MedGemma 1.5 Technical Report
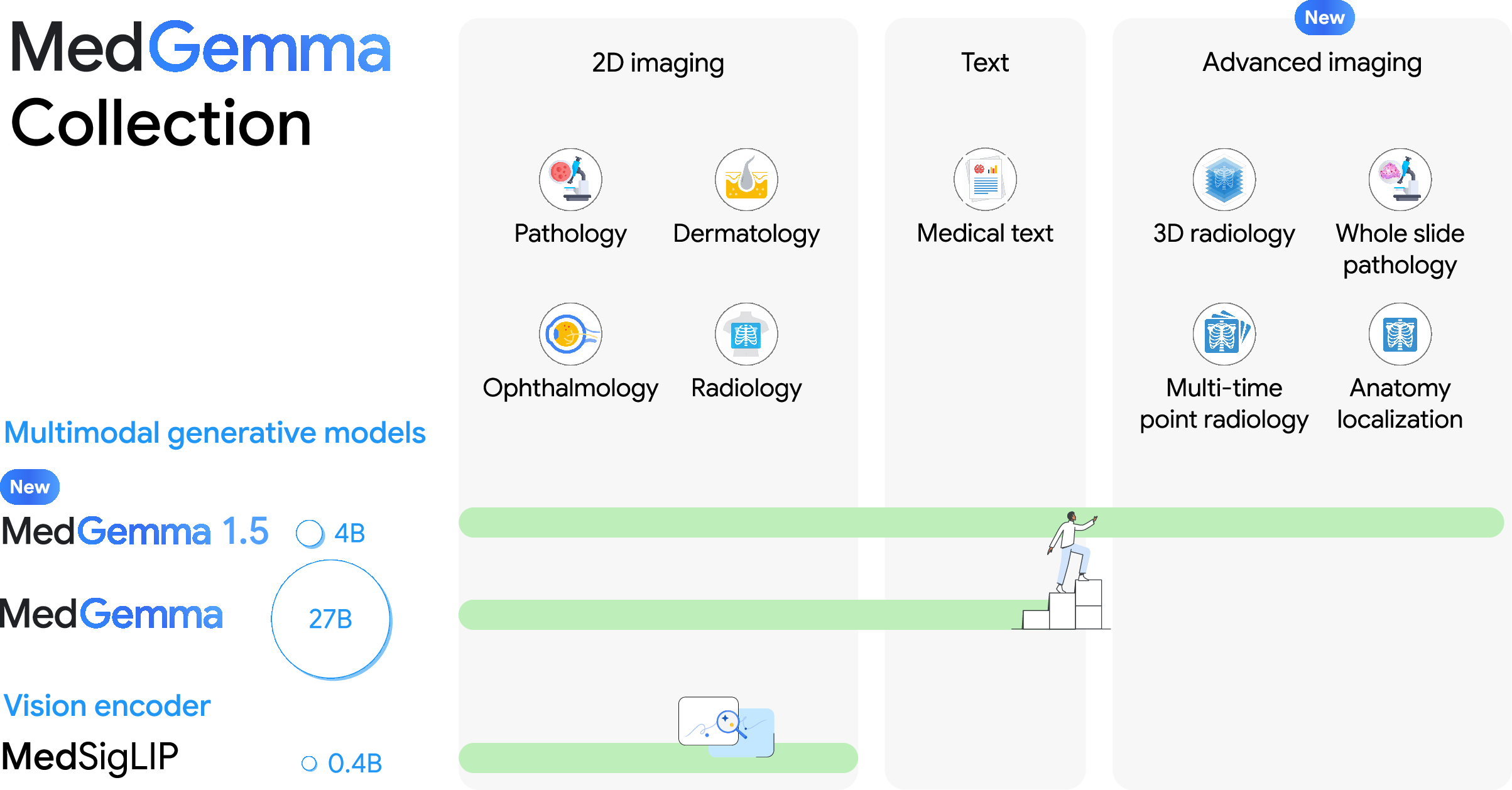
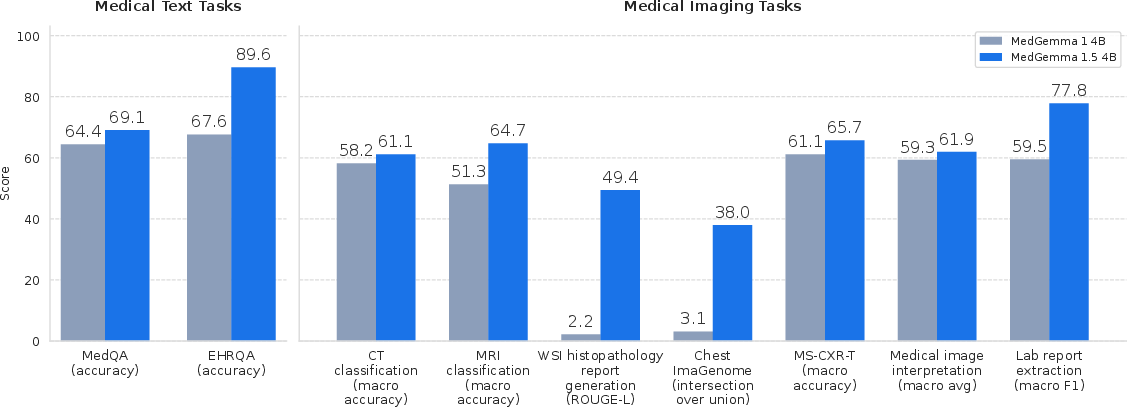
Abstract: We introduce MedGemma 1.5 4B, the latest model in the MedGemma collection. MedGemma 1.5 expands on MedGemma 1 by integrating additional capabilities: high-dimensional medical imaging (CT/MRI volumes and histopathology whole slide images), anatomical localization via bounding boxes, multi-timepoint chest X-ray analysis, and improved medical document understanding (lab reports, electronic health records). We detail the innovations required to enable these modalities within a single architecture, including new training data, long-context 3D volume slicing, and whole-slide pathology sampling. Compared to MedGemma 1 4B, MedGemma 1.5 4B demonstrates significant gains in these new areas, improving 3D MRI condition classification accuracy by 11% and 3D CT condition classification by 3% (absolute improvements). In whole slide pathology imaging, MedGemma 1.5 4B achieves a 47% macro F1 gain. Additionally, it improves anatomical localization with a 35% increase in Intersection over Union on chest X-rays and achieves a 4% macro accuracy for longitudinal (multi-timepoint) chest x-ray analysis. Beyond its improved multimodal performance over MedGemma 1, MedGemma 1.5 improves on text-based clinical knowledge and reasoning, improving by 5% on MedQA accuracy and 22% on EHRQA accuracy. It also achieves an average of 18% macro F1 on 4 different lab report information extraction datasets (EHR Datasets 2, 3, 4, and Mendeley Clinical Laboratory Test Reports). Taken together, MedGemma 1.5 serves as a robust, open resource for the community, designed as an improved foundation on which developers can create the next generation of medical AI systems. Resources and tutorials for building upon MedGemma 1.5 can be found at https://goo.gle/MedGemma.
Paper Prompts
Sign up for free to create and run prompts on this paper using GPT-5.
Top Community Prompts
Explain it Like I'm 14
What is this paper about?
