Making Conformal Predictors Robust in Healthcare Settings: a Case Study on EEG Classification
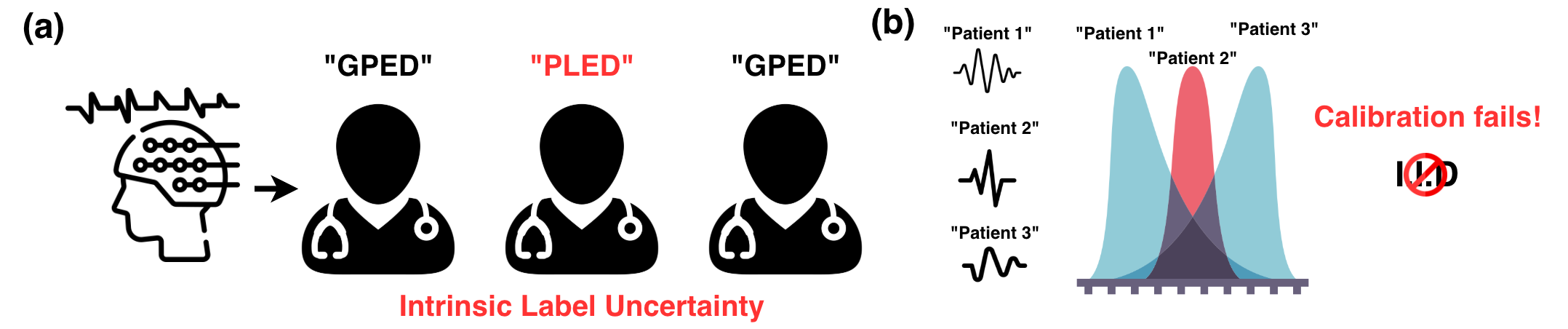
Abstract: Quantifying uncertainty in clinical predictions is critical for high-stakes diagnosis tasks. Conformal prediction offers a principled approach by providing prediction sets with theoretical coverage guarantees. However, in practice, patient distribution shifts violate the i.i.d. assumptions underlying standard conformal methods, leading to poor coverage in healthcare settings. In this work, we evaluate several conformal prediction approaches on EEG seizure classification, a task with known distribution shift challenges and label uncertainty. We demonstrate that personalized calibration strategies can improve coverage by over 20 percentage points while maintaining comparable prediction set sizes. Our implementation is available via PyHealth, an open-source healthcare AI framework: https://github.com/sunlabuiuc/PyHealth.
Paper Prompts
Sign up for free to create and run prompts on this paper using GPT-5.
Top Community Prompts
Explain it Like I'm 14
Plain-language summary of “Making Conformal Predictors Robust in Healthcare Settings: a Case Study on EEG Classification”
What is this paper about?
This paper is about making AI systems for healthcare more honest about how sure they are. The authors focus on EEG classification—using brainwave recordings to detect things like seizures. Instead of having the AI give one label and pretend it’s always right, they use a method called conformal prediction to give a small set of possible answers along with a guarantee about how often the right answer is in that set. They show that by “personalizing” this method—calibrating it using patients similar to the current one—the guarantees work much better when patients differ from those the model saw before.
What questions did the researchers ask?
The paper asks:
- How can we give trustworthy uncertainty estimates (i.e., honest “I’m not fully sure” signals) for EEG classification?
- Do standard conformal prediction methods break when the new patients look different from the patients used to calibrate the model (a common problem in hospitals)?
- Can “personalized” calibration—using examples from patients most similar to the current one—fix this problem and keep prediction sets small?
How did they do it? (Methods in simple terms)
Think of conformal prediction like a game of multiple-choice:
- Instead of giving one answer, the model gives a short list of answers.
- It aims to be right (include the true answer) at least, say, 90% of the time. That target (like 90% or 95%) is the “coverage.”
The challenge: Most methods assume the past and future patients look the same. In healthcare, that’s often untrue—patients come from different hospitals, devices, or backgrounds. This mismatch is called “distribution shift.”
The authors tested four versions of conformal prediction on two EEG datasets:
- TUAB: Decide if an EEG is normal or abnormal (binary).
- TUEV: Identify which of six EEG event types is present (multiclass).
They trained a deep learning model that turns EEG signals into features and predicts probabilities for each class. Then they wrapped conformal prediction around it in four ways:
- Naive CP: A single “one-size-fits-all” threshold for everyone.
- Covariate CP: Tries to adjust for shifts by reweighting examples (like paying more attention to samples that look like test data). This needs estimating tricky probability ratios.
