Physics-informed neural networks to learn cardiac fiber orientation from multiple electroanatomical maps
Published 28 Jan 2022 in eess.IV, cs.LG, physics.med-ph, and q-bio.TO | (2201.12362v3)
Abstract: We propose FiberNet, a method to estimate \emph{in-vivo} the cardiac fiber architecture of the human atria from multiple catheter recordings of the electrical activation. Cardiac fibers play a central role in the electro-mechanical function of the heart, yet they are difficult to determine in-vivo, and hence rarely truly patient-specific in existing cardiac models. FiberNet learns the fiber arrangement by solving an inverse problem with physics-informed neural networks. The inverse problem amounts to identifying the conduction velocity tensor of a cardiac propagation model from a set of sparse activation maps. The use of multiple maps enables the simultaneous identification of all the components of the conduction velocity tensor, including the local fiber angle. We extensively test FiberNet on synthetic 2-D and 3-D examples, diffusion tensor fibers, and a patient-specific case. We show that 3 maps are sufficient to accurately capture the fibers, also in the presence of noise. With fewer maps, the role of regularization becomes prominent. Moreover, we show that the fitted model can robustly reproduce unseen activation maps. We envision that FiberNet will help the creation of patient-specific models for personalized medicine. The full code is available at http://github.com/fsahli/FiberNet.
The paper introduces FiberNet, a PINN framework that infers patient-specific cardiac fiber orientation from multiple sparse activation maps.
The method leverages the anisotropic eikonal equation and a composite loss function—combining data fidelity, physics constraints, and regularization—to reconstruct conduction velocity tensors.
Robust performance on synthetic, DT-MRI atlas, and in-vivo patient data highlights its potential for digital twin applications and improved clinical planning.
Physics-Informed Neural Networks for Inferring Cardiac Fiber Orientation from Electroanatomical Maps
Introduction