This paper introduces MedGemma 1.5, a new version of an open medical AI model from Google Research and Google DeepMind. Think of it as a smart assistant that can read and reason over both medical images and medical text. Unlike earlier versions that mostly handled flat 2D images (like single X‑rays), MedGemma 1.5 also understands:
- 3D scans (CT and MRI), which are like a loaf of bread made of many image “slices”
- Very large microscope images called whole‑slide images (WSIs) used in pathology
- Where things are in an image (by drawing boxes around them)
- How a patient’s images change over time (comparing “before” and “after” X‑rays)
- Medical documents like lab reports and electronic health records (EHRs)
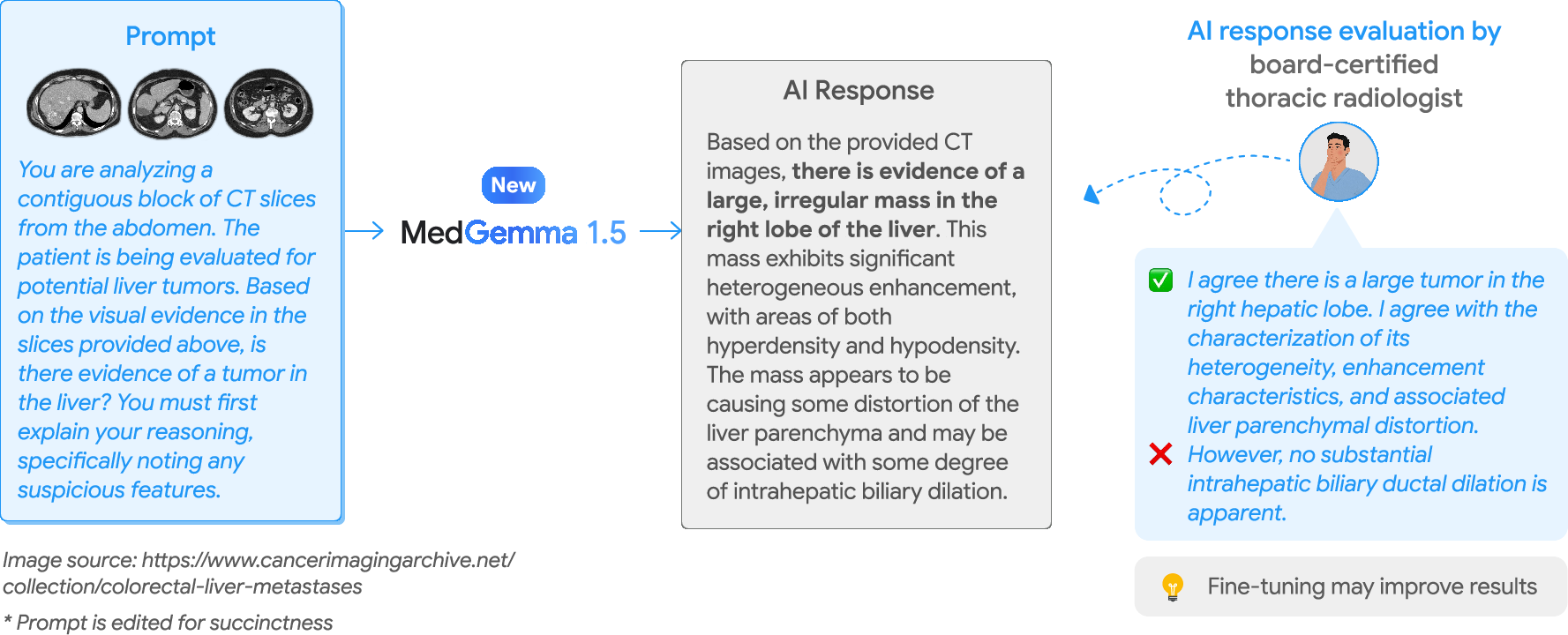
The goal is to give researchers and developers a strong, open starting point for building useful healthcare tools—while making clear it’s not ready for direct clinical use without further fine‑tuning and validation.
What questions were the researchers trying to answer?
In simple terms, they asked:
- Can a single, compact AI model handle many kinds of medical data at once (images, 3D scans, giant slide images, and long documents)?
- Can it learn to spot medical problems in 3D CT/MRI scans and describe what it sees in large pathology slides?
- Can it find the right spots in chest X‑rays (by drawing accurate boxes)?
- Can it track if a patient’s condition got better or worse when comparing two chest X‑rays?
- Can it read messy medical documents and pull out key facts accurately?
- And can it improve its medical question‑answering skills at the same time?
How did they build and train the model?
They started from a small but capable language‑and‑vision model and upgraded it with more medical skills.
- The “vision encoder” (the part that sees images) was kept fixed.
- The “language decoder” (the part that reads, reasons, and writes answers) was further trained with medical data.
To teach it well, they used three main training ideas:
