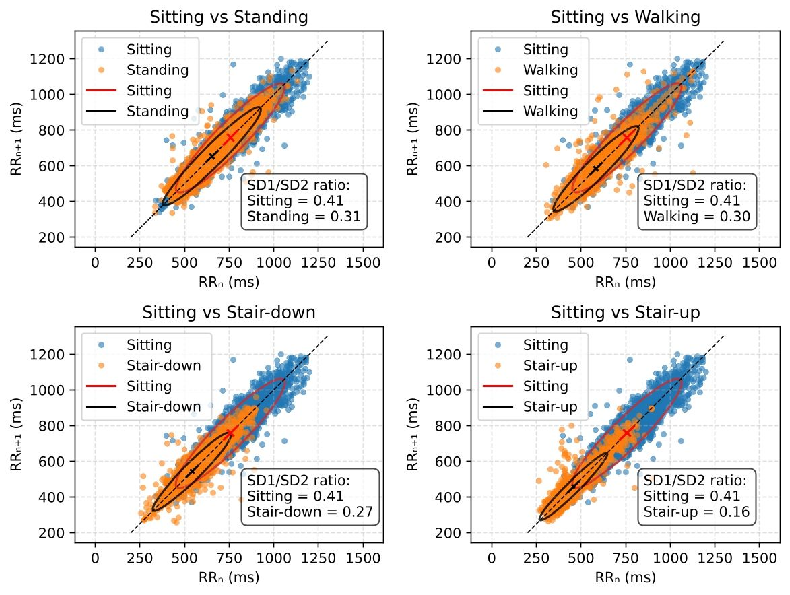
Figure 4: Poincaré plots quantify the reduction of parasympathetic response with increasing physical activity.
Boxplot visualization of HRV metrics (SDNN, RMSSD, SD1, SD2) further confirmed robust reductions in both short- and long-term variability parameters under increased physical stress, with walking producing the greatest inter-individual variance.
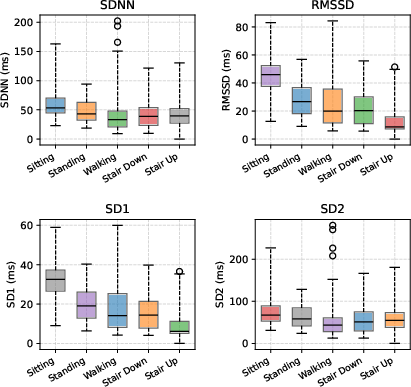
Figure 5: Boxplot demonstrates reduced HRV metric medians during high-exertion activities, signaling autonomic adaptation.
Frequency-domain analysis focused on LF (sympathetic) and HF (parasympathetic) power, utilizing Lomb–Scargle periodograms. Physical exertion was correlated with increased normalized LF and diminished HF spectral power, consistent with established models of autonomic modulation.
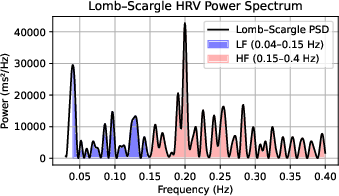
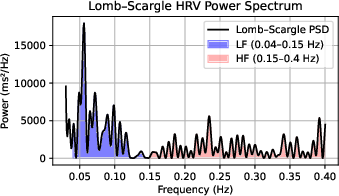
Figure 6: LF and HF spectral power comparison for sitting versus climbing, confirming a shift toward sympathetic activity during exertion.
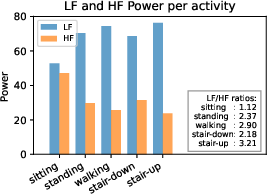
Figure 7: Aggregated LF and HF power across all activities, highlighting progressive sympathetic dominance.
Practical and Theoretical Implications
These results have direct implications for remote cardiac monitoring, sport physiology, and outpatient diagnostics. The strong agreement in RR interval and HRV statistics across wireless and clinical ECG systems, even during variable physical activities and unsupervised operation, supports the adoption of wireless ECGs for ambulatory health evaluation, risk stratification, and early detection paradigms. The robustness to device and environmental noise, as evidenced by the confidence interval analyses, validates their application in ML-based disease prediction pipelines reliant on high-quality feature extraction.
The findings provide further theoretical insight into sympathovagal balance as assessed through HRV metrics and spectral features in unconstrained monitoring scenarios. The ability to capture activity-driven dynamic transitions in autonomic function outside the clinic paves the way for studies of stress adaptation, wellness, and personalized medicine. Future research may focus on separating device-originated error sources, expanding age and health status coverage, and exploring multimodal sensor fusion.
Conclusion
Wireless ECG platforms, when coupled with standardized filtering, normalization, and R-peak detection algorithms, deliver RR interval and HRV features statistically equivalent to clinical-grade reference systems. Activity-driven modulation of cardiac features, including the sympathovagal balance, is reliably captured, supporting the case for their integration into scalable, remote health monitoring frameworks. Further advancements may arise from expanded datasets, rigorous calibration protocols, and granular error source analysis.