The precise, in-vivo characterization of cardiac fiber orientations, especially in the atria, remains a challenge in computational cardiology. Fiber direction critically determines cardiac electrophysiological anisotropy and underlies predictive accuracy in digital twinning and personalized simulation of cardiac activation and arrhythmogenesis. The presented work introduces FiberNet, a novel framework based on physics-informed neural networks (PINNs), designed to infer spatially resolved, patient-specific cardiac fiber fields from multiple sparse electroanatomical activation maps, thus providing a means to estimate local conduction velocity tensors from minimally invasive measurements and enabling predictive cardiac modeling without relying on ex-vivo imaging or generalized atlas priors.
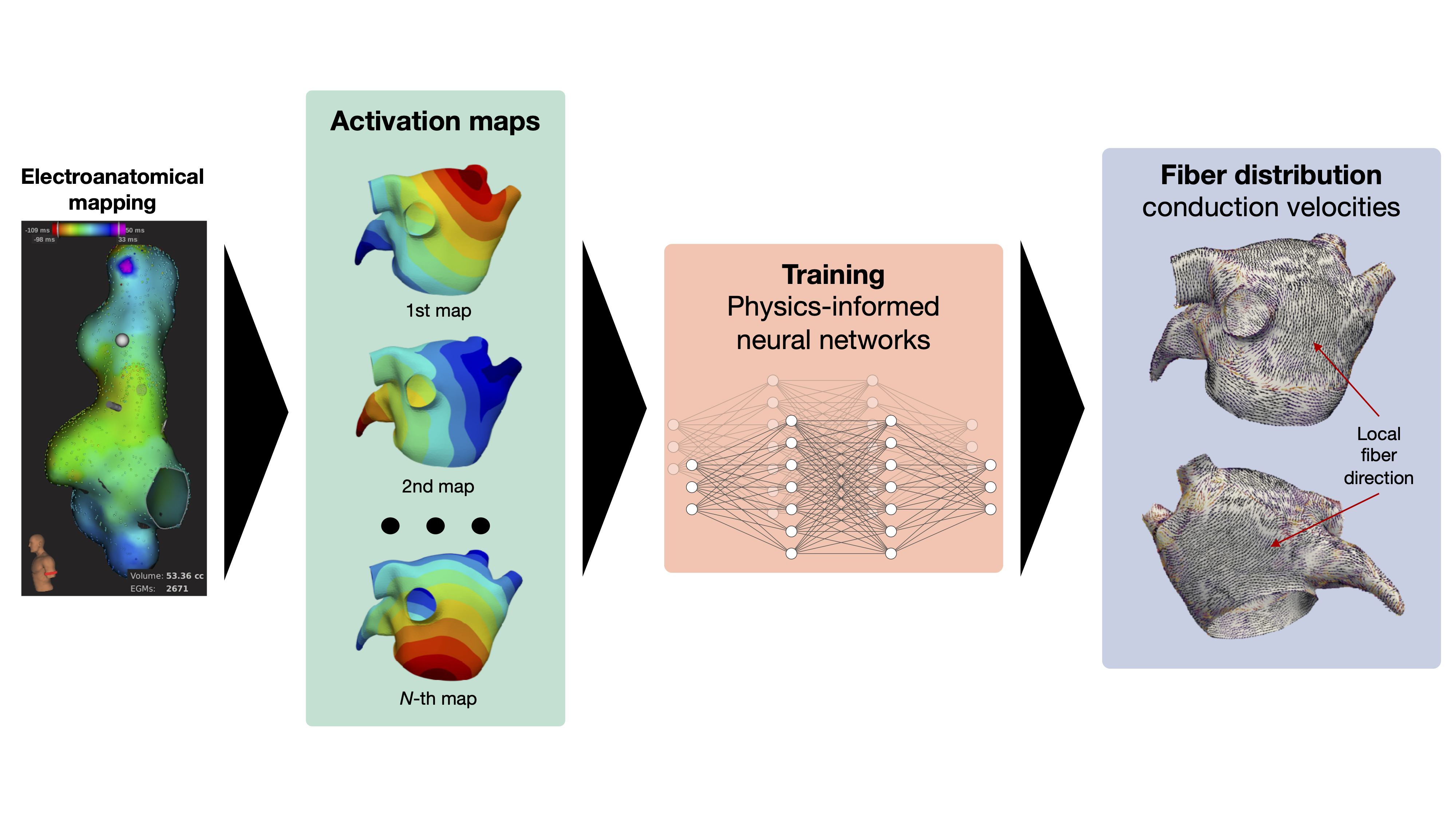
Figure 1: FiberNet translates a set of electroanatomical maps into a continuous estimate of the fiber field and conduction velocity. These estimates can be used for simulating cardiac activation in a predictive model based on the eikonal equation. Internally, FiberNet uses physics-informed neural networks to constrain the parameter space during the training phase.
Methodological Framework
Mathematical Modeling of Electrophysiological Propagation
Cardiac activation is modeled by the anisotropic eikonal equation:
D(x)∇ϕ(x)⋅∇ϕ(x)=1,
where D is the spatially varying conduction tensor, encoding both the anisotropy ratio and fiber orientation, and ϕ is the activation time. Fiber direction l(x) is the dominant eigenvector of D(x).
Physics-Informed Neural Networks for Inverse Problem
FiberNet parameterizes both D and the set of activation maps {ϕm}m=1M as feedforward neural networks sharing the same spatial input, leading to a mesh-free parameterization enabling continuous field reconstruction over arbitrarily shaped atrial manifolds.
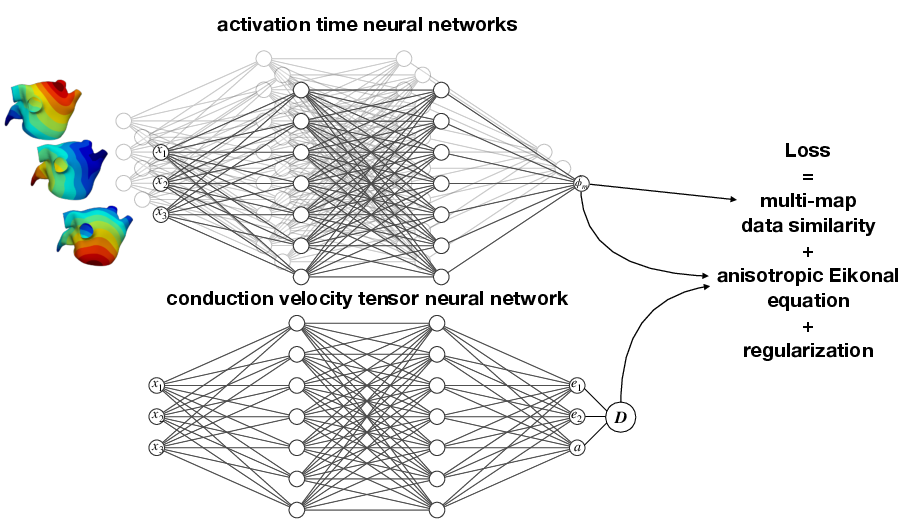
Figure 2: Schematic representation of the PINN ensemble—activation maps and the conduction velocity tensor are represented via neural networks, with loss components enforcing both data fidelity and satisfaction of the eikonal PDE constraint.