- Continued pretraining (like more lessons): feeding it lots of paired images and text from medical sources.
- Distillation (teacher‑student learning): a stronger “teacher” model shows many possible next‑word hints, and the “student” (MedGemma 1.5) learns from that guidance—similar to learning from a tutor’s worked examples.
- Reinforcement learning (practice with feedback): the model tries answers and gets nudged toward better ones using rewards.
How it handles 3D scans and huge slides
AI vision models usually take 2D color pictures. The team turned complex medical images into sequences the model can digest:
- 3D CT/MRI scans: They slice the scan into many thin images (like cutting a loaf of bread) and feed a selected set of slices in order. For CT, they also adjust brightness/contrast in smart ways (like photo filters) to highlight bones, soft tissue, or subtle brain features. For MRI, they normalize the brightness consistently.
- Whole‑slide pathology images: These are enormous. The team cuts them into a grid of small image tiles (like cropping a giant poster into squares) and sends a limited number of representative tiles to the model in the slide’s original layout.
For documents (EHRs, lab reports), they trained the model to read the pages and turn important items—like test names, results, and units—into a clean, structured format (like a tidy spreadsheet or a JSON record).
What did they find?
Here are the main takeaways, expressed simply:
- Better at 3D scans:
- MRI condition classification improved by about 11 percentage points compared to the previous version.
- CT condition classification improved by about 3 percentage points.
- Better at huge pathology slides:
- Big jump in performance when turning whole‑slide images into diagnostic text (large improvement from almost unusable to very useful on their metric).
- Better at pointing to the right places:
- Stronger at drawing boxes around key anatomy in chest X‑rays, with a large improvement in overlap with expert boxes (mean IoU up to ~38% from ~3% in the small model comparison inside their tests).
