- The paper introduces a novel pipeline that integrates EKF-based needle pose estimation to significantly improve autonomous suturing accuracy.
- It utilizes stereo imaging with RAFT-Stereo and SAM for precise 3D suture alignment, ensuring uniform wound closure without manual input.
- Experimental evaluations demonstrate a 66% increase in suture count and a 38% reduction in time, underscoring its clinical potential.
STITCH 2.0: Augmented Dexterity for Autonomous Surgical Suturing
Introduction and Motivation
STITCH 2.0 presents a comprehensive pipeline for autonomous surgical suturing using the da Vinci Research Kit (dVRK), addressing critical limitations in prior work (STITCH 1.0) related to needle pose estimation, thread management, and suture alignment. The system is designed within the paradigm of "Augmented Dexterity," where robots automate well-defined surgical subtasks under human supervision, aiming to improve consistency and reduce surgeon fatigue. The pipeline integrates seven key improvements, including an Extended Kalman Filter (EKF) for needle pose estimation, adaptive pointcloud filtering, automated 3D suture alignment, and robust thread management strategies.
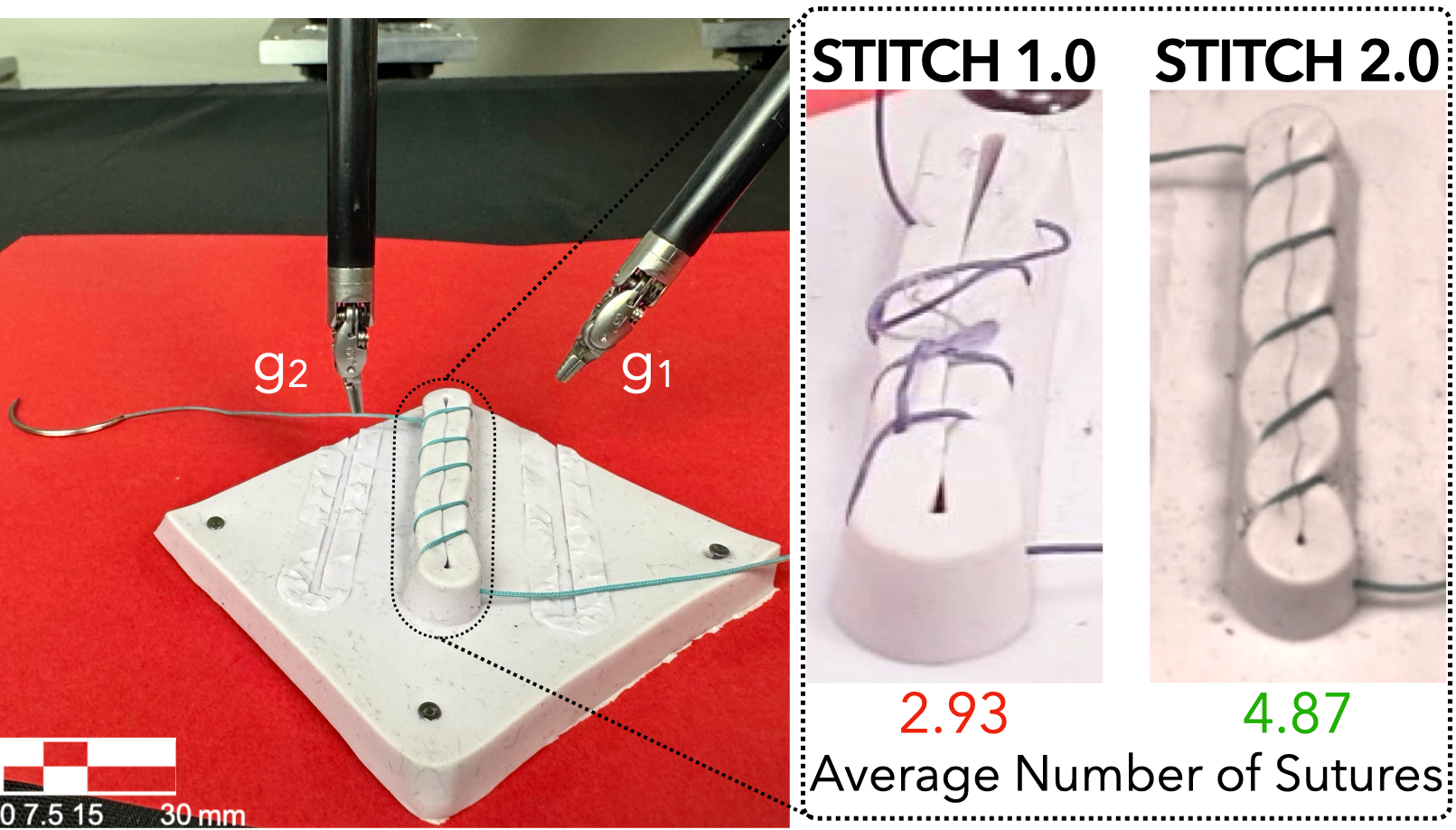
Figure 1: The da Vinci Research Kit equipped with two grippers g1 and g2; STITCH 2.0 achieves tighter, more uniform sutures compared to STITCH 1.0.