The loss function comprises:
Data loss: squared error between predicted and measured activation times at observation points.
Physics loss: eikonal PDE residual at collocation points, enforcing local physical consistency.
Regularization: Huber-norm-based total variation penalties to favor physiologically plausible smoothness in both fiber angle and conduction velocities.
Identifiability and Well-Posedness Analysis
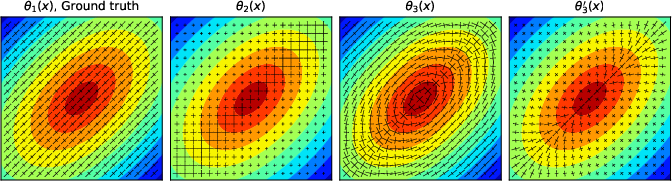
The inverse problem of reconstructing D(x) from activation maps is ill-posed for a single map, as different tensors can generate the same activation wavefront geometry—only the velocity in the direction of propagation is constrained. The work systematically demonstrates, through constructive counterexamples and visualization, that at least three non-parallel activation maps are required for unique local identification of the conduction tensor’s eigenstructure, unless sufficient regularization or specific priors are imposed.
Figure 3: Multiple conductivity tensors reproducing the same activation map. The solution with lowest Huber norm, θ1(x), matches the ground truth, but alternative solutions can exist without unique identifiability from single-map data.