- Better at reading change over time:
- Improved at telling whether chest X‑ray findings got better, worse, or stayed the same across two timepoints (macro accuracy rose by several percentage points).
- Better at clinical text and document tasks:
- Improved medical Q&A accuracy (e.g., +5% on MedQA).
- Much better at answering questions about EHRs (+22% on EHRQA).
- Improved extraction of lab report details (average macro F1 gains across multiple datasets, meaning it pulled out names, results, units, and times more accurately).
Why this matters: It shows a relatively small, efficient model can understand complex medical images and documents together, opening the door to tools that help clinicians and researchers work faster and more consistently.
Why does this matter?
- Many medical tasks aren’t just about “seeing” a picture or “reading” text—they need both. MedGemma 1.5 shows a single model can handle 3D images, huge slides, time‑based comparisons, and long documents all in one place.
- Because it’s open and efficient, teams can adapt it to their own hospitals, specialties, or datasets, rather than building everything from scratch.
- It’s a step toward AI that supports doctors with time‑consuming tasks like summarizing slides, locating findings, tracking changes over time, and organizing lab results.
What are the limits and what’s next?
- Not for direct clinical use “as‑is”: The team stresses it should be fine‑tuned and carefully validated for each real‑world use case.
- Trade‑offs: As the model became more of a “medical generalist,” it dipped slightly on a few older benchmarks that don’t perfectly reflect real clinical needs. These can likely be recovered with targeted fine‑tuning.
- Future work: Better prompts, more training data, and more domain‑specific tuning should continue to improve accuracy and reliability.
Bottom line
MedGemma 1.5 is a compact, open medical AI that can:
- Read complex medical images (including 3D scans and giant pathology slides),
- Locate findings in images,
- Compare images over time,
- And understand medical documents.
It’s not a doctor and shouldn’t be used for patient care without further work, but it’s a strong foundation for building the next generation of medical AI tools.
Knowledge Gaps
Knowledge gaps, limitations, and open questions
Below is a focused list of what remains missing, uncertain, or unexplored based on the paper; each point is phrased to be actionable for future work.
- Impact of a frozen vision encoder: quantify performance gains/losses if the 400M MedSigLIP encoder is partially or fully fine-tuned, especially on high-dimensional tasks (3D CT/MRI, WSI).
- 2D slicing vs native 3D modeling: compare the current 2D-slice pipeline to true 3D encoders (3D CNN/ViT, factorized attention) for CT/MRI to assess spatial continuity, lesion detectability, and efficiency.
- Long-context constraints: study how the 32K token cap, 85-slice CT/MRI limit, and 126-patch WSI cap affect sensitivity to small or sparse findings; evaluate adaptive slice/patch selection, learned retrieval, or hierarchical encoders to retain critical context.
- Preprocessing ablations for CT/MRI: systematically test HU window triplets, per-volume MR normalization, slice resolution (896×896), resampling, and equidistant sampling vs. pathology-aware sampling on condition-level and localization metrics.
- Orientation and thickness generalization: evaluate robustness to non-axial planes, mixed orientations, variable slice thickness, multi-sequence MR with differing resolutions, and multi-kernel CT stacks.
- Use of clinical history in prompts: ablate patient history text in CT/MRI prompts to quantify its contribution vs. image-only performance and risk of label leakage.
- Probability calibration and uncertainty: replace/augment generative yes/no outputs with calibrated probabilities; evaluate ECE, AUROC, selective prediction, and abstention policies per task.
- Label quality for internal 3D datasets: measure and publish inter-rater agreement and noise rates for labels derived via RegEx + Gemini extraction; expand blinded radiologist adjudication coverage and error taxonomy.
- External 3D benchmarks: evaluate on widely used public datasets (e.g., LIDC-IDRI for nodules, BraTS for brain tumors, LiTS for liver lesions) for comparability and lesion-level sensitivity/specificity.
- Beyond condition classification: extend CT/MRI to detection, localization, and segmentation (e.g., 3D boxes or masks) and evaluate clinically relevant endpoints (lesion size tracking, burden, progression).
- Temporal modeling beyond pairs: develop and test architectures for multi-visit temporal fusion (3+ timepoints) for CXR and extend to CT/MRI longitudinal analysis; assess robustness to inter-study acquisition differences.
- WSI tiling strategy: compare non-overlapping vs overlapping tiles, multi-scale tiling, and learned tile selection; quantify the effect of random magnification choice and 126-tile cap on slide-level diagnostic fidelity.
- WSI evaluation metrics: complement ROUGE-L with clinically grounded metrics (pathologist scoring, case-level accuracy, tumor detection/grade/stage) and evaluate on public WSI datasets for reproducibility.