- K-means CP: Breaks calibration examples into clusters and uses the cluster closest to the test patient.
- Neighborhood Conformal Prediction (NCP): For each test patient, it finds the most similar patients (nearest neighbors) and builds a custom threshold from them—like asking advice from the most relevant past cases.
In everyday terms:
- Naive CP: One general rule for everyone.
- Covariate CP: One rule, but tilted toward certain cases to fix shifts.
- K-means CP: Use the rule of the nearest group.
- NCP: Use a custom rule based on the closest few examples to the current case.
They also provide a simple theoretical explanation: if you tailor the calibration to similar patients, your accuracy-on-coverage stays steadier when the types of patients change. In other words, “local” rules wobble less than “global” rules under shifts.
What did they find, and why does it matter?
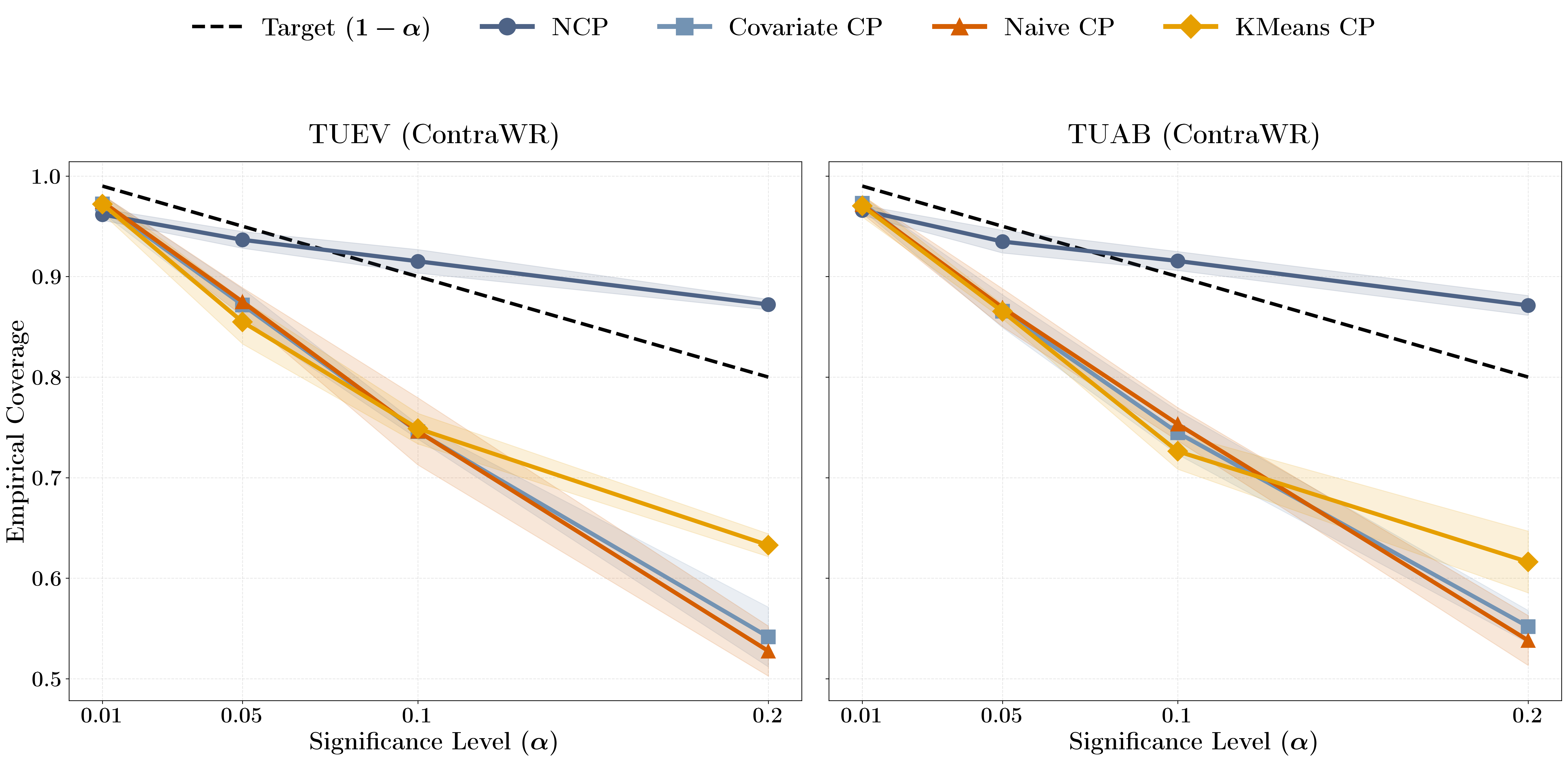
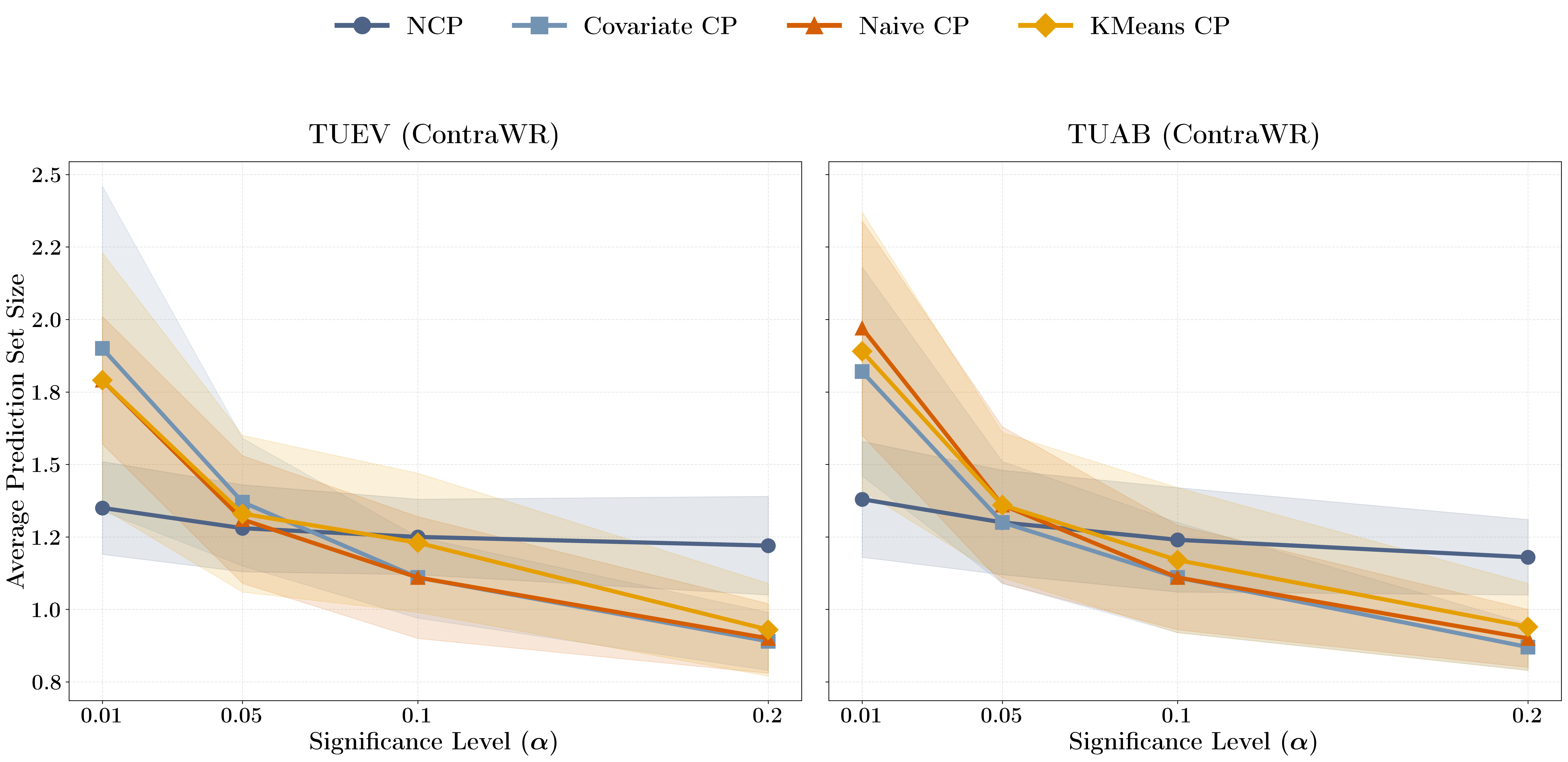
- Personalized methods worked better. NCP (the neighbor-based method) improved how often the true label was in the prediction set by more than 20 percentage points compared to the standard approach, while keeping the set sizes similar. That means you get better reliability without making the answer lists unhelpfully large.