Numerical Experiments and Performance Evaluation
Synthetic 2D and 3D Geometries
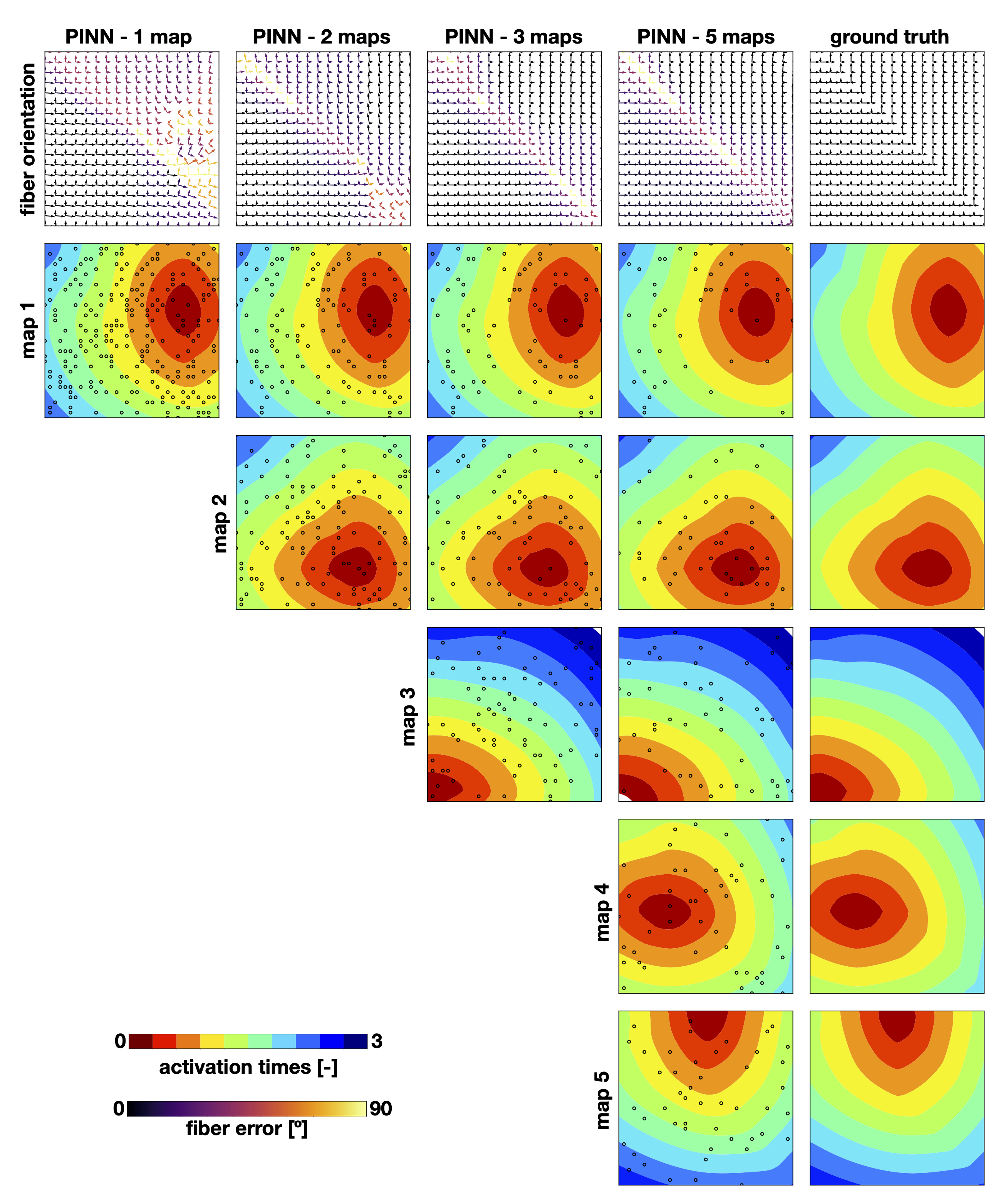
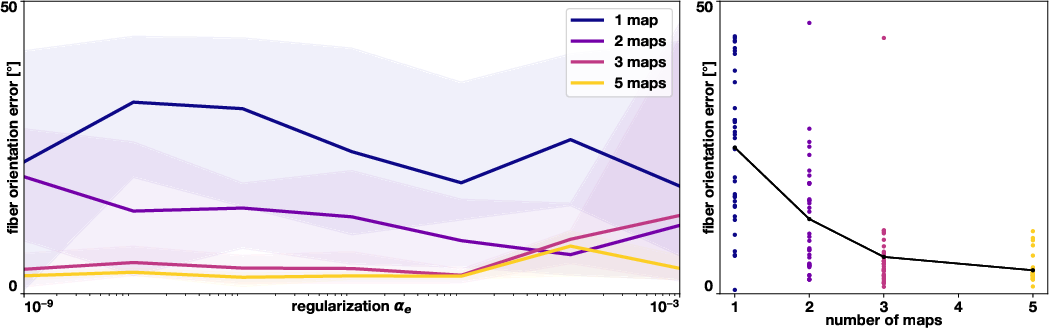
On both controlled grids and anatomically-realistic left atria, FiberNet demonstrates that precise fiber reconstruction (fiber angle RMSE ∼16∘–23∘) requires a minimum of three independent activation maps; error decreases sublinearly with additional maps. With a single map, high local accuracy for activation times can be achieved, but fiber orientation becomes nearly indeterminate except with strong regularization, introducing prior bias.
Figure 4: Activation times simulated in the 2D synthetic testbed, demonstrating the effect of varying the number of maps on prediction and fiber orientation accuracy.
Sensitivity to Regularization
Increasing total variation weights on the conduction tensor (parameter αe) reduces overfitting in low-data regimes, especially in noisy observations, but can lead to over-smoothing and the loss of genuine local heterogeneity as the number of data-rich, independent maps increases.
Figure 5: Sensitivity of fiber orientation error to regularization parameter αe for 2D geometries, highlighting the regime where gains are saturated by increasing the number of maps.