- Anatomical vs pathological localization: extend bounding-box localization from anatomy to pathology findings; compare box vs segmentation metrics and assess IoU calibration and clinical tolerances.
- JSON-format robustness: test the bounding-box JSON output for robustness to prompt variations, malformed outputs, and coordinate normalization errors; implement constrained decoding or schema validation.
- Document understanding generalization: evaluate lab-report parsing across institutions, templates, languages, OCR noise, handwriting, stamps, and low-quality scans; benchmark against specialized OCR+NLP pipelines and LOINC mapping accuracy end-to-end.
- Beyond lab reports: test broader clinical document types (radiology/pathology reports, discharge summaries, referrals) with structured extraction targets (FHIR resources) and multi-page cross-reference consistency.
- Bias and fairness: audit performance by demographic subgroups, scanner vendors, institutions, and geographies (e.g., India vs U.S. sites) for each modality; address disparate error rates with mitigation strategies.
- Safety and reliability: conduct adverse-case analyses (hallucinations, unsafe advice), red-teaming for prompt injection and instruction drift, and uncertainty-aware guardrails; report failure modes.
- Catastrophic forgetting/multi-task interference: quantify regressions across legacy tasks; study task-balanced sampling, modular heads, or continued-pretraining regimes to mitigate interference.
- Cross-model inference comparability: re-run baselines with standardized decoding settings, multiple seeds, and statistical testing; report variance and significance to ensure fair comparisons.
- Teacher/distillation transparency: document teacher model architectures, training data, and domain coverage; ablate teacher mixtures and RL reward design to isolate contributions and potential biases.
- Efficiency and deployment: report latency, memory, and throughput for long-context inference (e.g., 20k–30k vision tokens); explore compression (kv-caching strategies, token pruning) and cost-quality trade-offs.
- Multilingual capacity: evaluate and/or train for non-English clinical text and non-English report templates, including mixed-language settings common in healthcare systems.
- Multi-modal temporal EHR+imaging reasoning: create benchmarks requiring joint reasoning over longitudinal imaging and evolving EHR notes/labs; assess clinical trajectory prediction and decision support utility.
- Clinical validation: perform reader studies (assisted vs unassisted), time-to-diagnosis, and non-inferiority trials; quantify workflow integration benefits and human-AI complementarity.
- Data governance and privacy: clarify de-identification methods for internal datasets and WSIs; assess re-identification risks and compliance with local regulations for model training and release.
- Robustness to acquisition shifts: test OOD generalization across institutions, devices, reconstruction kernels, and protocols; evaluate test-time adaptation or domain generalization techniques.
- Extending modalities: explore ultrasound, echocardiography, endoscopy, and video-based tasks with temporal encoders and audio-text fusion where applicable.
- Prompt sensitivity: quantify performance sensitivity to prompt wording; develop prompt-robust training (instruction augmentation) and task adapters to reduce manual prompt engineering burden.
Practical Applications
Immediate Applications
Below are deployable use cases that leverage MedGemma 1.5’s current capabilities as a foundation model. These focus on non-diagnostic, backend, and research/ops workflows that benefit from multimodal, long-context processing but do not constitute autonomous clinical decision-making.
- Lab report digitization and structuring for analytics and interoperability (Healthcare IT, LIS/EHR vendors, Payers, Public Health)
- What: Convert scanned/digital lab reports to structured JSON as a precursor to LOINC mapping and FHIR DiagnosticReport generation; feed data lakes, quality reporting, and surveillance pipelines.
- Tools/products/workflows: “Document-to-JSON” microservice (PDF→image via pypdfium2 → MedGemma 1.5 extraction → JSON → LOINC/FHIR transform); RPA to populate registries and HEDIS measures.
- Assumptions/dependencies: Template variability and OCR noise; site-specific finetuning; clinical QA; HIPAA/GDPR-compliant deployment; downstream LOINC mapping still required.
- EHR question answering over discharge summaries for clinician prep and CDI teams (Healthcare providers, EHR vendors; Academia for evaluation)
- What: Answer MCQs about patient history/treatments from discharge notes to support chart navigation, rounding prep, and documentation improvement.
- Tools/products/workflows: EHRNoteQA-style component in clinician-facing dashboards; on-prem inference for PHI; human-in-the-loop confirmation.
- Assumptions/dependencies: Not for diagnostic advice; local validation and prompt governance; latency and context-window management for long notes.
- Imaging data indexing, triage, and curation in research data lakes (Academia, Biopharma RWD teams, PACS/VNA vendors)
- What: Use coarse 3D CT/MRI classification and longitudinal CXR change detection to auto-tag studies (e.g., “possible aneurysm,” “effusion worsened”), enabling cohort discovery and data retrieval; use WSI-to-text summaries to index slides.