- The “reweighting” method (Covariate CP) didn’t help much. Estimating what to reweight in high-dimensional EEG data proved hard and didn’t improve coverage here.
- NCP came closest to hitting the target coverage across many settings, especially when the allowed error was moderate (for example, aiming for 80–90% coverage). At extremely strict settings (like targeting 99% coverage), even NCP sometimes fell short—reminding us that no method is perfect yet in high-stakes, shifting healthcare data.
- The model’s answer lists stayed reasonably small. So, the method didn’t just say “I don’t know” and list everything—it stayed practical.
Why it matters: In clinical contexts, being honest about uncertainty can prevent overconfident mistakes. Giving a small, reliable set of possible diagnoses helps doctors use AI safely—especially when patients differ from those the AI saw before.
What’s the bigger impact?
- Safer AI in healthcare: Better uncertainty estimates make AI more trustworthy and easier to use in real hospitals, where patient populations and devices often vary.
- Personalization helps: Calibrating to similar patients (not everyone at once) is a promising path for robust predictions under real-world shifts.
- Open tools: The team released their code in the PyHealth framework, making it easier for others to try these methods on their own medical tasks.
- Future directions: Testing in other medical areas (like imaging or labs), using stronger EEG embeddings to find better “neighbors,” and pushing toward reliable performance even at very strict safety targets.
In short: The paper shows a practical way to make AI predictions more dependable in EEG tasks by personalizing uncertainty estimates—an important step toward safer, real-world healthcare AI.
Knowledge Gaps
Knowledge gaps, limitations, and open questions
Below is a concise list of what remains missing, uncertain, or unexplored in the paper, framed to guide actionable follow-up research.
- Generalizability beyond TUAB/TUEV: The study evaluates only two tasks from a single corpus; it remains unclear whether personalized CP maintains coverage across other EEG datasets, hospitals, devices, and broader healthcare modalities (e.g., ECG, imaging, clinical tabular data).
- Patient-level data splits and leakage: The paper uses “global” splits but does not confirm subject-wise disjointness; coverage claims may be confounded by shared patients or sessions across splits. Patient-wise and hospital-wise splits should be tested explicitly.
- Formal validity of NCP implementation: While NCP is argued to retain marginal validity under exchangeability, the paper does not provide finite-sample guarantees for the specific k-NN weighting scheme used nor quantify deviations when exchangeability is violated.
- Shift taxonomy and assumption checks: The covariate shift assumption () is not validated for EEG; the type and magnitude of shifts (covariate, label, concept, conditional) remain uncharacterized, limiting the interpretability of coverage results.
- Alternative density ratio estimation under shift: Covariate CP relies on KDE, which underperforms in high dimensions; modern ratio estimators (e.g., KLIEP/uLSIF, domain-classifier propensity weights, deep density-ratio models) were not evaluated.
- Hyperparameter sensitivity of personalized CP: The robustness of NCP/K-means CP to k, distance metrics, neighbor weighting kernels, cluster count, embedding normalization, and representation layer choice is not assessed.
- Dependence on feature extractor quality: Results use ContraWR; the extent to which NCP’s neighborhood quality (and coverage) depends on the chosen encoder versus stronger EEG foundation models is not systematically studied.
- Nonconformity score design: The paper uses ; alternatives (e.g., margins, calibrated logits, APS/RAPS for controlling set sizes) and class-conditional or label-conditional CP were not explored.
- Class-conditional and subgroup coverage: Only marginal coverage is reported; per-class, per-patient, device, demographic, and session-level coverage (and fairness) remain unquantified.
- Temporal dependence and exchangeability violations: EEG segments are temporally and patient-correlated; methods like blocked, grouped, or sequential conformal prediction were not used to address non-i.i.d. structures.
- Low-alpha regimes for safety-critical use: NCP fails to meet target coverage at ; strategies for achieving valid coverage at very low miscoverage (e.g., conservative calibration, jackknife+, ensembles, distributionally robust CP) remain open.
- Computational scalability and latency: Personalized methods require k-NN over large calibration sets; runtime, memory, and feasibility in real-time clinical workflows (including approximate nearest neighbors) are not evaluated.
- Calibration set size effects: The impact of calibration set size on NCP coverage, stability, and set size (especially in small-calibration or domain-shifted scenarios) is not characterized.
- OOD detection integration: The paper does not assess combining CP with OOD detectors to gate predictions or adapt set sizes when test points are far from the calibration distribution.
- Label noise-aware CP: Given annotator disagreement in EEG labels, methods that incorporate soft labels, consensus uncertainty, or robust CP to label noise were not investigated.