System Architecture
STITCH 2.0 is structured into three primary phases: 3D Suture Alignment, 6D Needle Pose Estimation with EKF, and the Augmented Dexterity Controller.
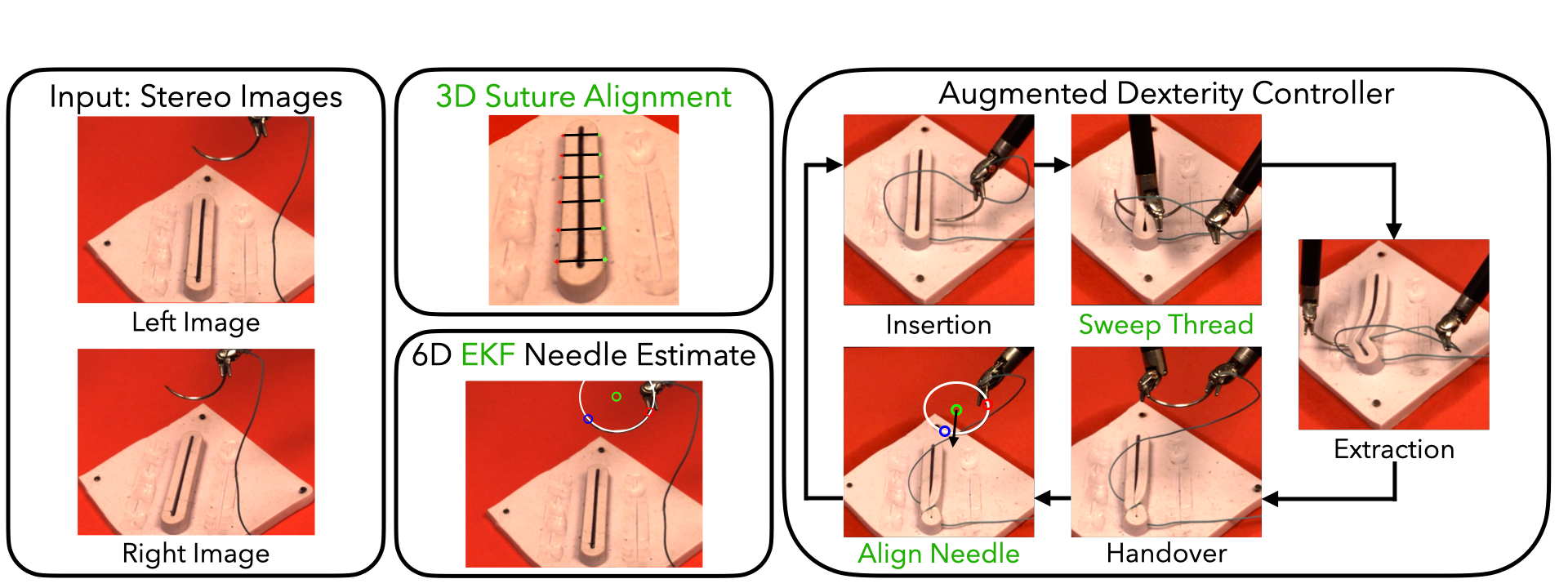
Figure 2: Overview of the STITCH 2.0 pipeline, highlighting new modules for suture alignment, EKF-based needle pose estimation, and dexterity control.
