- The paper introduces NeuroVase, a tangible mobile AR system that fuses interactive 3D neuroanatomical visualizations with physical cue cards for enhanced neurovascular and stroke education.
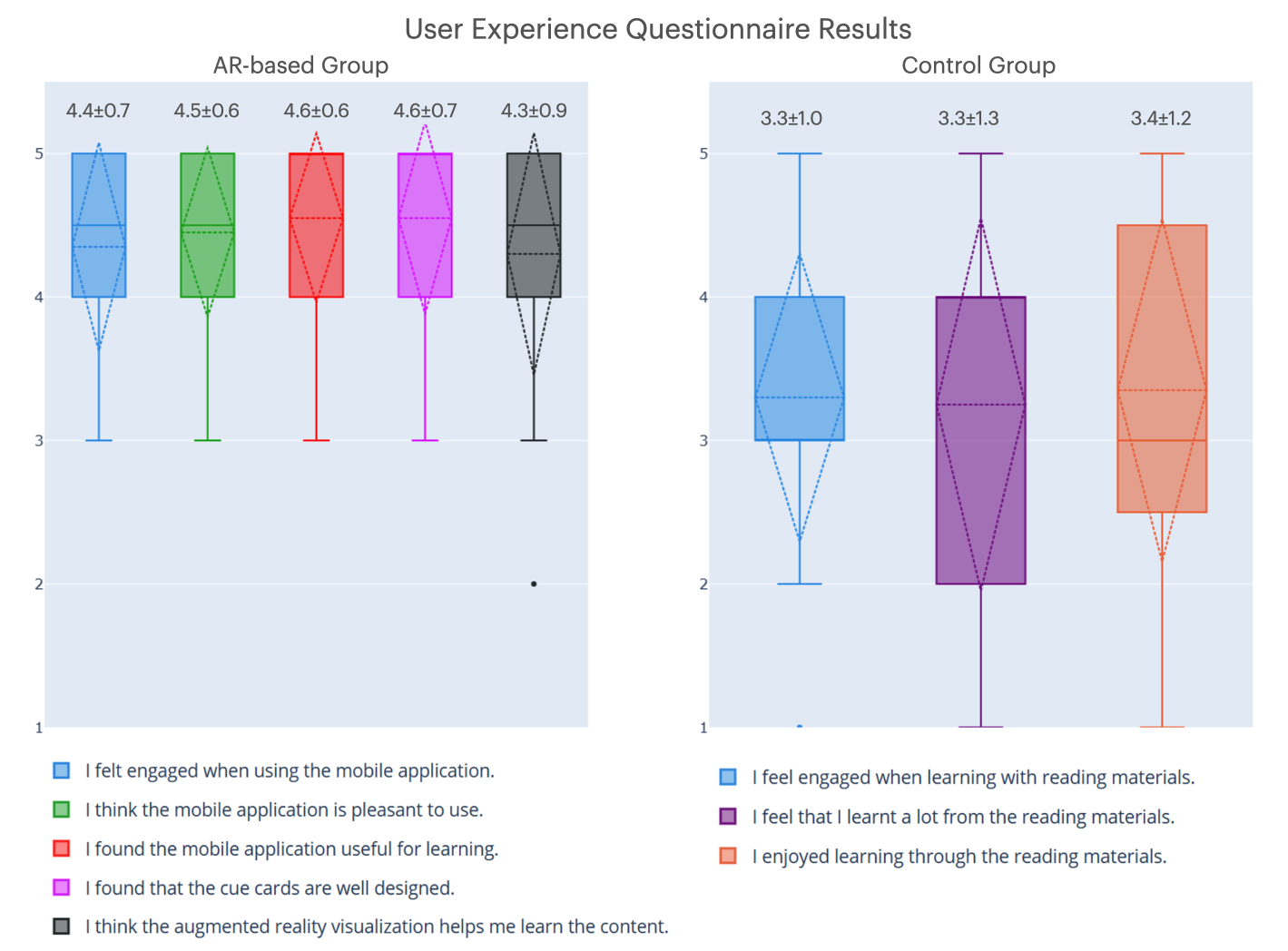
- The paper demonstrates a dual-mode curriculum leveraging AR gestures and cue cards, achieving high usability (SUS=90.0±5.7) and superior user engagement compared to traditional methods.