- Tools/products/workflows: DICOMweb ingestion → volume slicing/HU windowing → batch inference → metadata tagging; WSI patch-extraction pipeline for slide indexing.
- Assumptions/dependencies: Research-only labeling (non-clinical); radiologist/pathologist spot checks; domain shift across scanners/sites; compute for long sequences.
- Bounding-box anatomical localization as an annotation accelerator (Imaging AI vendors, Academic labs)
- What: Generate draft ROIs on chest X-rays to speed dataset labeling and internal QA (e.g., anatomy coverage checks, protocol compliance).
- Tools/products/workflows: Annotation tool plug-in that auto-seeds boxes; QC workflow to accept/edit model suggestions; export COCO-like JSON.
- Assumptions/dependencies: Box quality varies by anatomy; requires human review; normalization of coordinates to image size; institution-specific calibration.
- Pathology WSI pre-screening for operations and archival search (Pathology labs, Digital pathology software vendors)
- What: Produce short slide-level summaries to route cases (e.g., probable organ/site) and enable search in archives without reading full gigapixel slides.
- Tools/products/workflows: Slide tiling/patch sampling → MedGemma 1.5 summary → LIS/WSI viewer integration for triage queues and search indexing.
- Assumptions/dependencies: Not for diagnosis; magnification/scan variability; color normalization differences; pathologist oversight.
- Patient-facing lab/exam explanation for health literacy (Daily life; Payer/provider portals)
- What: Educational summaries of lab reports or discharge notes for patients and caregivers (non-advisory), with links to authoritative sources.
- Tools/products/workflows: Portal widget that parses uploaded reports → lay-language summary + glossary; disclaimers and handoffs to clinicians.
- Assumptions/dependencies: Strict non-diagnostic positioning; plain-language validation; privacy-safe on-device or on-prem deployment where feasible.
- Open-weight baseline for multimodal medical ML education and benchmarking (Academia)
- What: Teach multimodal pre-processing (3D slicing, WSI patching), prompt engineering for medical tasks, and benchmarking of spatiotemporal tasks.
- Tools/products/workflows: Course labs using MedGemma 1.5 checkpoints; reproducible pipelines for CT/MRI/WSI/CXR tasks; shared prompts and metrics.
- Assumptions/dependencies: Compute for long-context inference; access to permitted datasets; clear separation from clinical use.
- On-prem privacy-preserving model-as-a-service for PHI-intensive workflows (Healthcare IT, Cloud/on-prem integrators)
- What: Run an open 4B model inside hospital firewalls for document extraction, imaging metadata tagging, and internal search.
- Tools/products/workflows: Containerized inference (with quantization) behind hospital VPN; DICOMweb/FHIR connectors; audit logging.
- Assumptions/dependencies: MLOps for updates/monitoring; throughput tuning; GPU/CPU availability; institutional security review.
Long-Term Applications
These use cases require additional finetuning, validation, scaling, and/or regulatory clearance before clinical deployment.
- Clinical decision support for 3D radiology (triage, prioritization, and structured reporting) (Healthcare providers, PACS/RIS vendors)
- What: Triage CT/MRI volumes for suspected high-acuity findings (e.g., ICH, aneurysm); generate structured impressions; compare priors for interval change.
- Tools/products/workflows: PACS plug-in with series-level pre-screen and change summaries; structured templates (e.g., RadLex/SNOMED); radiologist-in-the-loop editing.
- Assumptions/dependencies: Prospective multi-site validation; robustness across scanners/kernels; regulatory clearance; latency constraints for emergency settings.
- Computer-assisted digital pathology (WSI) with region proposals and slide-level suggestions (Pathology labs, WSI viewer vendors)
- What: ROI ranking, suspected tissue/organ/site detection, and draft diagnostic descriptors to accelerate primary reads and QA.
- Tools/products/workflows: Interactive WSI viewer overlay; uncertainty-aware proposals; concordance auditing; integration with LIS sign-out.
- Assumptions/dependencies: High-stakes validation; stain and lab protocol variability; pathologist acceptance and workflow fit; regulation.
- End-to-end multimodal report generation and longitudinal disease tracking (Radiology, Pulmonology/Cardiology service lines)
- What: Auto-generate initial reports from current + prior images and EHR context; timeline visualizations for pathology trajectories (e.g., edema trend).
- Tools/products/workflows: EHR/FHIR pull of priors → imaging + text fusion → draft report + change assessment → structured output to EHR.
- Assumptions/dependencies: Guardrails to avoid hallucinations; human-in-the-loop sign-off; medico-legal frameworks; reliability across edge cases.