3D Suture Alignment
The pipeline begins by autonomously determining optimal suture insertion and extraction points using stereo imaging and pointcloud analysis. RAFT-Stereo generates a dense scene pointcloud, and Segment Anything (SAM) segments the wound and phantom surfaces. RANSAC is used to fit planes and extract wound geometry, enabling the system to evenly distribute suture positions along the wound centerline. This eliminates the need for manual input and ensures uniform suture spacing, which is critical for optimal wound healing.
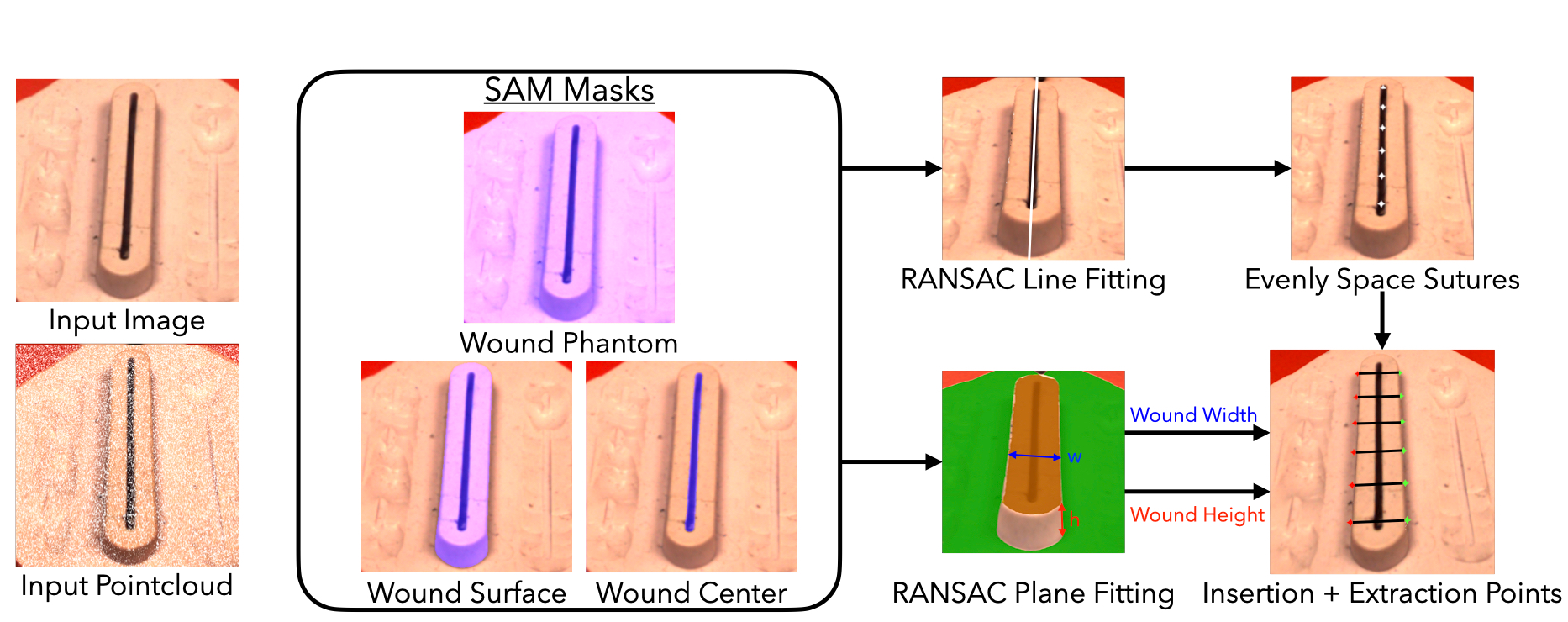
Figure 3: Automated 3D suture alignment using stereo pointclouds and segmentation to determine insertion/extraction points.
6D Needle Pose Estimation with EKF
Needle pose estimation is performed using a U-Net trained on UV-illuminated needle images for robust segmentation. Flood-filling is applied to reduce specular noise, and skeletonization (Zhang's method) further refines the mask for efficient and accurate pointcloud extraction. RANSAC is used for plane and circle fitting, yielding the needle's center, endpoints, and normal vector. The EKF is instantiated before each needle interaction, leveraging stationary needle states for high-confidence pose estimates. The EKF state vector is 13-dimensional, encompassing all geometric parameters required for precise manipulation.