- The controlled study reveals significant learning improvements and user satisfaction while highlighting technical challenges such as cue card tracking under variable conditions.
NeuroVase: Tablet-Based Tangible AR for Neurovascular Anatomy and Stroke Education
Introduction
NeuroVase introduces a tangible mobile AR system designed to address deficiencies in current neurovascular and stroke education. The platform delivers interactive three-dimensional neuroanatomical and cerebrovascular visualizations, leveraging physical cue cards for both augmented interaction and offline study. The design aims to overcome the spatial and clinical complexities that impede traditional 2D neuroanatomy curricula, providing context-rich and scalable pedagogical interventions on consumer-grade tablets.
System Architecture and User Interaction
The NeuroVase platform utilizes a dual-mode curriculum integrating AR visualizations and tangible cue cards. The cue cards, using carefully selected high-contrast anatomical images with QR codes, serve as both physical AR targets and standalone learning aids. When the master card is positioned in the camera field, the core 3D neuroanatomical model is rendered and anchored within the AR interface. Trigger cards update content contextually, allowing modular progression through lobar anatomy, arterial vasculature, and arterial territories.
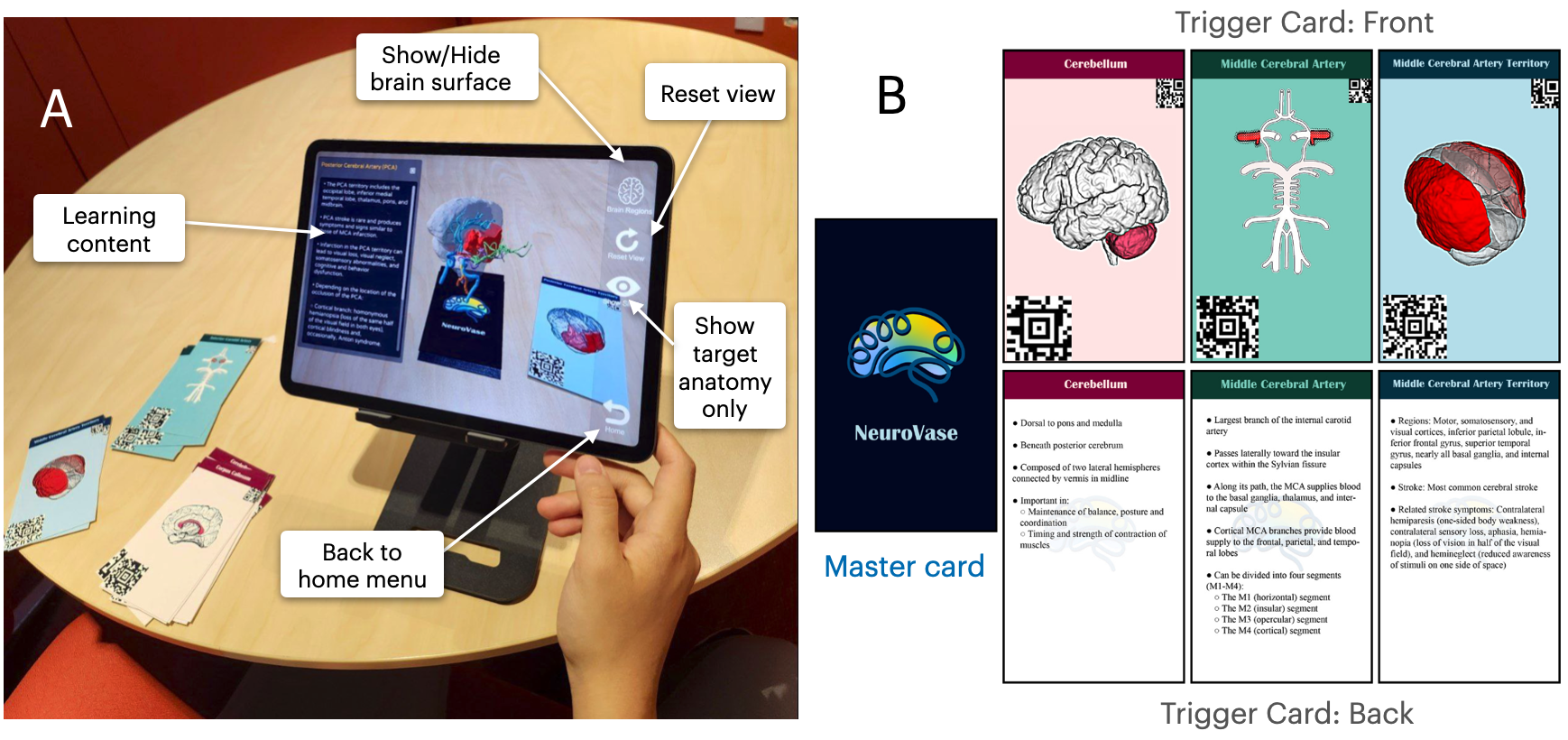
Figure 1: The AR user interface leverages tangible cue cards for content-triggering and spatial interaction, seamlessly integrating physical and virtual content delivery.
The interface supports canonical AR gestures (pinch/zoom/rotate/translate), with a rigid assignment of cue cards to content modules to maintain linear pedagogical flow. The design supports structured, progressive learning aligned with clinical reasoning relevant to stroke management.
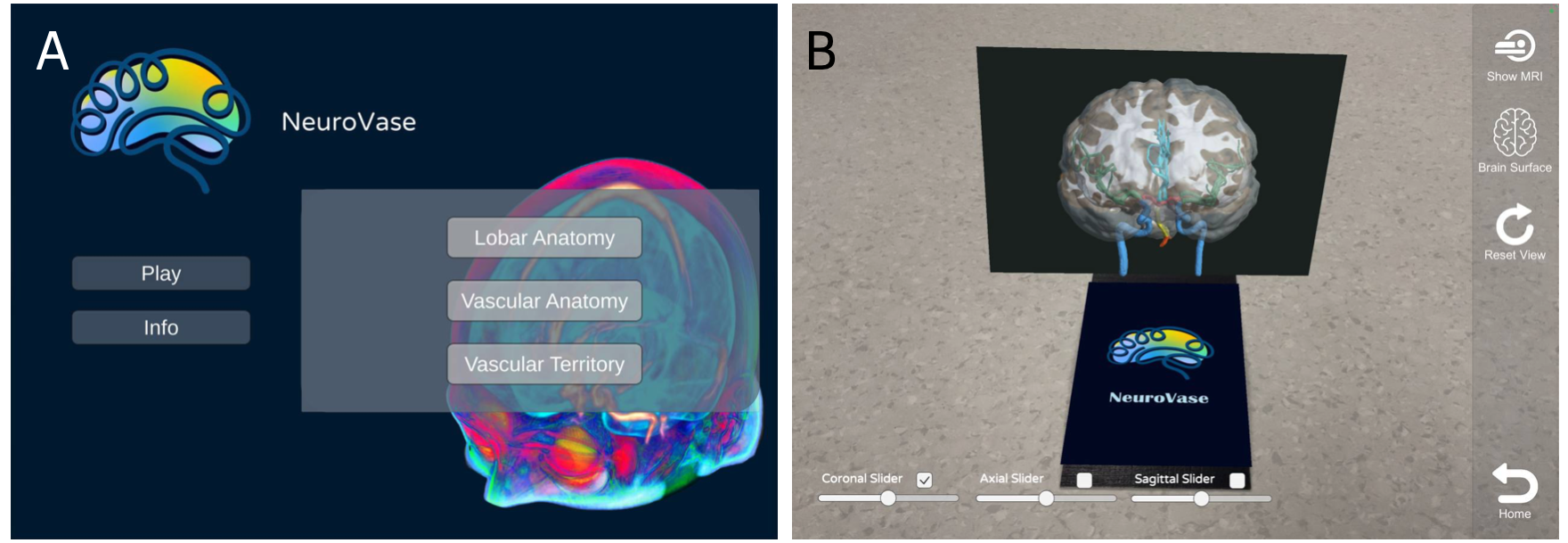
Figure 2: The main menu allows users to select between core modules and engage with high-fidelity MRI overlays in the Vascular Anatomy section.