- Multimodal clinical agents for differential diagnosis and care planning (Healthcare providers; Clinical AI platforms)
- What: Agentic systems that reason jointly over labs, notes, and imaging to surface differentials, next-step tests, and guideline-based care pathways.
- Tools/products/workflows: Tool-using agents with retrieval, calculators, and order sets; provenance tracking; safety layers and counterfactual checks.
- Assumptions/dependencies: Robustness to spurious correlations; continuous QA; regulatory pathway for decision support; clinician governance.
- Automated clinical trial screening leveraging imaging + EHR (Biopharma, Academic medical centers)
- What: Identify eligible patients by matching inclusion/exclusion criteria against structured EHR data and coarse imaging findings or change patterns.
- Tools/products/workflows: Criteria codification → FHIR-based querying → imaging tags from MedGemma → coordinator review workflow.
- Assumptions/dependencies: Site-specific finetuning; recall-vs-precision trade-offs; IRB and patient consent; bias monitoring.
- Population health and disease registries augmented by document and imaging mining (Public health agencies, Payers)
- What: Scalable ingestion of scanned lab reports and imaging summaries to maintain registries (e.g., TB, cancer, cardiopulmonary disease) and track trends.
- Tools/products/workflows: Ingestion microservices → normalization (LOINC/FHIR) → surveillance dashboards; de-duplication logic.
- Assumptions/dependencies: High accuracy thresholds; jurisdictional data sharing rules; equity and bias oversight.
- Revenue cycle and utilization management supported by structured evidence extraction (Payers, Provider revenue cycle)
- What: Extract medically necessary evidence from notes and images to support pre-authorization and audits; reduce manual chart review.
- Tools/products/workflows: Evidence summarization API; attach structured findings to requests; audit trail generation.
- Assumptions/dependencies: Policy compliance and explainability; alignment with payer guidelines; appeals processes.
- Edge/embedded deployment for point-of-care devices and mobile viewers (Medical device OEMs, Telehealth)
- What: Low-parameter, quantized multimodal inference on modalities (e.g., portable X-ray, handheld ultrasound) for on-device pre-screen and metadata tagging.
- Tools/products/workflows: Model compression/quantization; DICOM on-device parsing; streaming inference.
- Assumptions/dependencies: Throughput and power constraints; rigorous validation in varied environments; secure update mechanisms.
- Standards and policy tooling for multimodal health data integration (Standards bodies, Health systems)
- What: Reference pipelines that transform unstructured documents and imaging context into FHIR resources and standard vocabularies (LOINC/SNOMED).
- Tools/products/workflows: Open reference implementations; conformance test suites; procurement guidelines for open-weight medical foundation models.
- Assumptions/dependencies: Cross-vendor interoperability; governance for updates; sustained community maintenance.
Cross-cutting dependencies and assumptions
- Clinical use requires fine-tuning on local data, prospective validation, and regulatory approval; out-of-the-box model is not for autonomous diagnosis or treatment.
- Data variability (scanner vendors, protocols, document templates, languages) and domain shift must be addressed; prompt and preprocessing choices materially affect performance.
- Long-context inference incurs compute/memory costs; batching and quantization strategies may be necessary for production.
- PHI handling demands on-prem or strongly isolated deployment, robust logging, and access controls.
- Human oversight is essential for high-stakes tasks; workflows should be built for efficient review, correction, and feedback.
Glossary
- Anatomical localization: Identifying and specifying the positions of anatomical structures within medical images, often via structured outputs like boxes or coordinates. "anatomical localization via bounding boxes"
- Axial orientation: The imaging plane aligned perpendicular to the body’s long axis; axial slices are horizontal cross-sections used in CT/MRI. "axial orientation"
- Bounding boxes: Rectangular regions used to localize objects or anatomy in images by specifying coordinates. "generate coordinates of 2D bounding boxes"
- Cross-entropy loss: A loss function measuring the difference between two probability distributions, commonly used for classification and distillation. "via cross-entropy loss"
- Distillation: A training technique where a smaller “student” model learns to mimic a larger “teacher” model’s output distribution. "Distillation here means we sample 256 teacher model logits per token, weighted by teacher probabilities."
- Fast Healthcare Interoperability Resources (FHIR): A standard for structuring and exchanging healthcare data between systems. "Question/answer dataset drawn from synthetic FHIR records."
- Gradient Echo (GRE): An MRI pulse sequence that emphasizes T2* contrast, useful for detecting certain tissue properties. "including T1-weighted (T1w), T2-weighted (T2w), GRE, and SWI."