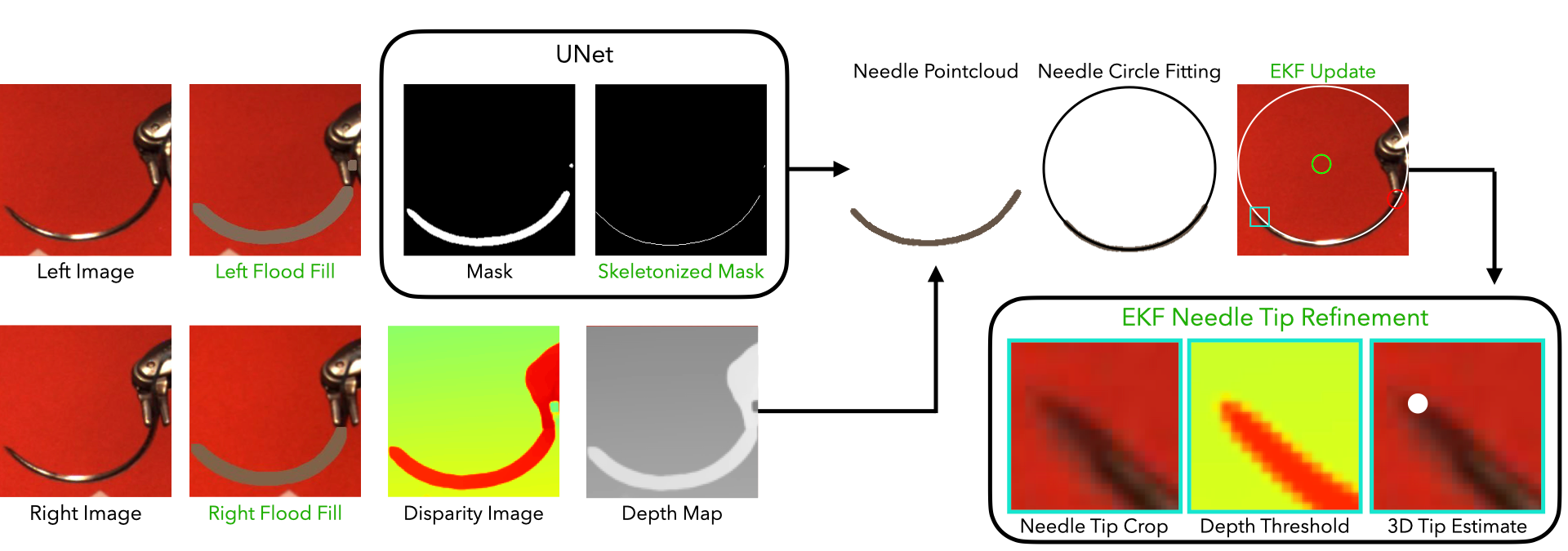
Figure 4: EKF-based needle pose estimation pipeline, integrating U-Net segmentation, flood-filling, stereo disparity, and skeletonization for robust 3D circle fitting.
Augmented Dexterity Controller
The controller orchestrates five subtasks: needle insertion, thread sweeping, needle extraction with cinching, needle alignment and handover, and pre-insertion alignment. Each subtask is informed by perception modules and calibrated kinematics (RNN-based). Thread management is a major innovation, with coordinated gripper trajectories to prevent tangling and cross-stitching, a common failure in prior systems.