Application to DT-MRI Atlas and Patient Data
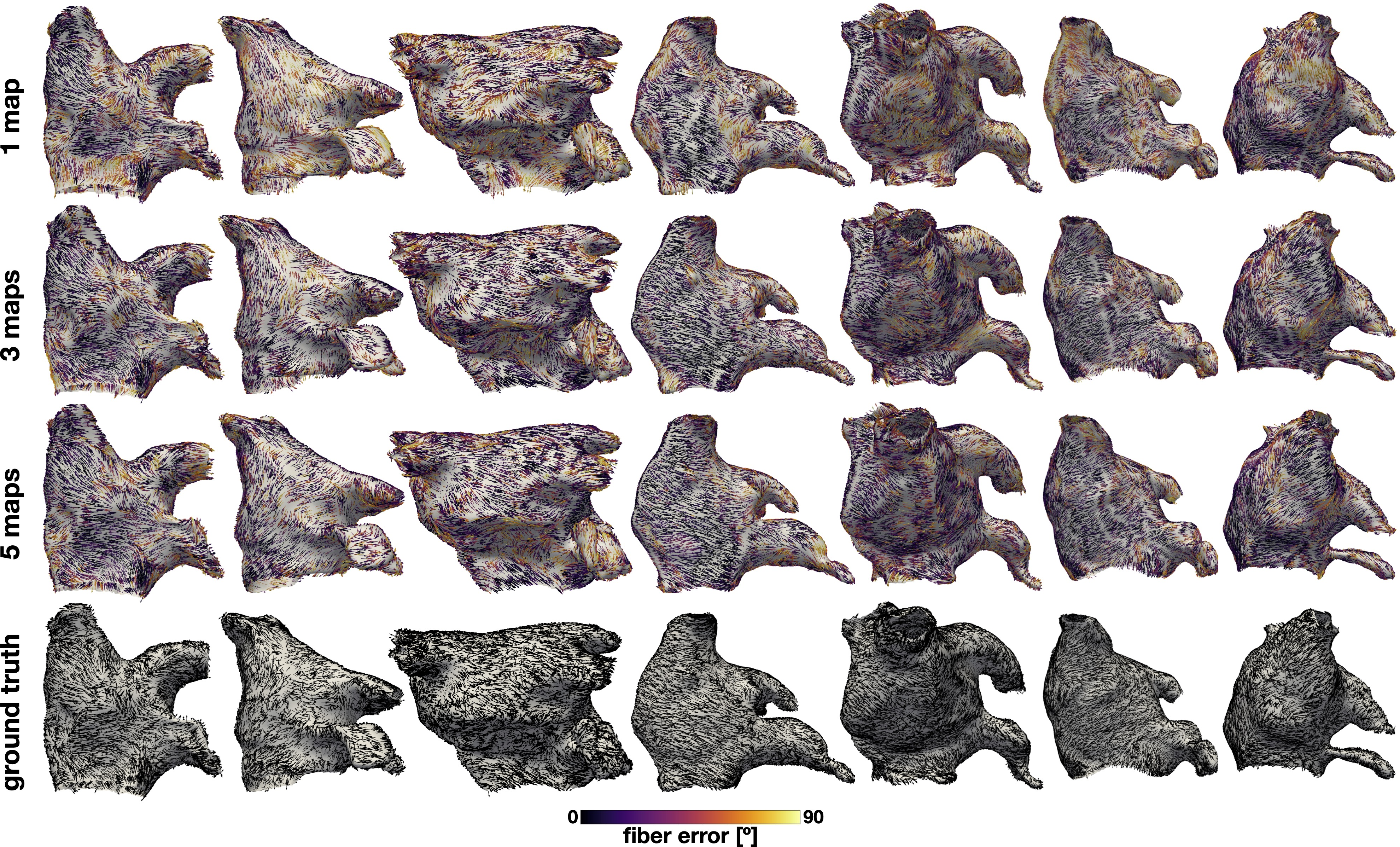
Inferential performance is validated on ex-vivo human DT-MR-derived fiber fields, where ground truth is available. FiberNet consistently reconstructs micro-anatomical fiber discontinuities and recapitulates both global and regional anisotropy. The method maintains robust predictive capacity under moderate noise, with fiber direction RMSE increasing ∼13∘ under 1 ms activation noise and maintaining errors <25∘ when using three or more maps.
Figure 6: Fiber predictions on diffusion tensor fibers for 7 left atrial geometries using 1, 3, and 5 maps. Error magnitude and regional mapping fidelity are visualized spatially.