- Hounsfield Units (HU): A standardized scale of radiodensity used in CT imaging to quantify tissue attenuation. "we employed multi-channel windowing to map raw Hounsfield Units (HU) to RGB values"
- HSV color space: A color representation defined by Hue, Saturation, and Value, often used in image segmentation tasks. "operating in the HSV (Hue, Saturation, Value) color space."
- Intersection over Union (IoU): A metric for localization accuracy measuring the overlap between predicted and ground-truth boxes divided by their union. "The primary metric for evaluating localization performance was the Intersection over Union (IoU)."
- Logical Observation Identifiers Names and Codes (LOINC): A universal code system for identifying laboratory and clinical observations. "such as LOINC (Logical Observation Identifiers Names and Codes) mapping"
- Long-context 3D volume slicing: Converting volumetric scans into long sequences of 2D slices to fit models with extended context windows. "long-context 3D volume slicing"
- Longitudinal imaging: Analysis of patient images acquired over multiple time points to assess disease progression. "temporal reasoning within longitudinal medical imaging"
- Logits: The raw, unnormalized scores output by a model before applying softmax to obtain probabilities. "256 teacher model logits per token"
- Macro accuracy: Accuracy averaged equally across classes or tasks, mitigating class imbalance effects. "using the macro accuracy metric to account for class imbalance"
- Macro F1: The unweighted mean F1 score across classes or datasets, giving each class equal importance. "achieves an average of 18\% macro F1 on 4 different lab report information extraction datasets"
- MedSigLIP encoder: A specialized medical vision encoder (based on SigLIP) used to process images in the model. "The vision encoder is 400M MedSigLIP encoder"
- Min-max normalization: Scaling data so that values fall within a fixed range, typically [0, 1]. "we normalized them per volume using min-max normalization"
- Multi-channel windowing: Mapping CT intensities into multiple window ranges across RGB channels to emphasize different tissues. "we employed multi-channel windowing"
- Multi-parametric MRI: MRI acquisitions comprising multiple sequences/contrasts to capture diverse tissue characteristics. "axial multi-parametric MRI studies"
- Out of Distribution (OOD): Data that differ from what the model encountered during training, used to test generalization. "Out of Distribution: Data not seen during any model development stages."
- Optical magnification level: The microscope zoom factor (e.g., 5x, 10x, 20x) used when extracting patches from whole-slide images. "a single optical magnification level was stochastically selected"
- RadGraph F1: An information-extraction–based metric evaluating the clinical correctness of generated radiology reports via graph comparisons. "a radiology report generation metric (RadGraph F1"
- Reconstruction kernels: Algorithmic filters applied during CT image reconstruction that influence image sharpness and noise characteristics. "volumes with different reconstruction kernels originating from the same scan"
- Reinforcement learning (RL): A training paradigm that optimizes models via reward signals, often used for post-training alignment. "reinforcement learning (RL)"
- ROUGE-L: A text evaluation metric based on the longest common subsequence between generated and reference text. "RL (on token-level ROUGE-L)"
- Susceptibility Weighted Imaging (SWI): An MRI sequence sensitive to magnetic susceptibility differences, highlighting veins, blood products, and calcifications. "including T1-weighted (T1w), T2-weighted (T2w), GRE, and SWI."
- T1-weighted (T1w): An MRI contrast that emphasizes differences in T1 relaxation, often highlighting fat and anatomy. "including T1-weighted (T1w), T2-weighted (T2w), GRE, and SWI."
- T2-weighted (T2w): An MRI contrast emphasizing T2 relaxation differences, often highlighting fluid and edema. "including T1-weighted (T1w), T2-weighted (T2w), GRE, and SWI."
- Tissue mask: A binary segmentation identifying tissue-containing regions on a whole-slide image to guide patch extraction. "A tissue mask was generated for each slide at a low resolution (5x magnification)."
- Tokenized F1: F1 score computed on tokenized outputs, used to evaluate free-form VQA answers. "we evaluated average tokenized F1 on SLAKE"
- Vision tokens: Discrete token representations derived from images/patches for processing by a vision-LLM. "which amount to 21,760 vision tokens"
- Voxel: A volumetric pixel representing a value in a 3D image grid. "since voxel values of MR images are all relative"
- Whole Slide Image (WSI): A high-resolution digital scan of an entire pathology slide for computational analysis. "pathology whole slide imaging (WSI)"
- z-axis: The depth dimension of a volumetric scan along which slices are stacked. "equidistantly across the z-axis (of the stacked volume)."
- z-stacked volumes: Multiple 3D volumes combined along the depth axis to create a larger stack of slices. "Slices could originate from multiple z-stacked volumes per study."
Collections
Sign up for free to add this paper to one or more collections.