- Utility metrics beyond coverage and set size: Clinical decision utility (e.g., cost-weighted metrics, conditional accuracy given set size, rate of singleton sets), and calibration curves are missing.
- Structured and sequential outputs: CP for event-level detection, multi-label EEG patterns, or sequence-level structured outputs (rather than fixed segments) remains unexplored.
- Privacy and federated calibration: Personalized CP requires storing and querying calibration embeddings; privacy-preserving or federated conformal calibration strategies were not considered.
- Theory beyond covariate shift: The provided decomposition does not cover conditional shift or patient-cluster shift; distributionally robust bounds and finite-sample guarantees under broader shift models are an open direction.
- Statistical significance and uncertainty reporting: Improvements (e.g., “25% greater coverage”) are shown without confidence intervals or formal hypothesis testing across seeds.
- Reproducibility details: Preprocessing steps, montage/channel handling, normalization, split stratification (by patient/session/class), and hyperparameters for CP methods are insufficiently specified for exact replication.
- Cross-device and montage variability: Robustness to differences in EEG channel configurations, sampling rates, and acquisition hardware is not evaluated.
- Interaction with improved predictors: The paper does not analyze how advances in representation learning (e.g., domain generalization, self-supervised pretraining) affect CP coverage and set sizes under shift.
Practical Applications
Immediate Applications
The following applications can be deployed now using the paper’s methods, code (PyHealth), and empirical insights, assuming appropriate validation and governance in each setting.
- EEG model uncertainty quantification and reporting (Healthcare, Software)
- What it enables: Wrap existing EEG classifiers with neighborhood conformal prediction (NCP) to output prediction sets instead of single labels, yielding better-calibrated uncertainty under patient distribution shift.
- Tools/workflows: PyHealth NCP module; post-hoc calibration pipeline; reporting of coverage and set-size distributions.
- Assumptions/dependencies: Sufficient calibration data from the target population; representation quality (ContraWR or comparable embeddings) so “neighborhoods” reflect clinically meaningful similarity; compute for kNN/ANN search.
- Reader triage in EEG labs (Healthcare operations)
- What it enables: Route “high-uncertainty” segments (large prediction sets) to senior readers or consensus review; auto-pass clear singleton-set cases for faster throughput.
- Tools/workflows: Integration with EEG review software and PACS-like workflow; dashboard highlighting segments by set size; configurable α to match service-level targets.
- Assumptions/dependencies: Human-in-the-loop workflow; institutional QA; acceptance of set-based outputs by clinicians; monitoring to ensure no degradation for rare, high-risk events.
- Model validation and auditing with coverage metrics (Healthcare, Academia, MLOps)
- What it enables: Evaluate empirical coverage and set-size distributions overall and across subgroups (site, device, demographics) to identify under-covered regions before deployment.
- Tools/workflows: “Coverage cards” in model review; subgroup stratified evaluation; CI pipelines that fail builds when coverage drops below thresholds.
- Assumptions/dependencies: Representative calibration/holdout cohorts; governance to act on audit findings; clarity on acceptable α for use-case risk.
- Data curation and active learning (Healthcare, Academia)
- What it enables: Prioritize relabeling or adjudication for segments with large prediction sets; focus labeling budgets on uncertain regions to reduce label noise.
- Tools/workflows: Queue management for annotation; “uncertainty-driven” sampling; periodic recalibration after relabeling.
- Assumptions/dependencies: Access to annotators; processes to reconcile disagreements; stable data ingestion.
- Rapid replication and benchmarking (Academia)
- What it enables: Reproduce the study on TUAB/TUEV; benchmark new embeddings/foundation models for calibration quality under shift using the provided NCP baseline.
- Tools/workflows: PyHealth pipelines; shared scripts/configs; standardized metrics (coverage at multiple α, average set size).
- Assumptions/dependencies: Access to datasets; compute; careful seed/partition control to compare fairly.
- Calibration-as-a-service microservice (Software, Healthcare IT)
- What it enables: A lightweight API that takes model scores and returns conformal prediction sets using NCP for any classifier.
- Tools/workflows: Containerized service; FAISS/ScaNN indexes for fast neighbor lookup; monitoring endpoints for empirical coverage.
- Assumptions/dependencies: Secure data flow; latency budgets; PII/privacy compliance.
- Internal policy updates for model evaluation checklists (Policy, Health systems)
- What it enables: Require reporting of conformal coverage and set-size statistics across subgroups in internal model review gates.