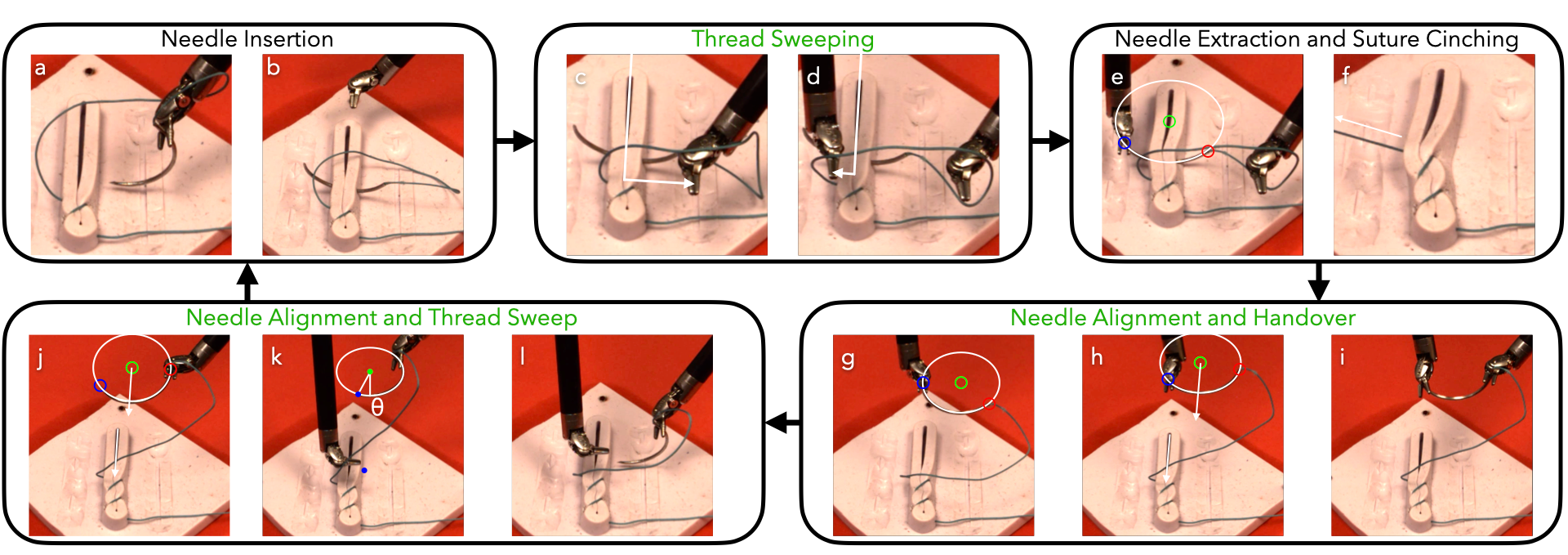
Figure 5: Augmented Dexterity Controller workflow, detailing the sequence of needle and thread manipulations for each suture cycle.
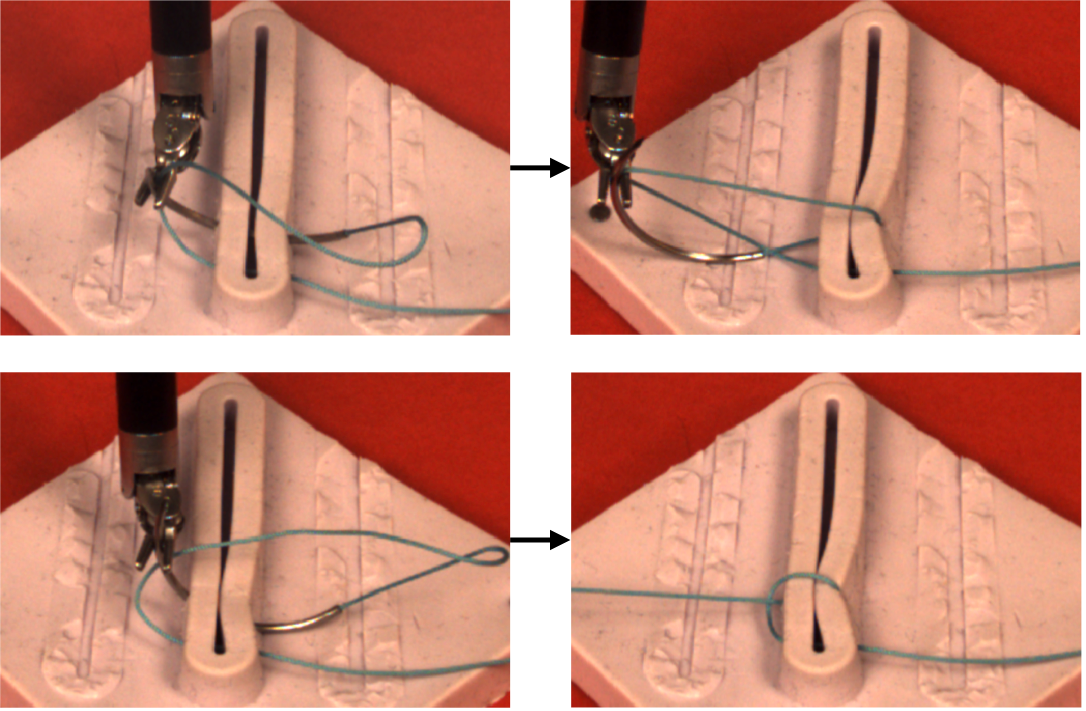
Figure 6: Examples of thread tangling and cross-stitching failures addressed by STITCH 2.0's thread management strategies.