Forward Extrapolation and Generalization
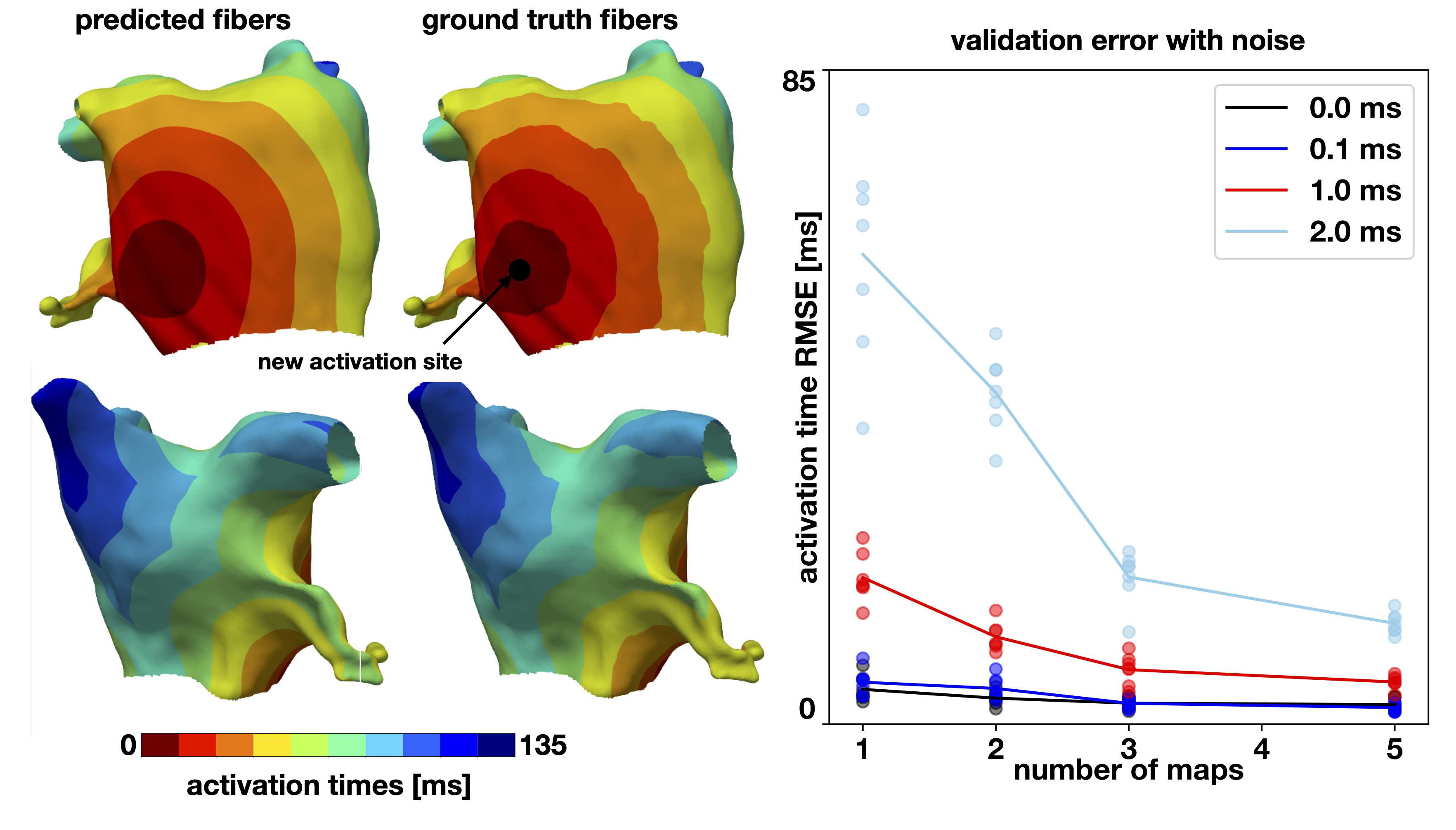
Trained FiberNet models predict unseen activation maps (initiated from stimulation sites not present in training data) with RMS errors routinely below 5 ms, demonstrating the model’s validity as a surrogate for digital twin–based forward modeling.
Figure 7: Exemplar validation on left atrial geometry: predicted activation pattern for an unseen stimulus (separate from all training maps), compared to ground truth.