- Tools/workflows: Add uncertainty KPIs to existing AI governance frameworks; dashboards for coverage drift over time.
- Assumptions/dependencies: Organizational buy-in; threshold-setting aligned with clinical risk; trained reviewers.
- Extension to other biosignals with minimal adaptation (Healthcare, Software)
- What it enables: Apply NCP to ECG arrhythmia, sleep staging, EMG, ICU waveform alarms where patient/device shift is common.
- Tools/workflows: Swap in task-specific embeddings; reuse NCP calibration; compare against naive and covariate-weighted CP.
- Assumptions/dependencies: Reasonable embeddings for neighborhood quality; calibration data from deployment domain; task-specific validation.
Long-Term Applications
These applications require further research, embedding advances, scaling, human-factors work, or regulatory studies.
- Real-time, patient-personalized seizure monitoring with uncertainty-aware triage (Healthcare, Medical devices)
- What it enables: Continuous EEG monitoring that escalates only high-confidence seizures, defers ambiguous cases, and communicates uncertainty to bedside staff.
- Tools/workflows: Streaming NCP with low-latency ANN; alert management tuned to α; EHR/monitor integration.
- Assumptions/dependencies: Prospective trials; UI/UX for set-based outputs; robust performance at very low α (e.g., 0.01).
- Regulatory-grade uncertainty guarantees (Policy, Healthcare)
- What it enables: Standards requiring uncertainty reporting (coverage, set sizes, subgroup stability) in SaMD submissions and post-market surveillance.
- Tools/workflows: Harmonized metrics and protocols; external validation; ongoing coverage monitoring as real-world evidence.
- Assumptions/dependencies: Engagement with regulators; consensus on acceptable α by indication; evidence that NCP meets guarantees at clinical risk levels.
- Foundation-model–enhanced calibration (Healthcare AI, Software)
- What it enables: Use stronger EEG foundation embeddings (e.g., time–frequency motif models) to improve neighborhood quality, reducing set sizes while achieving target coverage.
- Tools/workflows: Pretraining pipelines; plug-and-play encoders in NCP; transfer learning across sites.
- Assumptions/dependencies: Availability of large, diverse pretraining corpora; evaluation across devices/sites; compute.
- Dynamic online calibration under nonstationarity (Healthcare, MLOps)
- What it enables: Continual recalibration as devices, protocols, and populations drift; hybrid neighborhood + importance weighting without brittle density estimation.
- Tools/workflows: Drift detection; sliding-window calibration; adaptive k and neighborhood radius selection; safe rollback.
- Assumptions/dependencies: Streaming metrics; resource budgets; safeguards against catastrophic undercoverage.
- Fairness-aware conformal prediction (Policy, Healthcare)
- What it enables: Uniform conditional coverage across demographics, sites, and devices; auditing and mitigation when some subgroups are under-covered.
- Tools/workflows: Subgroup-aware NCP; reweighting or neighborhood constraints; fairness dashboards.
- Assumptions/dependencies: Access to sensitive attributes (or robust proxies); legal/ethical approvals; sample size per subgroup.
- Multimodal decision support with set-based outputs (Healthcare)
- What it enables: Combine EEG, imaging, labs with CP to provide calibrated, set-based differential diagnoses, highlighting plausible alternatives and next steps.
- Tools/workflows: Late-fusion predictors; modality-specific NCP; clinician-facing explanations linked to each candidate label.
- Assumptions/dependencies: Interoperability across data streams; human-factors validation; calibration across modalities.
- Coverage-driven active learning and label QA at scale (Academia, Healthcare)
- What it enables: Systematic reduction of label noise by targeting high-uncertainty segments for consensus review; measurable gains in downstream coverage.
- Tools/workflows: Consensus workflows; budget-optimized selection; periodic recalibration loops.
- Assumptions/dependencies: Sustained annotation capacity; reproducible labeling guidelines; governance for adjudication.
- Privacy-preserving neighborhood calibration (Software, Privacy tech)
- What it enables: Hospital-to-hospital calibration using federated or DP-aware approximate neighbor search without sharing raw data.
- Tools/workflows: Federated indices; secure kNN; differential privacy accounting.
- Assumptions/dependencies: Infrastructure and legal frameworks for cross-institution collaboration; acceptable utility–privacy tradeoffs.
- Cross-sector adaptation to high-shift domains (Finance, Energy, Robotics, Education)
- What it enables: In finance, set-based risk forecasts under regime shifts; in energy, uncertainty-bounded load forecasts; in robotics, safety gating when ambiguity is high; in education, robust grading assistance with ambiguity flags.