Experimental Evaluation
STITCH 2.0 was evaluated on 15 trials of 6 consecutive sutures each, using a dVRK and a standardized wound phantom. Metrics include number of successful sutures, wound gap closure rate, mean time per suture, and needle pose estimation accuracy. Four error types were tracked: alignment, thread management, insertion, and missed grasp.
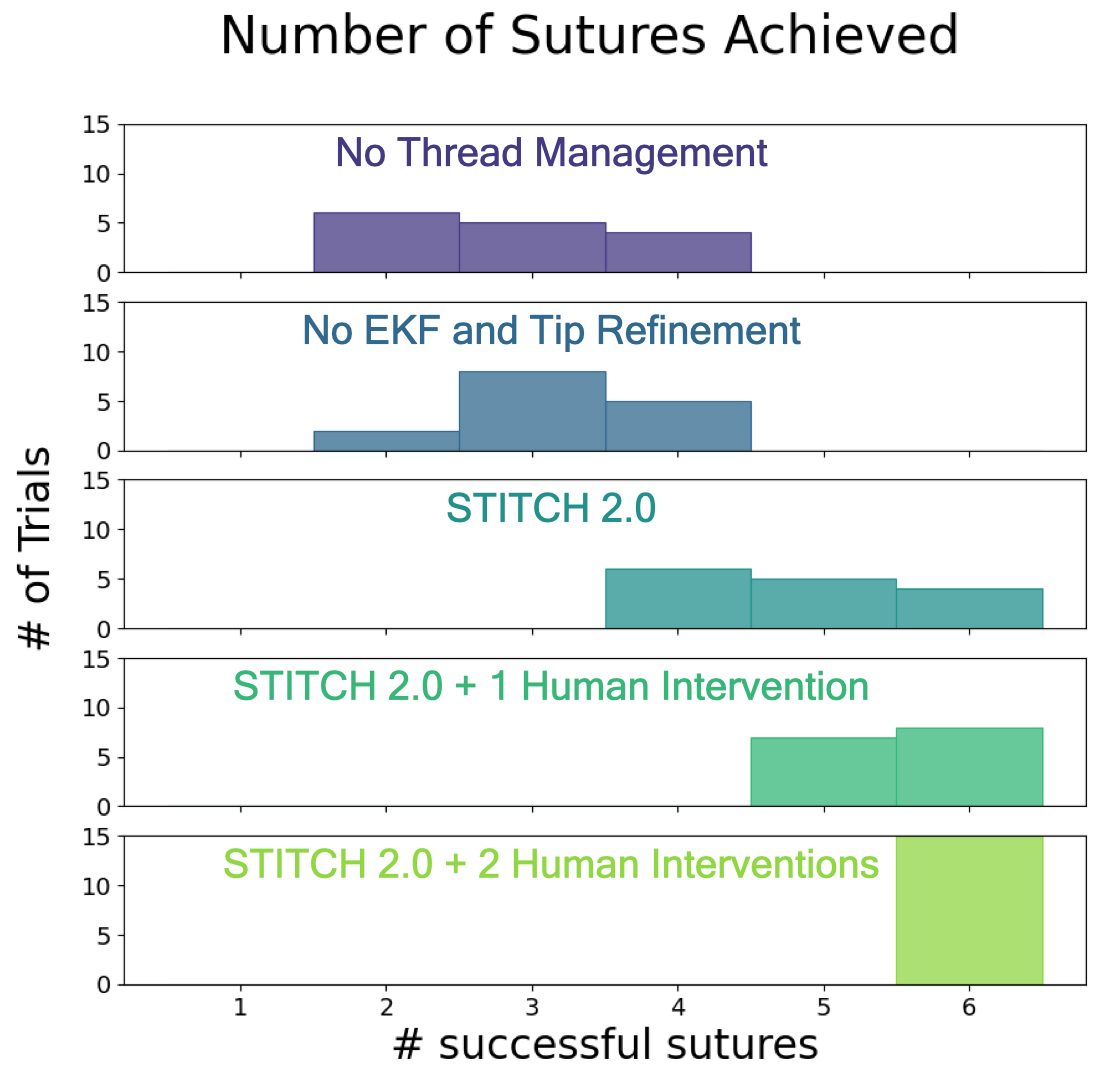
Figure 7: Histogram of sutures achieved per method across 450 trials, demonstrating STITCH 2.0's superior performance.