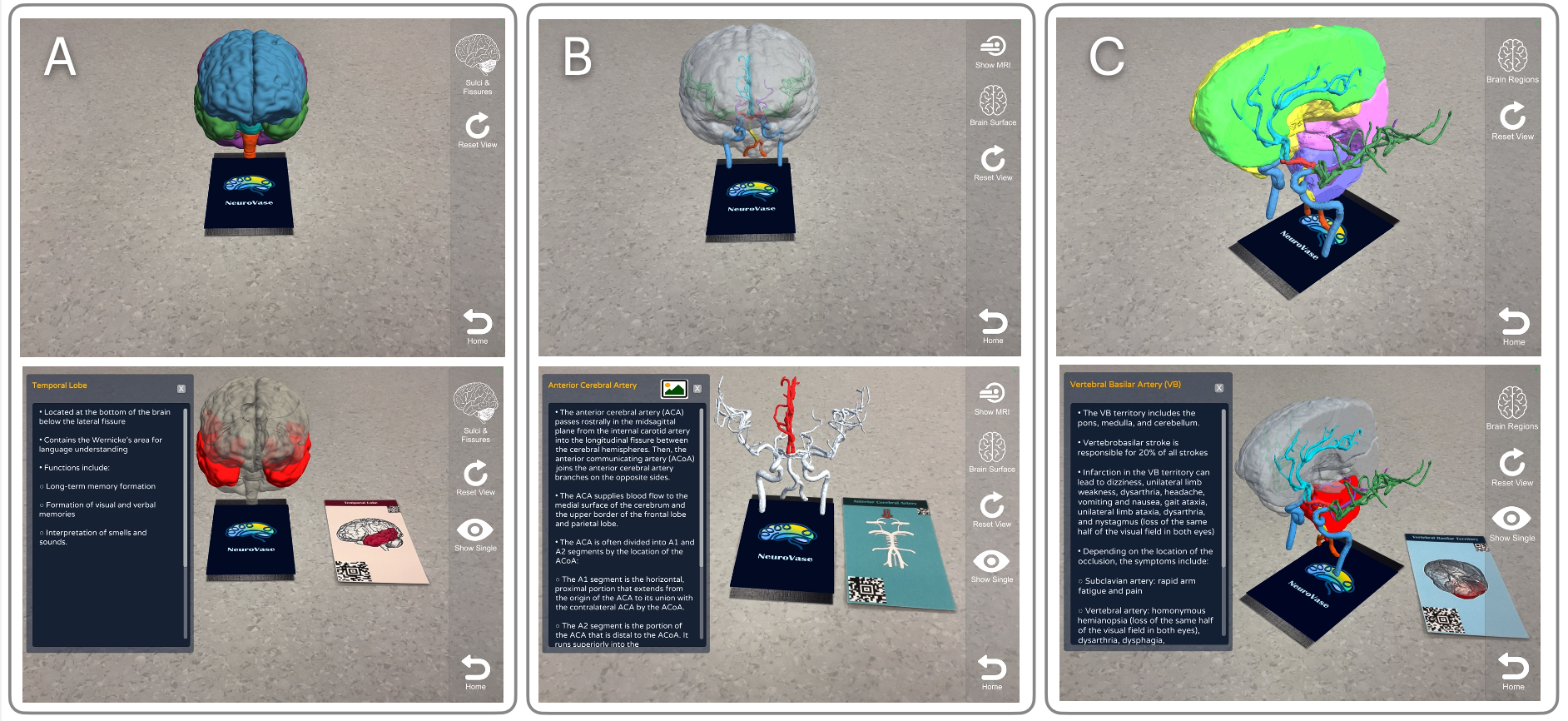
Figure 3: Example module states showing pre- and post-trigger activation for lobar, arterial, and territory-specific content.