- Tools/workflows: Domain-specific embeddings; NCP calibration on in-domain data; dashboards for set-size–based escalation.
- Assumptions/dependencies: Quality embeddings capturing domain similarity; adequate calibration data; governance for set-based decisions.
- Human-centric interfaces for uncertainty (Healthcare, Consumer health)
- What it enables: Patient-/clinician-facing UIs that present prediction sets clearly (e.g., top-2 labels with rationale), improving trust and decision quality in wearables (sleep staging, home EEG) and portals.
- Tools/workflows: UX studies; iconography and explanations for set outputs; configurable α by use case (wellness vs clinical).
- Assumptions/dependencies: Evidence that set-based displays improve outcomes; risk communication best practices; accessibility and localization.
Notes on overarching assumptions and dependencies:
- Empirical gains were shown on TUAB/TUEV EEG tasks using ContraWR; external validation is needed for other datasets, devices, and tasks.
- Theoretical benefits assume covariate shift (stable P(Y|X)) and neighborhoods that approximate conditional calibration; severe label shift or concept drift may violate assumptions.
- Kernel-density–based covariate weighting performed poorly here; successful weighting likely requires better density-ratio estimation or representation learning.
- Coverage at very low α (e.g., 0.01) remains challenging; safety-critical deployments require further advances, prospective studies, and robust monitoring.
Glossary
- Absolute continuity: A property where one probability distribution assigns zero probability to any event that another distribution also deems impossible (here, test is absolutely continuous w.r.t. calibration). Example: "Assume absolute continuity $P_{\mathrm{test}\ll P_{\mathrm{cal}$"
- Artifacts (ARTF): Non-neural signals or noise in EEG recordings that can confound analysis (e.g., muscle movement, electrode issues). Example: "artifacts (ARTF)"
- Background activity (BCKG): Baseline EEG patterns representing normal ongoing brain activity. Example: "background activity (BCKG)"
- Calibration set: A held-out dataset used to compute conformity/nonconformity scores for determining prediction set thresholds. Example: "the data are partitioned into a training set (used to fit a predictor) and a calibration set (used only to compute nonconformity scores)."
- Cauchy–Schwarz inequality: A fundamental inequality in inner-product spaces used here to bound coverage error via variances. Example: "by Cauchy--Schwarz:"
- Conditional coverage function: The probability that a prediction set contains the true label, conditioned on features X. Example: "define its conditional coverage function and local slack under $P_{\mathrm{cal}$ as"
- Conditional guarantee: A per-instance reliability guarantee (for a given X), contrasted with marginal (average) guarantees. Example: "rather than a conditional guarantee for each individual ."
- Conformal prediction: A distribution-free method that outputs prediction sets with guaranteed coverage under exchangeability. Example: "Conformal prediction (CP) is a distribution-free framework for constructing prediction sets (or intervals) that quantify uncertainty..."
- ContraWR: A CNN-based EEG representation learning architecture used as the base classifier in experiments. Example: "We utilize ContraWR\cite{yang2023selfsupervisedeegrepresentationlearning_contrawr} for our problem."
- Covariate CP: A conformal approach that adjusts for covariate shift by weighting conformity scores using estimated likelihood ratios. Example: "Covariate CP \cite{tibshirani2020conformalpredictioncovariateshift} addresses covariate shift between calibration and test sets by weighting each conformity score with a likelihood ratio."
- Covariate shift: A setting where the feature distribution changes between domains while the conditional label distribution given features remains the same. Example: "Formally, covariate shift assumes"
- Covariate-shift decomposition: A decomposition of test-domain coverage error into terms involving shift magnitude and variability of local slack. Example: "via a covariate-shift decomposition of the test-domain coverage error"
- Coverage error: The deviation of empirical or test-domain coverage from the target coverage level (1−α). Example: "Coverage error decomposition under covariate shift"
- Density ratio: The ratio of test to calibration feature densities, used for importance weighting under covariate shift. Example: "density ratio $w(x)=p_{\mathrm{test}(x)/p_{\mathrm{cal}(x)$"
- EEG (Electroencephalography): A technique for recording electrical activity of the brain, used here for seizure/event classification. Example: "EEG classification is typically framed as supervised classification (binary or multiclass) over fixed-length segments."