STITCH 2.0 achieved an average of 4.87 sutures per trial (86.9% single-suture success, 74.4% wound closure), representing a 66% increase in suture count and 38% reduction in time compared to STITCH 1.0. With up to two human interventions, STITCH 2.0 consistently achieved 6 sutures and 100% wound closure. Ablation studies confirmed the necessity of both EKF-based pose estimation and thread management, with each component contributing significant improvements in reliability and suture quality.
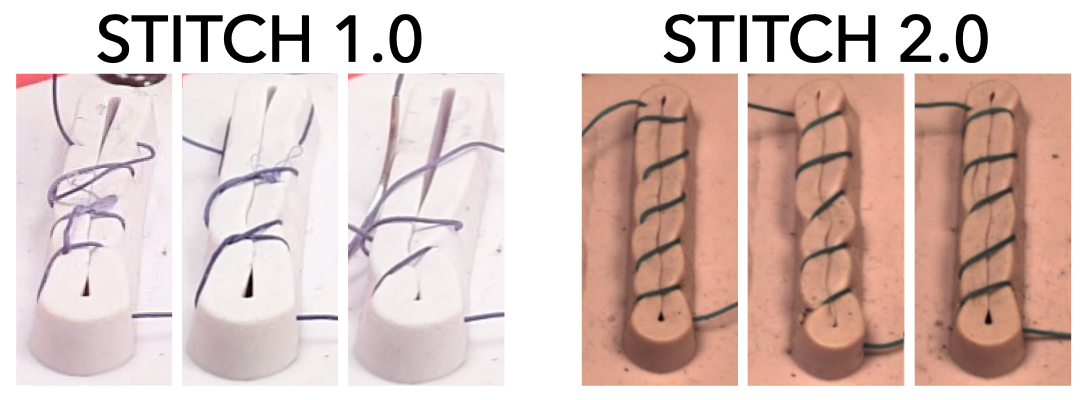
Figure 8: Qualitative comparison of suture outcomes; STITCH 2.0 produces uniform, tight sutures versus the messy, incomplete closure of STITCH 1.0.
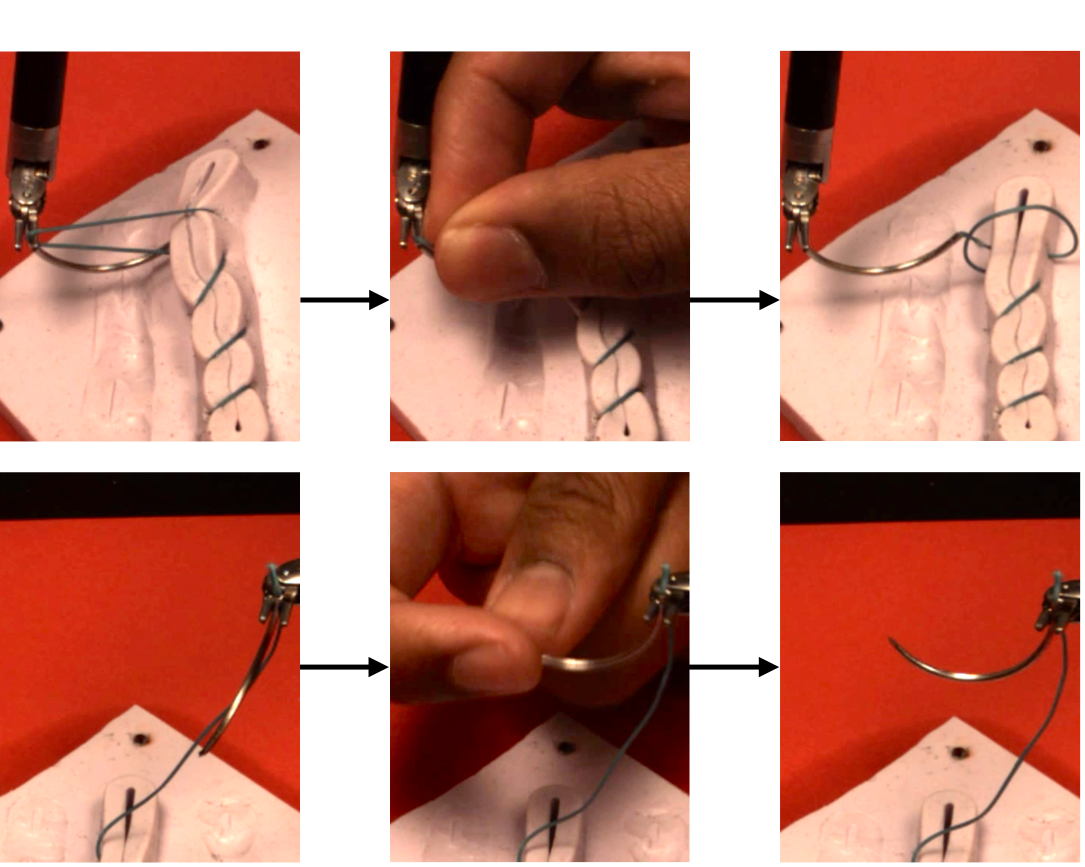
Figure 9: Examples of human interventions: thread removal from gripper and needle orientation correction.