Clinical Feasibility
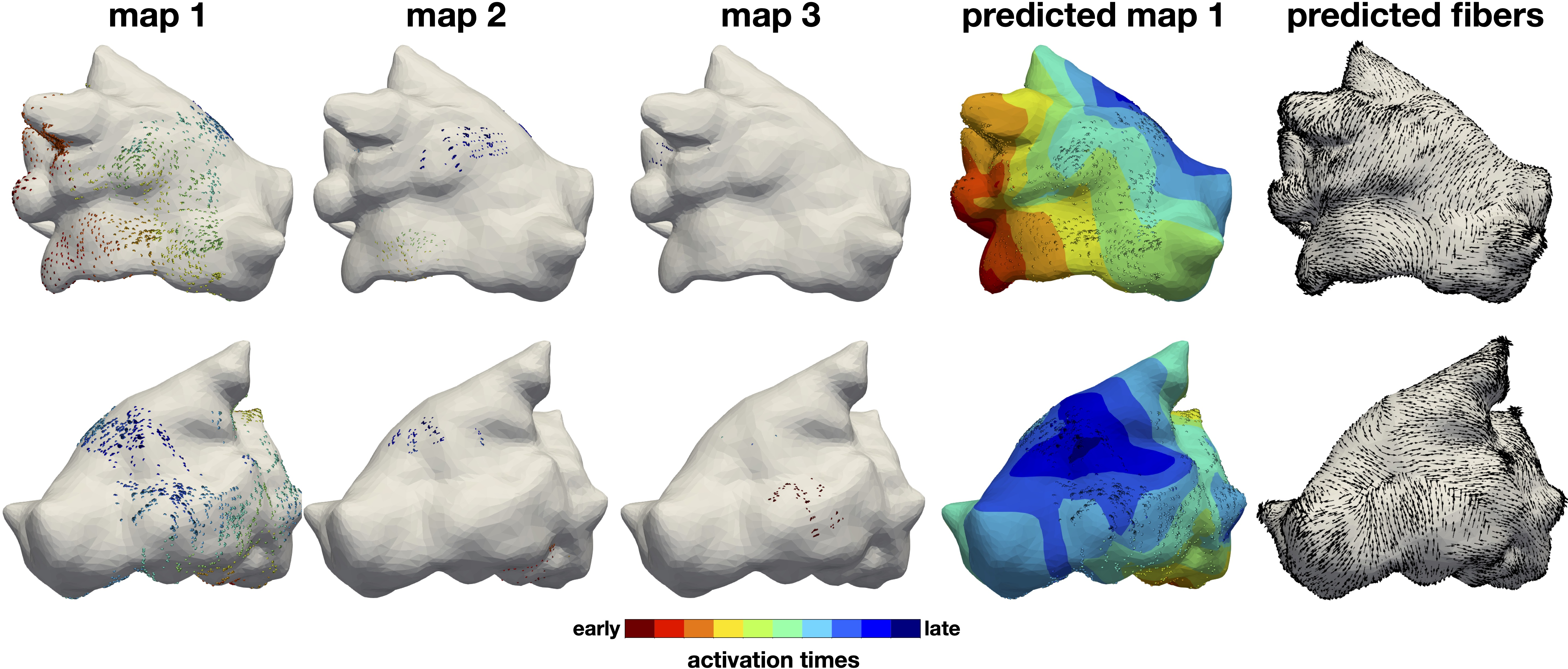
Experiments with in-vivo, patient-derived electroanatomical mapping sets demonstrate that FiberNet can infer physiologically plausible atrial fiber patterns and reconstruct activation with sub-3 ms RMS error, despite highly sparse and spatially non-uniform data. Predicted fibers in these cases align with known anatomical fiber tracts—roof, posterior wall, and annulus-aligned bundles—though ground truth cannot be independently validated in-vivo due to limitations of existing imaging modalities.
Figure 8: Patient-specific application—recorded data points, fitted activation maps, and predicted fiber orientations demonstrating the practical feasibility of clinical deployment.
Theoretical and Practical Implications
Generalizability and Model Bias
The study exposes the trade-off between data completeness vs. regularization priors in physics-constrained inverse learning for medical imaging. Unique and reliable conductivity/fiber inference critically depends on incorporation of sufficient independent data, with regularization partially mitigating but not fully resolving ambiguity in underdetermined regimes.
Technical Considerations
PINNs enable mesh-free parameterization, simplifying geometry handling and facilitating application to arbitrary surfaces without expensive mesh adaptation.
Training time is presently on the order of an hour on commodity CPUs, with convergence behavior robust to hyperparameter selection; prospects for GPU acceleration or transfer learning–based pretraining are strong and not fully explored in this work.
The current formulation is surface-based and most direct for applications in the atria; handling transmural fiber rotation and volumetric bodies (ventricles) would require architectural extensions and augmented clinical datasets.