Pedagogical Content and Model Construction
The content framework was constructed with domain expert curation, integrating three neuroanatomy modules of increasing complexity:
- General lobar anatomy: Extracted and segmented from the BCI-DNI atlas for high anatomic fidelity.
- Cerebral arterial system: Modeled using multi-modal MRI/MRA data and refined using Frangi-based vessel enhancement and ITK-SNAP segmentation.
- Vascular territories: Registered from a large-scale clinical stroke atlas (1,298-patient cohort) for territory boundary definition and pathophysiological correlation.
MRI overlays and vessel renderings are fused through Unity’s rendering pipeline, importing mesh data in .obj format for volumetric and surface renderings.
Controlled Study Design and Results
A parallel-arm randomized study (n=40; 20 AR, 20 control) with STEM participants of low cerebrovascular expertise assessed usability, enjoyment, and educational effectiveness. The AR cohort used the complete NeuroVase platform, while controls used matched paper materials with identical text and 2D images.
Key findings:
Implications and Theoretical Considerations
NeuroVase’s design addresses three core deficits in neuroanatomy technologies:
- Direct targeting of cerebrovascular territories and syndromic correlates, domains largely ignored by existing AR/VR systems.
- Integration of tangible interaction workflows (cue cards), bridging embodied cognition theory and digital visualization.
- An extensible, modular pedagogical scaffold, with open-source release enabling community adaptation.
The measured superiority in engagement and system usability, despite parity in raw knowledge gains, suggests differentiated impact on motivation and depth of spatial learning. The lack of significant delta on post-intervention testing aligns with prior AR neuroanatomy studies, but the high user-perceived value and lower cognitive friction observed reinforce AR as an effective supplement to didactic approaches.
Technically, NeuroVase demonstrates the practical feasibility of hybrid tangible–AR interaction paradigms deployable on consumer hardware, which is a critical criterion for broad clinical and educational adoption. The pipeline for converting MRI/MRA clinical data to AR-renderable assets establishes groundwork for future AI-driven automation in medical education content generation, and the structured cue card system provides a template for gamified or adaptive curriculum extensions.
Limitations and Future Directions
Key limitations include sensitivity to physical cue card tracking under variable lighting, modest sample diversity (mostly STEM students), and possible content complexity overload for novice users. Planned directions involve:
- Augmenting model fidelity and interaction fluidity (e.g., stabilized gestures, annotation overlays, blood flow animation).
- Formal integration into clinical and undergraduate medical curricula, followed by scaled multi-institutional evaluation.
- Investigation into AI-augmentation for personalized feedback, automatic content creation from clinical neuroimaging repositories, and ML-driven assessment of spatial learning outcomes.
Conclusion
NeuroVase advances mobile AR-based neurovascular education by merging tangible cue card interfaces, high-fidelity anatomical modeling, and a robust, clinician-informed didactic sequence. The system’s high usability and user engagement, combined with its open-source approach and modular extensibility, support its utility as a scalable supplement to traditional neuroanatomy and stroke teaching. Theoretical impact includes validation of embodied learning in AR-enhanced curricula, with practical implications for rapid knowledge transfer in time-sensitive clinical training.
(2604.00296)