Needle pose estimation accuracy reached 97.56% with EKF, compared to 85.98% without EKF and 42% for STITCH 1.0. Failure cases were primarily associated with needle orientations that occluded endpoints or deviated from the camera plane.
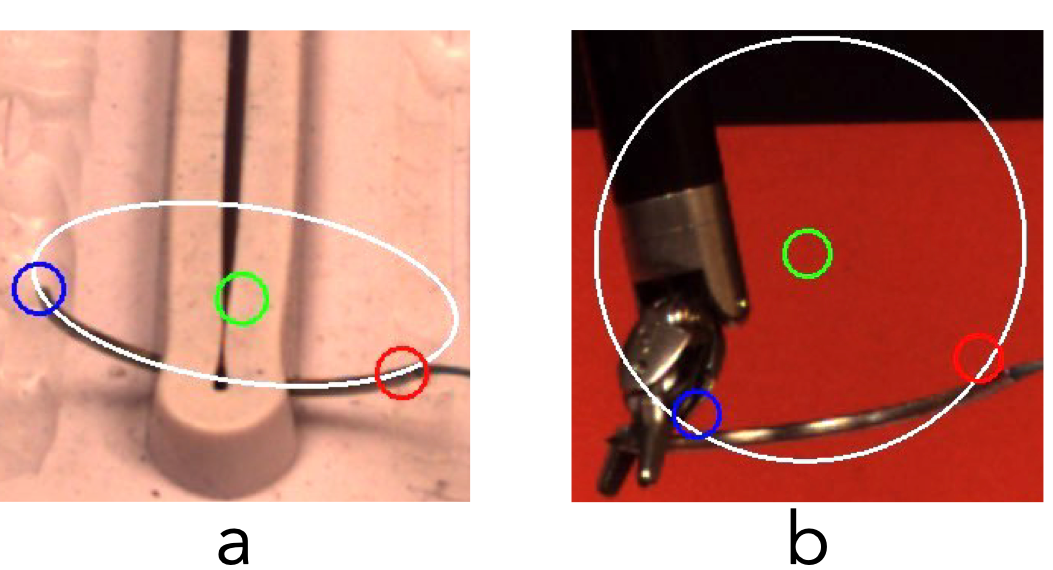
Figure 10: Needle pose estimate success and failure; endpoint errors are most pronounced when the needle is oriented away from the camera.
Limitations and Future Directions
Three primary limitations remain: (1) sub-millimeter gripper inaccuracies during insertion, (2) slow needle pose estimation (1 Hz), and (3) limited generalization to ex-vivo and clinical settings due to reliance on external stereo cameras and simplified wound geometry. Future work should focus on improved kinematic calibration, accelerated stereo reconstruction (potentially via region-of-interest cropping or integration with monocular keypoint methods), and adaptation to endoscopic imaging and complex wound topologies.
Conclusion
STITCH 2.0 demonstrates a robust, modular approach to autonomous surgical suturing, integrating advanced perception, state estimation, and dexterous control. The system achieves substantial improvements in suture quality, reliability, and efficiency over previous baselines, validated through extensive physical experiments and ablation studies. The pipeline's modularity and reliance on standard surgical hardware position it as a promising candidate for future clinical translation, contingent on further improvements in speed, generalization, and integration with endoscopic imaging modalities.