Perspectives and Future Directions
FiberNet has immediate translational potential in digital twinning workflows, enabling fast, patient-specific characterization of atrial anisotropy for electrophysiological procedure planning, risk stratification, or post-ablation assessment. The method suggests a route to reduce uncertainty in activation modeling where histological or ex-vivo fiber imaging is infeasible. Notably:
Application during arrhythmia states such as atrial fibrillation requires modifications to handle dynamic beat-to-beat variability.
Integration with Bayesian models and hybrid PINN/Gaussian process methods may enable explicit quantification of uncertainty in fiber field estimation, guiding data acquisition and point selection in future catheter mapping.
Extension to solid, transmural myocardium will necessitate incorporating multiple layers of observational constraints, potentially combining surface signals, body-surface ECG, and advanced imaging priors.
Conclusion
FiberNet establishes a well-posed, robust, and versatile framework for inferring cardiac fiber orientation from clinical electroanatomical mapping, overcoming the ill-posedness of classical local methods in anisotropic conductivity inference by leveraging the eikonal constraint and PINN-based global fitting. The demonstrated improvements in fiber inference fidelity and predictive capability with increasing numbers of independent activation maps provide both guidance for clinical data acquisition strategies and a technical foundation for integration in future digital twin platforms and model-driven decision support systems.
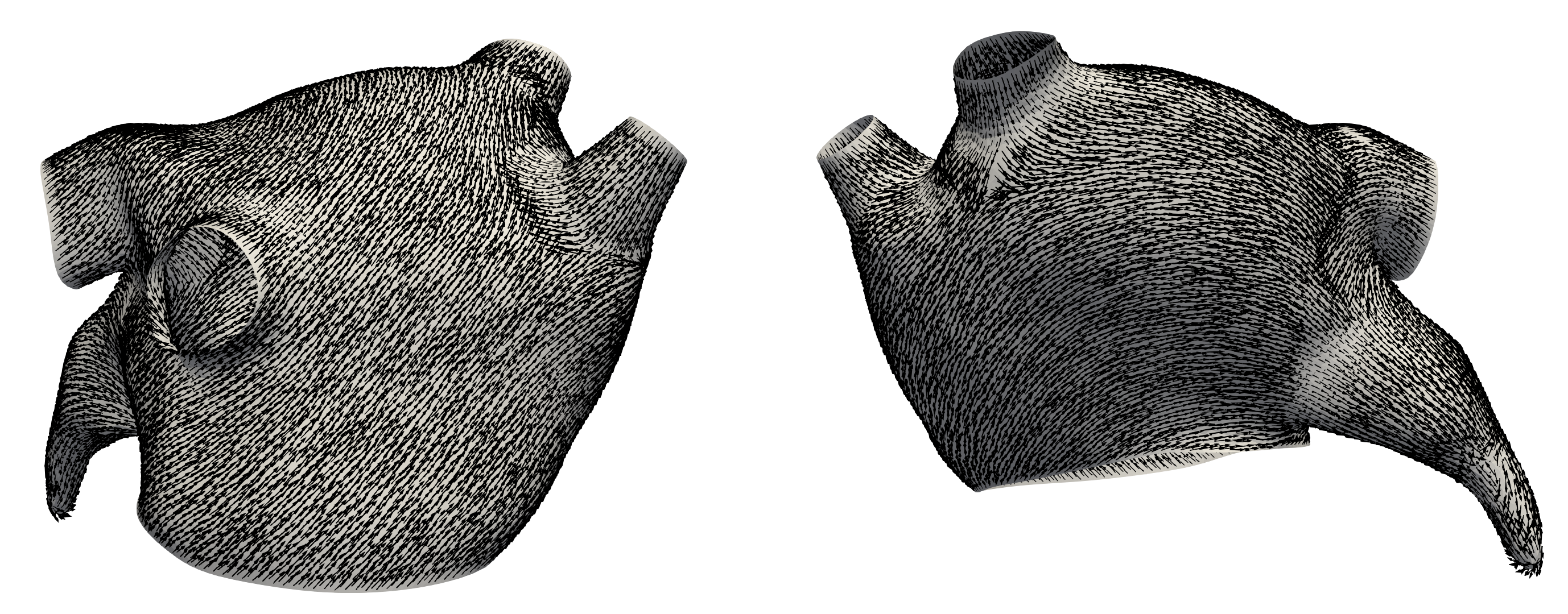
Figure 9: Transport and parallelization of a fiber vector along the atrial manifold, illustrating a smooth basis field except in regions of high geometric curvature.