- Eye movements (EYEM): EEG event class indicating ocular movement-related patterns. Example: "eye movements (EYEM)"
- Exchangeability: A statistical assumption akin to i.i.d. that allows conformal prediction guarantees, requiring the joint distribution be invariant to permutations. Example: "assuming exchangeability of the calibration and test examples (e.g., i.i.d.\ data)"
- Generalized periodic epileptiform discharges (GPED): A pathologic EEG pattern characterized by generalized periodic epileptiform activity. Example: "generalized periodic epileptiform discharges (GPED)"
- Importance weights: Weights proportional to the density ratio used to reweight calibration examples to reflect test distribution under covariate shift. Example: "weighted conformal prediction with importance weights proportional to the density ratio"
- i.i.d. (independent and identically distributed): A data assumption where samples are independent draws from the same distribution. Example: "i.i.d. assumptions underlying standard conformal methods"
- K-means CP: A personalized conformal method that calibrates within the nearest cluster rather than globally. Example: "K-means CP takes a naive approach to personalized conformal prediction by deriving each test sample's conformal threshold from only the calibration samples in its nearest cluster"
- k-nearest neighbors (k-NN): A neighborhood selection method to find nearby calibration points in representation space for local calibration. Example: "via -nearest neighbors in -space"
- Kernel density estimation: A nonparametric technique for estimating probability densities, used here to estimate likelihood ratios for covariate shift. Example: "this weight adjustment is estimated through kernel density estimation"
- Local calibration slack: The difference between local conditional coverage and the target level (1−α), capturing over/under-coverage at a point. Example: "and the local calibration slack"
- Marginal coverage guarantee: An average (over the data distribution) coverage guarantee that the true label lies in the prediction set with probability at least 1−α. Example: "such that the marginal coverage guarantee holds:"
- Marginal validity: The property that the conformal method achieves its nominal marginal coverage on the calibration distribution. Example: "Under (approximate) marginal validity on the calibration distribution"
- Neighborhood conformal prediction (NCP): A conformal method that adapts calibration locally using nearby examples in representation space to improve local reliability. Example: "Neighborhood conformal prediction (NCP) addresses this issue by localizing calibration to a patient's neighborhood in representation space"
- Nonconformity score: A measure of how atypical a candidate label is for an input, used to construct conformal prediction sets. Example: "Given a nonconformity score (a measure of how ``atypical'' a candidate label is for an input)"
- Penultimate-layer embedding: The feature vector from the layer just before the output layer of a neural network, used as a representation for neighborhood search. Example: "the penultimate-layer embedding of a deep network"
- Periodic lateralized epileptiform discharges (PLED): An EEG pattern of lateralized, periodic epileptiform activity associated with focal pathology. Example: "periodic lateralized epileptiform discharges (PLED)"
- Prediction set: A set of labels output by conformal prediction that is guaranteed to contain the true label with prescribed probability. Example: "CP outputs a prediction set "
- Representation space: The feature space induced by an embedding function (e.g., a neural network), used to define neighborhoods for local calibration. Example: "a patient's neighborhood in representation space"
- ResNet: A deep convolutional neural network architecture with residual connections, used here within the EEG classifier. Example: "a ResNet-based 2D CNN"
- Spike-and-sharp waves (SPSW): Epileptiform EEG discharges characterized by spikes and sharp waves. Example: "spike-and-sharp waves (SPSW)"
- Spectrogram: A time-frequency representation of signals used as input to CNNs for EEG processing. Example: "converts biosignals into multi-channel spectrogram representations"
- Split conformal prediction: A practical CP variant that splits data into training and calibration sets to compute a global threshold. Example: "we often instantiate CP via split conformal prediction"
- Temple University Hospital EEG Corpus (TUH EEG Corpus): A large, publicly available EEG dataset from TUH used for benchmarking. Example: "TUH EEG Corpus\cite{obeid2016temple_tuh_eeg_corpus}"
- TUAB: A TUH-derived dataset for abnormal EEG detection (binary classification). Example: "TUAB is designed for abnormal EEG detection"
- TUEV: A TUH-derived dataset for EEG event classification (multiclass). Example: "The TUEV dataset targets EEG event classification"
- Weighted conformal prediction: A CP variant that reweights calibration scores to correct for covariate shift between calibration and test distributions. Example: "A principled correction is to use weighted conformal prediction with importance weights proportional to the density ratio"
- Weighted empirical distribution: An empirical distribution where observations are assigned weights, used to compute local quantiles in NCP. Example: "constructs a weighted empirical distribution over calibration scores"
Collections
Sign up for free to add this paper to one or more collections.